Craig T. Basson, MD, PhD
- Gladys and Roland Harriman Professor of Medicine
- Director, Cardiovascular Research, Cardiology Division
- Weill Medical College of Cornell University
- New York, New York
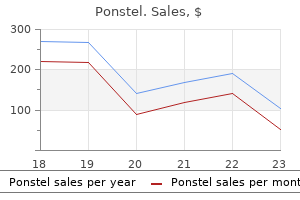
Ponstel dosages: 500 mg, 250 mg
Ponstel packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Purchase ponstel with visa
Although buprenorphine–naloxone seems to be more efficient than clonidine in reducing opioid withdrawal symptoms during the initial course of detoxification differences may wane after a few days [98] spasms colon buy discount ponstel on line. Proponents of this approach emphasize the shortened period of withdrawal associated with the addition of naltrexone spasms all over body generic 250 mg ponstel with visa. Continuing naltrexone as deterrent therapy after opioid withdrawal (akin to the use of disulfiram with alcoholics) has also been advocated muscle relaxant magnesium generic 250 mg ponstel otc, but this approach has a high attrition rate. Administering high doses of opioid antagonists to addicted individuals while under anesthesia has been suggested as a method of achieving detoxification from opiates within 24 to 48 hours. This method, known as ultrarapid detoxification, has been associated with pulmonary and renal failure as well as other complications, including death. Additionally, long- term follow-up has demonstrated relapse of drug abuse in many of these patients [99]. Tobacco exposure is a major risk factor for multiple respiratory, cardiovascular and infectious diseases, as well as carcinogenic. Symptoms generally begin 1 to 2 days after last use, peak within the first week, and persist for 2 to 4 weeks or longer with cravings lasting up to 6 weeks [101]. Nicotine replacement can be used to prevent withdrawal or alleviate symptoms with transdermal nicotine patches to reduce symptoms. Recent studies have evaluated mortality in association with nicotine replacement but are limited by their small size. The only prospective evaluation demonstrated no difference in mortality, length of stay or ventilator use in smokers receiving nicotine replacement versus those not receiving replacement therapy [102]. Bupropion, a long-acting serotonin and norepinephrine reuptake inhibitor, may be used at low doses alone or in combination with nicotine replacement to assist with smoking cessation. Varenicline is a α4β2 nicotinic receptor partial agonist that has also been used for smoking cessation. Clinical studies regarding the roles of bupropion and varenicline for critically ill adults are lacking [101]. Sano H, Suzuki Y, Ohara K, et al: Circadian variation in plasma homovanillic acid level during and after alcohol withdrawal in alcoholic patients. Monte R, Rabunal R, Casariego E, et al: Analysis of the factors determining survival of alcoholic withdrawal syndrome patients in a general hospital. Ramanujam R, L P, G S, et al: A comparative study of the clinical efficacy and safety of Lorazepam and chlordiazepoxide in alcohol dependence syndrome. American Society of Addiction Medicine Working Group on Pharmacological Management of Alcohol Withdrawal. Darrouj J, Puri N, Prince E, et al: Dexmedetomidine infusion as adjunctive therapy to benzodiazepines for acute alcohol withdrawal. Adinoff B: Double-blind study of alprazolam, diazepam, clonidine, and placebo in the alcohol withdrawal syndrome: preliminary findings. Rosenbaum M, McCarty T: Alcohol prescription by surgeons in the prevention and treatment of delirium tremens: historic and current practice. Addolorato G, Leggio L, Abenavoli L, et al: Baclofen in the treatment of alcohol withdrawal syndrome: a comparative study vs diazepam. Miotto K, Darakjian J, Basch J, et al: Gamma-hydroxybutyric acid: patterns of use, effects and withdrawal. Stetkarova I, Brabec K, Vasko P, et al: Intrathecal baclofen in spinal spasticity: frequency and severity of withdrawal syndrome. Amato L, Davoli M, Minozzi S, et al: Methadone at tapered doses for the management of opioid withdrawal. Faggiano F, Vigna-Taglianti F, Versino E, et al: Methadone maintenance at different dosages for opioid dependence. Lintzeris N, Bell J, Bammer G, et al: A randomized controlled trial of buprenorphine in the management of short-term ambulatory heroin withdrawal. Ling W, Amass L, Shoptaw S, et al: A multi-center randomized trial of buprenorphine-naloxone versus clonidine for opioid detoxification: findings from the National Institute on Drug Abuse Clinical Trials Network. In the setting of a large-scale disaster, ambulances will routinely transport critically ill or injured patients to the nearest hospital, often independently of a given hospital’s stated capabilities.
Syndromes
- Renal arteriography
- Do not drink alcohol.
- Drainage from the ear
- Calcium
- Bleeding from the biopsy site
- Multiple myeloma
- Low blood pressure
Purchase ponstel 250 mg with mastercard
Imaging immediately post-arrest it is less likely to help with prognosis muscle relaxant spray cheap ponstel 500 mg amex, unless there is evidence of hemorrhage muscle relaxant with painkiller purchase generic ponstel line, trauma spasms rectum buy 250 mg ponstel visa, or herniation. As a result, they are not recommended for use in isolation and should only be used as supportive information in combination with other tests and clinical findings [3]. In general, a combination of certain diagnostic testing can help to increase the specificity for a poor neurologic prognosis [50]. Rarely will one test be the deciding factor in prognosis; rather, the integration of all testing, combined with the patient’s age and co morbidities, will allow a multidisciplinary team to provide the most appropriate prognosis for patients. Only through team-based care at centers with resources and experience can the most contemporary treatments be delivered. Cronier P, Vignon P, Bouferrache K, et al: Impact of routine percutaneous coronary intervention after out-of-hospital cardiac arrest due to ventricular fibrillation. Bro-Jeppesen J, Kjaergaard J, Wanscher M, et al: Emergency coronary angiography in comatose cardiac arrest patients: do real-life experiences support the guidelines? Aurore A, Jabre P, Liot P, et al: Predictive factors for positive coronary angiography in out-of-hospital cardiac arrest patients. Tømte O, Andersen GØ, Jacobsen D, et al: Strong and weak aspects of an established post-resuscitation treatment protocol-A five-year observational study. Zanuttini D, Armellini I, Nucifora G, et al: Impact of emergency coronary angiography on in-hospital outcome of unconscious survivors after out-of-hospital cardiac arrest. Sunde K, Pytte M, Jacobsen D, et al: Implementation of a standardised treatment protocol for post resuscitation care after out-of-hospital cardiac arrest. Bouzat P, Suys T, Sala N, et al: Effect of moderate hyperventilation and induced hypertension on cerebral tissue oxygenation after cardiac arrest and therapeutic hypothermia. Laver S, Farrow C, Turner D, et al: Mode of death after admission to an intensive care unit following cardiac arrest. Hypothermia after Cardiac Arrest Study Group: Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. Nielsen N, Wetterslev J, Cronberg T, et al: Targeted temperature management at 33°C versus 36°C after cardiac arrest. Kim F, Nichol G, Maynard C, et al: Effect of prehospital induction of mild hypothermia on survival and neurological status among adults with cardiac arrest: a randomized clinical trial. Salinas P, Lopez-de-Sa E, Pena-Conde L, et al: Electrocardiographic changes during induced therapeutic hypothermia in comatose survivors after cardiac arrest. Bro-Jeppesen J, Hassager C, Wanscher M, et al: Targeted temperature management at 33°C versus 36°C and impact on systemic vascular resistance and myocardial function after out-of-hospital cardiac arrest: a sub-study of the Target Temperature Management Trial. The driver of this increase includes a larger burden of cardiac dysfunction related to the aging of the general population, expanding indications for device therapy, and ongoing innovation of the technology for cardiac pacing and defibrillation. This chapter aims to briefly review basic cardiac device function and programming with emphasis on device malfunction and troubleshooting. A discussion of the indications for permanent pacing, defibrillator, or resynchronization therapy is beyond the scope of this text; for additional information regarding these topics, the reader is referred to the American College of Cardiology/American Heart Association/Heart Rhythm Society 2012 Focused Update of the 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities [1]. Substantial device information can be gleaned from a chest radiograph, including the lead configuration, the type of device, abnormalities of lead position or integrity, and even the device manufacturer. Identification of the device manufacturer is essential when formal device interrogation or reprogramming is planned as each device company uses different software and programs to communicate with their respective devices. The overwhelming majority of devices implanted are manufactured by 1 of 3 companies, and patient device information and technical support are available 24 hours a day (Table 196. Pacing nomenclature is standardized to easily communicate information regarding the device and the pacing mode (Table 196. A pacemaker operates like a timer with programmable intervals to coordinate all sensed and paced events. Dual chamber devices programmed to a tracking mode can provide pacing at the programmed lower rate or track sensed intrinsic conduction up to a programmed upper rate limit. Application of a magnet to a pacemaker will cause the reed switch to close and result in asynchronous pacing.
Ponstel 500 mg buy otc
It is preferable to take a patient‐centred increased duration of bleeding spasms from anxiety cheap 500 mg ponstel with visa, and (iv) decreased parity approach to endometriosis muscle relaxant education order 500 mg ponstel mastercard, with a focus on patient‐cen- [6] spasms near heart purchase discount ponstel line. In addition, endometriosis is found more commonly tred outcomes, rather than the lesion‐based approach on the left side of the pelvis, thought to be due to the cleft that has been the hallmark of much clinical research in created by the sigmoid colon’s peritoneal reflections. However, Sampson’s theory does not explain all endome- Endometriosis affects approximately 176 million triosis since it can occur before menarche, in women with women of reproductive age worldwide [2]. While its amenorrhoea, despite menstrual suppression, at the underlying cause is uncertain, it is likely to be multifacto- umbilicus, and (incredibly rarely) in men. Hence the the- rial including genetic factors with epigenetic influences, ory of coelomic metaplasia, the pluripotential of coelomic and perhaps promoted through environmental expo- epithelium to develop not only into the more appropriate sures [3]. Endometriosis has elements of a pain syndrome normal tissue but also, through a programming defect, with central neurological sensitization [4], and is a prolif- into endometriotic tissue. Furthermore, despite the ubiq- erative, oestrogen‐dependent disorder with growing evi- uitous occurrence of retrograde menstruation, which dence of progesterone resistance [4]. There is overlap gynaecologists often view at the time of laparoscopy dur- with other conditions characterized by pelvic/abdominal ing menses, endometriosis occurs only in a minority of pain and infertility. Some symptomatic women with pel- women, and this is explained by the third theory, the con- vic pain who do not have diagnosed endometriosis may tribution of immunologic surveillance defects (which also benefit from similar treatments. The expression of factors such as cell adhesion molecules, proteolytic enzymes and cytokines affecting the adherence, implantation and pro- Epidemiology liferation of tissue within the peritoneal cavity may differ between women, as may clearance of endometrial cells Aetiology from the pelvis, and altered systemic humoral immunity the oldest proposal for the formation of endometriosis is (altered B‐cell function and antibody production) has Sampson’s theory of retrograde menstruation [5] or, more also been implicated. It is unclear whether such abnor- aptly, retrograde passage and implantation of endome- malities are truly a cause or a result of the disease. Menstrual material containing viable cells is embolic transport of endometrial cells through the blood transported into the peritoneal cavity in a retrograde and lymphatic stream may contribute to the very rare Dewhurst’s Textbook of Obstetrics & Gynaecology, Ninth Edition. One of the most appealing environ- pelvis, including lungs, brain and nasal tissues (responsi- mental exposure theories, that the environmental pollut- ble for the rare case reports, so loved by journal editors, ant dioxin might be an underlying cause of the disease [9], of catamenial pneumothorax and haemoptysis, catame- was ultimately difficult to confirm. The currently recognized nine endometriosis first‐degree relatives of affected women than in controls; gemetic loci explain only 3. Endometriosis is inherited as a complex genetic Prevalence trait, similar to diabetes or asthma, meaning that a number of genes interact to confer disease susceptibility, but the the prevalence is estimated to be 8–10% in women in phenotype probably only emerges in the presence of envi- the reproductive years [6]. Natural history of endometriosis [16], symptoms of endometriosis may also persist after and associated comorbidities natural or surgical menopause. Evidence is emerging regarding lescents with suggestive symptoms; in fact most women comorbidity for women with endometriosis. There may with endometriosis date the onset of symptoms to their be subtle associations with ovarian and breast cancers, teens [15]. Women with endometriosis appear to have a cutaneous melanoma, asthma and some autoimmune, higher risk of obstetric complications, including preterm cardiovascular and atopic diseases, and women with delivery, antepartum haemorrhage, pre‐eclampsia and endometriosis appear to be at decreased risk of cervical need for caesarean section, with rare occurrences of cancer [17]. Endometriosis has been recently shown to intra‐abdominal bleeding from endometriotic lesions have a significant association with coronary heart dis- requiring urgent surgery [1]. There with endometriosis become pain‐free after menopause is an association between endometriosis and clear‐cell, Endometriosis 725 low‐grade serous and endometrioid ovarian cancer [19], Peritoneal (or typical) endometriosis but the overall risk of ovarian cancer among women with Peritoneal endometriosis comprises superficial lesions endometriosis remains low, with a relative risk ranging scattered over the peritoneal, serosal and ovarian sur- from 1. The appearance has been described as ‘powder‐ time risk of ovarian cancer of no more than 1 in 100, burn’ or ‘gunshot’ deposits. Much more rarely, endometriosis may Cystic ovarian endometriosis present as an invasive disease while remaining histologi- (endometriomas) cally benign, with ascites, sometimes even pleural effu- Endometriomas develop as cystic lesions within the sions, and invasive lesions affecting not only the pelvis ovary, classically forming ‘chocolate cysts’ due to the deg- but also the diaphragm, bowel and abdominal side‐walls, radation of blood over time to a thick haemosiderin‐rich and thus may be impossible to distinguish clinically and fluid. Several variants on the implantation and metapla- on imaging from intra‐abdominal malignancy. Thus, it has been suggested that super- ficial lesions on the ovarian cortex become inverted and Endometriosis phenotypes at invaginated, and that endometriomas are derived from laparoscopy functional ovarian cysts or metaplasia of the coelomic epithelium covering the ovary. Endometriomas have fea- Although a stronger focus on the symptoms experienced tures in common with neoplasia such as clonal prolifera- by women and their outcomes is currently needed, it is tion, which is consistent with the endometriosis disease also important to retain an understanding of endome- theory. They are statistically associated with subtypes of triosis lesions, as this features prominently in the litera- ovarian malignancy, such as endometrioid and clear‐cell ture. However, it still remains uncertain whether lesions that are not absolutely typical often remain unrec- such cancers arise from malignant transformation of ognized by less experienced laparoscopists. Images (a), (b), (d) and (e) kindly contributed by Dr Michael East, Gynaecologist, Oxford Women’s Health, Christchurch, New Zealand. The ‘most subtle’ of all endometriotic lesions would be microscopic endo- Now defined as lesions extending deeper than 5mm metriosis [26], in other words the histological finding of under the peritoneal surface or those involving or dis- endometriosis in macroscopically normal peritoneum.
Ponstel 250 mg buy with amex
Campers must aggressively sterilize drinking water from mountain streams to prevent this common infection muscle relaxant drug list ponstel 250 mg buy amex. Giardia can also be transmitted from person to person in daycare centers and other confining institutions muscle relaxant methocarbamol cheap 250 mg ponstel with visa. This pathogen also has been spread from person to person by sexually active homosexuals muscle relaxant erectile dysfunction cheap ponstel 250 mg on-line. Clinical Manifestations, Diagnosis, and Treatment A patient with this parasite usually has only mild symptoms or is asymptomatic. Adults may complain of abdominal cramps, bloating, diarrhea, anorexia, nausea, and malaise. Chronic disease is less common and results in malabsorption, chronic diarrhea, and weight loss. A diagnosis of giardiasis should be considered in all patients with prolonged diarrhea. Examination of cysts using concentration techniques has a 90% yield after three stool samples. Endoscopy and duodenal biopsy, or duodenal aspiration, are no longer necessary in most cases. Oral metronidazole (250 mg every 8 hours for 5-7 days), tinidazole (2 g as a single dose), or nitazoxanide (500 mg q12h × 3 days) is the treatment of choice (see Table 8. Clinical manifestations are usually mild; the disease is self-limiting, 4- 6 weeks. Diagnosis: a) Stool smear shows no polymorphonuclear leukocytes; cysts are seen in 90% of cases after three stool examinations. Autoinfection can also occur, explaining how ingestion of small numbers of oocysts can cause severe, persistent infection in the immunocompromised host. Cryptosporidium is classified as an intestinal coccidian; it is related to malarial organisms. The mechanisms by which Cryptosporidium causes diarrhea are not completely understood. The pathogen affects intestinal ion transport and causes inflammatory damage to the intestinal microvilli, resulting in malabsorption. This parasite is carried in the intestinal tract of many animals and is also found in water. The oocyst is resistant to chlorination, and large outbreaks resulting from contaminated drinking water supplies have been reported. Infection can also be transmitted in contaminated swimming pools, and an outbreak in a water park has been described. Person-to-person spread has also been reported and can occur in households or in institutional settings such as daycare centers and hospitals. With increased globalization of the food supply, Cyclospora is likely to become an increasing problem. An outbreak in the United States was associated with Guatemalan raspberries and this parasite can contaminate fresh vegetables and fruits. The obligate intracellular parasite known as Microsporidium is very small in compared with the other parasites that cause diarrhea (ure 8. It infects mucosal epithelial cells, causing villous atrophy, and may ascend into the biliary tract to cause cholangitis. The diagnosis is made by demonstrating the organisms in stool or after intestinal biopsy. Children and immunocompetent adults can develop symptomatic cryptosporidiosis, and acute disease may be followed by chronic intestinal symptoms associated with fatigue, headaches, eye, and joint pains. Stool samples should be stained not only with iodine but also with modified Kinyoun acid-fast stain, and concentrated. Cryptosporidium is acid-fast; however, fecal smears have proved less specific and sensitive than fecal antigen tests that are now commercially available. Cyclospora oocysts can also be detected in the stool by modified acid-fast staining (8-10 microns in diameter). It is important to differentiate them from Cryptosporidium oocysts that are smaller (5 microns in diameter. In addition to being acid-fast, they demonstrate blue autofluorescence when observed under a fluorescence microscope with a 330-380 nm ultraviolet filter.
Generic ponstel 500 mg buy on-line
The test takes only 15 minutes back spasms 6 weeks pregnant cheap ponstel 250 mg otc, and allows inexperienced caregivers to rapidly institute appropriate therapy spasms sphincter of oddi purchase ponstel paypal. The focus must be on differentiating falciparum malaria from other forms of the disease spasms down there purchase 250 mg ponstel visa. In falciparum malaria, signet-ring forms are most abundant on peripheral smear immediately after a fever spike 3. An immunochromatographic lateral flow rapid diagnostic test is now commercially available that detects P. Polymerase chain reaction methods have been developed but are not commercially available. An elevated unconjugated bilirubin level without a significant increase in hepatic enzymes is also observed when hemolysis is severe. Elevated serum creatinine, proteinuria, and hemoglobinuria are found in severe cases of P. Prophylaxis and Treatment Drug treatment exploits unique targets in the parasite not found in host cells. The aminoquinolines, chloroquine, quinine, mefloquine, primaquine, and halofantrine inhibit proteolysis of hemoglobin in the food vacuole and inhibit the heme polymerase that Plasmodium requires for production of malaria pigment. Artemisinin derivatives bind iron in the malarial pigment to produce free radicals that damage parasite proteins. These derivatives are faster-acting than quinine, and they have activity against all stages of the intraerythrocytic life cycle. In recent years, many areas of Africa, northern South America, India, and Southeast Asia have become populated with chloroquine-resistant P. These strains contain an energy-dependent chloroquine efflux mechanism that prevents the drug from concentrating in the parasite. Resistance to mefloquine and halofantrine has also developed, being seen primarily in Southeast Asia. Chemoprophylaxis should start 2 weeks before departure to an endemic area when taking chloroquine and mefloquine, and 1-2 days before travel for atovaquone–proguanil as well as doxycycline. Prophylaxis should be continued for 4 weeks after return if taking chloroquine and mefloquine and for 7 days if taking atovaquone-proguanil or doxycycline. The adult dosage is 300 mg base (500 mg of chloroquine phosphate) orally once per week. In areas of chloroquine-resistance, atovaquone–proguanil (atova-quone 250 mg combined with proguanil 100 mg, the combination tablet is called Malarone) orally once per day, mefloquine 250 mg (228 mg base) orally once per week, or doxycycline 100 mg orally once per day. Mefloquine should be avoided in individuals with psychiatric disorders, seizure disorders, or cardiac conduction abnormalities. Determine if the traveler will be visiting areas with chloroquine-resistant strains (check www. Begin prophylaxis 2 weeks or 1-2 days before travel (depending on the medication). Atovaquone-proguanil, doxycycline, or mefloquine recommended for chloroquine-resistant areas. All individuals without previous immunity who contract falciparum malaria should be hospitalized, because their clinical course can be unpredictable. This agent kills dormant hepatic hypnozoites, preventing their subsequent development into infective schizonts. Before the primaquine is administered, the patient should be tested for glucose-6- phosphate dehydrogenase deficiency, because patients with this deficiency are at risk of severe hemolysis during primaquine treatment. Given the worldwide prevalence of chloroquine resistance, unless absolute assurance can be obtained that travel was only in regions with chloroquine- sensitive P. Artemisinin derivatives have shown superior efficacy for severe chloroquine-resistant P. Their use therefore decreases infectivity after treatment, and can eliminate malaria transmission in endemic areas. The first dose should be followed by a second dose 8 hours later, then 1 dose twice a day for the next 2 days. Artesunates are short-acting, and they should always be combined with one or more other classes of antimalarial agents such as lumefantrine, pyronaridine, atovaquoneproguanil or mefloquine to prevent the development of resistance. Determine whether the traveler came from a chloroquine-resistant area: a) For chloroquine-sensitive strains, use chloroquine. Determine whether the patient is too ill to take oral medicines (requires intravenous quinidine).
American White Hellebore (American Hellebore). Ponstel.
- How does American Hellebore work?
- Epilepsy, spasms, water-retention, nervousness, fever, high blood pressure, and other conditions.
- Are there safety concerns?
- Dosing considerations for American Hellebore.
- What is American Hellebore?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96798
Cheap ponstel 250 mg without prescription
The posterior suture line is continued onto the ascending aorta spasms muscle pain ponstel 250 mg buy lowest price, stopping 5 mm above the proximal extent of the incision infantile spasms 8 months 500 mg ponstel mastercard. The anterior suture line is accomplished with the other needle infantile spasms 6 months old buy cheap ponstel on line, again ending the suture line 5 mm short of the proximal ascending aortic opening. Patch Material A patch cut from an adult-sized pulmonary homograft has a natural curved shape, which mimics the curve of the underside of the aortic arch. However, there are availability and cost issues, as well as concerns regarding viral transmission and the generation of cytotoxic antibodies, which may limit transplant options. Some surgeons have advocated the use of bovine pericardium or other substitutes, using two pieces cut in a curved shape and sewn together along their concave aspect to create an appropriately shaped aortic arch patch. Suturing along Arch Alternating traction on the left carotid tourniquet and the innominate artery tourniquet improves the exposure for performing the posterior and anterior suture line on the underside of the aortic arch. The main pulmonary artery is anastomosed to the ascending aorta, taking care not to distort the aortic root. This is accomplished with multiple interrupted 7-0 Prolene sutures to avoid “purse-stringing” of the opening into the aortic root. This interrupted suture line is carried up to meet the suture lines connecting the ascending aorta to the pulmonary homograft patch. The pulmonary homograft patch and base of the pulmonary artery are pulled upward, and the patch trimmed to create an appropriate hood. Compression of Pulmonary Artery by Neoaorta the homograft patch must not be too large or left too long because it may compress the central pulmonary artery. Pulmonary homograft tissue is fairly distensible, and this must be taken into consideration when fashioning the patch. Inset: Distortion of proximal aorta by inaccurate alignment of proximal pulmonary artery to aortic opening or purse-stringing of anastomosis. Damus Modification In some patients, most notably those with double inlet left ventricle, or those with double outlet right ventricle and mitral valve atresia, it is preferable to perform a modified Blalock-Taussig shunt, so as to eliminate the need for a left ventriculotomy, and also for ease because of the size of the reconstructed great vessel. Coronary Artery Compromise Meticulous technique must be used when anastomosing a small ascending aorta to the proximal portion of the pulmonary artery to avoid obstructing flow into the coronary arteries. Some advocate an incision into the sinus of the pulmonary valve so as to increase the area of connection between the diminutive aorta and the pulmonary artery. Modified Patch Technique Some surgeons use a homograft patch to enlarge the entire opening beginning in the descending aorta, across the aortic arch, and down the ascending aorta to just above the sinotubular junction. An incision is made in the patch under the aortic arch, and the pulmonary base is anastomosed to this opening. A disadvantage of this technique is the lack of growth potential of the homograft patch, which is circumferentially attached to the pulmonary base. The innominate, left carotid, and left subclavian arteries are snared down during low-flow cerebral perfusion. The opening is carried proximally along the inferior aspect of the aortic arch to the level of the innominate artery. The distal opening may be connected to the incision on the inferior aspect of the aortic arch (dotted line). Small Ascending Aorta If the ascending aorta is less than 3 to 4 mm in diameter, it is transected distally near the takeoff of the innominate artery and the distal opening is connected to the aortic arch incision or is closed with a separate running suture. If the main pulmonary artery is of good length, it can be anastomosed directly into the opening on the aortic arch with no patch material. The suture line is begun at the distal opening on the descending aorta using double-armed 7-0 Prolene suture. The needle is first passed from inside to outside on the pulmonary artery base and then outside to inside on the aorta. The second needle is used to complete the suture line anteriorly starting inside to outside on the descending aorta and continuing along the arch until the first suture line is met. Inadequate Mobilization of the Descending Aorta the descending aorta must be aggressively mobilized at least 1 cm beyond the ductal insertion to allow a tension-free anastomosis. The curved clamp placed on the descending aorta helps to hold it in place and provides improved exposure for the distal extent of the anastomosis. Inadequate Length of the Main Pulmonary Artery the takeoff of the right pulmonary artery is variable in its proximity to the pulmonary valve. When it is located more proximally, the transected main pulmonary artery may not be long enough to reach the aortic arch. A rectangular or oval piece of pulmonary homograft is then used to augment the posterior aspect of the opening in the arch and descending aorta.
Buy genuine ponstel online
Magnification of the cardiac silhouette cannot be eliminated because of the short tube–detector distance and the often supine position of the patient muscle relaxant leg cramps generic ponstel 250 mg line. Furthermore muscle relaxant drugs over the counter buy discount ponstel 500 mg on line, the meniscus of a pleural effusion is often not visible using supine or semi-erect radiographic positioning infantile spasms youtube purchase ponstel line. Radiographs are often acquired after a poor inspiratory effort because of the patient’s inability to follow breath-hold instructions. Increased inflation of the lung may cause the opacities to appear less dense, but the apparent improvement secondary to increased aeration does not correspond to a true improvement. This is demonstrated on this anteroposterior portable chest radiograph of a 70-year-old male who is day 2 after uncomplicated mitral valve repair. The first radiograph (A) demonstrates a low lying endotracheal tube tip in the lower trachea (arrow), two satisfactorily positioned right internal jugular venous catheters, intact sternotomy wires, two mediastinal drains, and moderate cardiomegaly. Five hours later (B), the endotracheal tube has been removed because of clinical stability and as a result, lung density increases due to the absence of mechanical ventilation. When the inferior border of the mandible is at or above C4, the tip should be 7 ± 2 cm from the carina. When the inferior border of the mandible is at the C5 to C6 levels, the tip of the tube should be 5 ± 2 cm from the carina. When the inferior border of the mandible is at T1 or below, the tip of the tube should be 3 ± 2 cm from the carina. If, however, the mandible is not visible, and the technologist has ensured that the head is in a neutral position, an endotracheal tube position 5 ± 2 cm from the carina is acceptable. If it is just below the vocal cords, its inflated cuff can cause glottic or subglottic edema, ulceration, and, ultimately, scarring. If it is too low, it can enter a bronchus and cause atelectasis of the lung supplied by the obstructed bronchus. Anteroposterior portable chest radiograph of a 70-year-old male who is day 1 after mitral valve repair. The radiograph demonstrates appropriate endotracheal tube position in the lower trachea 3 cm from the carina (arrow), two satisfactorily positioned right internal jugular venous catheters, intact sternotomy wires, two mediastinal drains, acute perihilar “batwing” opacities indicating pulmonary edema which resolved after diuresis. The radiograph demonstrates the tip of the endotracheal tube in the right main bronchus (arrow), causing right upper lobe atelectasis; in addition, there is complete collapse of the left lung owing to a large pneumothorax which has been treated with emergent left chest tube placement, the tip of which is in satisfactory position. Ideally, the tube should be one-half to two-thirds the width of the trachea, and the inflated cuff should fill the trachea without causing the lateral walls to bulge. Repeated overdistension of the cuff on chest film, despite careful cuff inflation to the minimal leak level may predispose to tracheomalacia. The balloon of the endotracheal tube (arrow) is wider than the transverse diameter of the trachea indicating overdistension. Immediately after intubation, and especially after difficult intubation, an image should be obtained to define the position of the endotracheal tube. The radiologist should also look for signs of perforation of the pharynx, such as new subcutaneous emphysema, pneumomediastinum, and pneumothorax. Dislodging of teeth, dental caps, and portions of dentures into the tracheobronchial tree has been reported after intubation. Unlike the endotracheal tube, the tracheostomy tube does not change position with flexion and extension of the neck. The tracheostomy tube should be evaluated to determine its inner diameter (which should be two-thirds that of the tracheal lumen); its long axis (which should parallel the tracheal lumen); the location of its distal end. Central Venous Catheters Central venous catheters should be evaluated to ensure accurate central venous pressure measurement and central venous drug delivery. The intersection of the bronchus intermedius with the right heart border and the inflection of the right heart border are the closest radiographic landmarks to the cavoatrial junction. When these landmarks are not identifiable, the most uniformly visible radiographic landmark is the carina; the superior cavoatrial junction is approximately 4 cm above this structure. Complications of central venous catheter placement include infection, vascular perforation or dissection, inadvertent arterial cannulation. The junction of the internal jugular and right subclavian veins (long arrow) occurs at approximately the level of the first rib (short arrow).
Ponstel 500 mg buy cheap
Anaphylaxis can be prevented by delaying exercise by at least 2 and preferably 4 hours after eating (48 hours after ingesting a known food cofactor) and stopping exercise at the onset of pruritus spasms ms cheap ponstel online master card. Antihistamines and/or leukotriene modifiers (montelukast spasms due to redundant colon ponstel 250 mg order without prescription, zileuton spasms chest cheap ponstel 500 mg online, and others) are occasionally of benefit in prevention. Idiopathic (Spontaneous) Urticaria/Angioedema/Anaphylaxis A group of patients has been described who experience recurrent anaphylaxis without an identifiable precipitant, the so-called idiopathic anaphylaxis [98]. In these patients, a careful review of all foods, preservatives, and drugs ingested before the episodes, as well as physical factors such as exercise, fails to reveal a cause for recurrent life- threatening anaphylaxis. Idiopathic anaphylaxis is most likely on the spectrum of diseases of excess mast cell activity with resultant signs and symptoms of excess histamine release and its consequences, whether from autoantibodies to the high-affinity IgE receptor on mast cells or other unknown triggers [100,101]. Maintenance therapy is directed at reducing histamine responsiveness as well as oral glucocorticoids, and, in refractory cases, anti-IgE therapy (omalizumab) [102,103]. Second-line additional agents (cyclosporine, dapsone, hydroxychloroquine) have been used in individual patients [104]. Onset of angioedema usually starts within the first several hours or up to a week after beginning therapy, but angioedema can develop after months to years of asymptomatic usage [106]. The mechanism is unknown but is suspected to be related to an alteration in bradykinin metabolism, leading to excess bradykinin and resultant vasodilatation or, possibly, an interaction with components of the complement cascade (e. An important distinguishing feature of bradykinin/complement angioedema is that, as a rule, there is no associated urticaria or pruritus. In general, epinephrine, antihistamines, and systemic glucocorticoids are of minimal benefit, although a few studies have suggested an earlier time to extubation among patients treated with antihistamines. For patients with severe or persistent airway swelling, some studies have reported benefit with agents that are approved for use in hereditary angioedema, such as icatibant (off-label, 30 mg given by slow infusion subcutaneously, may be repeated in 6 hours), fresh frozen plasma (2 units), and purified C1 inhibitor concentrate (off-label, dosing per package insert) [106,108]. The disorder is inherited in an autosomal dominant pattern, but up to 15% of cases are new mutations without ancestral history. Onset of disease is typically in early to late adolescence and is marked with three main types of crises: extremity, facial/airway, and abdominal. Although crises can be spontaneous, trauma is a well-recognized precipitant, specifically for extremity and facial/airway crises. Of particular relevance is the development of facial and airway angioedema within 24 hours after invasive dental work or oral surgery because this can be readily misidentified as local anesthetic allergy since these are usually co-administered in these procedures. Abdominal crises are characterized by subacute or acute onset of crampy abdominal pain associated with nausea and vomiting. Due to bowel wall edema, there is often initial constipation from peristaltic dysfunction, which can be followed by diarrhea. Of note, these patients can present with an acute abdomen and radiographic findings suggestive of ischemic bowel. Careful clinical judgment is needed because episodes are typically self-limited and abdominal surgery, as a traumatic trigger, could further exacerbate visceral angioedema. Diagnostic laboratory evaluation is warranted in patients who present with angioedema without urticaria and no clear trigger, especially if there is suggestive underlying autoimmune or lymphoproliferative disorder. In the absence of ready availability of these agents, 2 units of fresh frozen plasma [110], with the intent to provide functional exogenous C1 esterase inhibitor, can be used, typically to avert the need to establish an emergency airway for severe laryngeal edema. Most patients have either the urticaria/anaphylaxis pattern or the respiratory disease pattern, but a few patients have both. Desensitization protocols for patients with coronary artery disease, who need the antiplatelet effects of aspirin, have been published [116,117]. Miscellaneous Causes of Anaphylaxis Insulin therapy has been associated with an increased risk of anaphylaxis, particularly when a patient on insulin therapy has a history of local wheal-and-flare reactions at the site of insulin injections and interrupts insulin therapy for more than 48 hours and then resumes it [11,118]. If heterologous serum must be used (antitoxin for snake bites, passive rabies immunization in developing countries, and antilymphocytic serum for organ transplantation), patients are usually evaluated for cutaneous sensitivity by first performing a scratch test with antitoxin or normal horse serum. As with all skin testing, the physician must be prepared to treat any systemic reactions that arise [1]. Patients with mastocytosis appear to be at greater risk for developing anaphylaxis from Hymenoptera stings (even in the absence of IgE mediation) and from mast cell degranulating agents (see Table 69. Administration of diagnostic and therapeutic agents that might cause mast cell activation should be avoided in these patients. The quality of evidence and recommendations for diagnosis and management of anaphylaxis are summarized in Table 69.
Cheap ponstel 250 mg buy
The provision of mechanical ventilation is the most common requirement needed to manage critically ill patients with respiratory compromise spasms 14 year old beagle buy ponstel in united states online. The main challenge of providing this important therapeutic modality during a disaster is the availability of mechanical ventilators muscle relaxant high blood pressure purchase ponstel 500 mg. During a major influenza pandemic muscle relaxer z purchase genuine ponstel line, demand for mechanical ventilators in the United States could increase by 60,000, assuming a 30% attack rate and a high case-fatality rate of 0. The United States has approximately 62,000 full-feature ventilators, or 20 of these per 100,000 residents, plus an additional 100,000 ventilators with fewer features but which could be used during a disaster [27]. Thus, in preparing to provide mechanical ventilation to a large number of critically ill disaster casualties, planners need to consider other options, such as high-flow nasal cannula oxygenation or noninvasive positive-pressure ventilation for selected patients. Anesthesia machines and transport ventilators could serve as additional options, although these could be similarly limited by the number of trained personnel and have disadvantages with regard to infection control [29–32]. The provision of critical care during a disaster will also require that a large quantity of supplies and pharmaceuticals be on hand and readily available to critical care providers. The Joint Commission currently requires that accredited hospitals plan for 96 hours of autonomous function, without external resupply, in the event of disaster (although 96 hours of supplies and the ability to function at full capacity are not required). In 2005, during the Hurricane Katrina disaster in New Orleans, the lack of available supplies, pharmaceuticals, and operational equipment forced the dedicated staff at Charity Hospital to improvise critical care practices and deviate from the usual standards of care prior to final evacuation of the hospital [33]. Hospitals in areas affected by the Great East Japan Earthquake and subsequent tsunami of 2011 and by Hurricane Sandy in 2012 showed comparable experiences. In Miyagi Prefecture in Japan, for example, six out of 14 of hospitals had less than 1 day of food on hand at the time of the quake, and another six hospitals had less than 1 day of medical supplies. Just-in-time supply practices at New York City hospitals produced some similar shortages, offset in part by supplies available from elsewhere in the city [34,35]. Shortages of intensivists, critical care nurses, respiratory therapists, critical care pharmacists, and other specially trained personnel may be a limiting factor in caring for large numbers of critically ill patients. In infectious outbreaks or natural disasters, hospital staff may themselves be victims, further decreasing the institution’s ability to respond [36,37]. These recommendations state that experienced providers should perform direct patient care, when feasible. Finally, systematic procedures (such as protocols) should be instituted and understood by all critical care providers, in order to standardize processes, maximize good outcomes, and maximize safety to patients and staff during a disaster. During contigency and crisis surge conditions, intensivists will need to focus part of their effort on supervising cross-trained physicians from other specialties. Nonintensivist physicians who are skilled in proving hands-on care, such as hospitalists, emergency physicians, general surgeons, or anesthesiologists, could be assigned six patients each (assuming that other urgent clinical duties do not take precedence). Intensivists could supervise four to eight such providers, thereby extending their critical care coverage to almost 50 patients. Training for such processes will become necessary for prolonged events that will severely strain staff resources during a major disaster [25,38]. During a major disaster, space limitations may require that critical care be provided in other areas of a hospital [24,39]. In the initial phases of a surge requirement, hospitals should be able to accommodate up to a 20% increase of critically ill patients with minimal impact, assuming that supplies and staff are available and the hospital is not at maximum capacity. As an emergency mass critical care event progresses, formal critical care space will need to expand into other areas of the hospital, with the hospital continuing to make room for critically ill patients by transferring the most stable inpatients elsewhere. Critical care has been provided in such settings before, with recent experience in New York City following the damage to Bellevue Hospital by Hurricane Sandy as well as during humanitarian international missions or military operations [25,40,41]. However, because of the logistical requirements for specialized equipment, infection control support, and the relocation of trained personnel, critical care should only be provided in “field” settings as a last resort. For most major disaster situations, such facilities can be best used for the management of noncritically ill patients who are transferred from hospitals in order to free up space for the management of the critically ill. Critical care providers and institutions should strive to manage resources within their own facility and region with the goal of providing usual critical care practices to the extent possible. However, in a major disaster, because resources become increasingly limited, health care providers and leaders must have a plan in place to change the focus of critical care from the needs of the individual to the needs of the population as a whole. Ethical and Legal Principles Utilitarian principles guide the theory of the “greatest good for the greatest number.

Discount 500 mg ponstel with amex
Esophageal pseudodiverticulum may occur in patients with esophageal stricture as early as 1 week after corrosive ingestions spasms hands fingers buy ponstel 250 mg with amex. It appears to result from incomplete destruction of the esophageal wall and usually resolves with dilation of associated strictures [28] spasms pain rib cage ponstel 500 mg order with visa. Sepsis secondary to perforation is the most common cause of death; severe hemorrhage or aspiration may also contribute [18] spasms definition buy 500 mg ponstel with mastercard. It occurs most commonly at the level of the tracheal bifurcation and is estimated to occur 1,000 times more frequently in patients who have had corrosive injuries than in the general population. Systemic toxicity has occurred with burns caused by arsenic and other heavy metals, cyanide, acetic acid, formic acid, fluoride, hydrazine, hydrochloric acid, nitrates, sulfuric acid, and phosphoric acid [11,30–34]. The anion gap is usually elevated, although a hyperchloremic acidosis may be seen in hydrochloric acid and ammonium chloride ingestion. After hydrochloric acid ingestion, cardiovascular collapse is the most common cause of early death; myocardial infarction has occurred after large ingestions. Other findings associated with severe acid injuries include hemolysis, hemoglobinuria, nephrotoxicity, and pulmonary edema [31,32]. Identification of the compounds involved and any measures required for their safe handling can be established by a number of means: Container labeling, material safety data sheets and safety officers in cases of workplace exposure, fire department hazardous materials units, and regional poison information centers. If the exposure is the result of an industrial or transportation accident, the patient should be evaluated for traumatic injuries. After decontamination, assessment of eye exposures should include measurement of visual acuity and conjunctival pH and a slit-lamp examination. Chemosis, conjunctival hemorrhages, corneal epithelial defects, stromal opacification, and loss of limbic vessels should be noted. If the affected area is greater than 15% of total body surface area or if systemic toxicity is possible, a complete physical examination with appropriate monitoring and laboratory testing should be performed. With ingestions, the ability to swallow secretions and findings on examination of the oropharynx, neck, chest, and abdomen should be noted. Patients with signs and symptoms suggestive of significant injuries should have an electrocardiogram, arterial blood gas analysis, complete blood cell count, type and cross-match, coagulation profile, and biochemistry testing, including electrolytes, glucose, and liver and renal function testing. Upper gastrointestinal endoscopy should be performed in symptomatic patients or those with visible burns in the mouth or throat. Although the absence of symptoms or signs does not preclude the presence of gastrointestinal burns, in patients with accidental ingestions, such injuries are always of a minor nature and endoscopy is not necessary [17]. Minor symptoms or grade I visible burns following the accidental ingestion of substances shown to have low toxicity, such as sodium hypochlorite household bleach (less than 10% solution) and hair relaxer gel, do not necessarily require endoscopy, as significant injuries are rare in this setting [36]. However, endoscopy is still recommended if excessive drooling or dysphagia or significant mucosal burns occur after ingestion of these products or if there is doubt about the exact composition of the ingested substance [36]. In contrast, in those with ingestions of strong acids or bases, significant injuries may be present in the absence of clinical findings, and endoscopy is indicated. Because injuries may progress over several hours, endoscopy performed earlier may not detect the full extent of injury and therefore may need to be repeated. In the past, it was recommended that the endoscope not be passed beyond the first circumferential or full-thickness lesion because of the risk of iatrogenic perforation. Not examining beyond the first significant lesion results in failure to detect more distal lesions of the stomach or duodenum [37]. The endoscope should be advanced across the cricopharynx under direct vision to assess for the presence of laryngeal burns [18]. If laryngeal edema or ulceration is noted, the airway should be intubated before endoscopy is continued. Examination should be done gently with minimal air insufflation, avoiding retroversion or retroflexion, and the procedure terminated if the endoscope cannot be easily passed through a narrowed area. Therapeutic dilation of the esophagus on initial endoscopy carries a high risk of perforation and should be avoided [17]. It should also be avoided during the subacute phase (5 to 15 days after ingestion), when the tensile strength of tissues is lowest [18]. Some parallel grading systems used for thermal skin burns; others differentiate several levels of ulceration and necrosis (Table 111. Injuries that consist only of mucosal inflammation or superficial ulceration and do not involve the muscularis are not at risk for stricture formation [18]. Patients with full-thickness circumferential burns and extensive necrosis are at high risk for perforation and stricture formation.
Hauke, 47 years: Neurotoxicity the penicillins are irritating to neuronal tissue, and they can provoke seizures if injected intrathecally or if very high blood levels are reached. Identifying and preventing individuals who have been exposed to tuberculosis from developing active disease is a major public health goal. Despite this preference, family members of critically ill patients often demonstrate avoidant behaviors that suggest not wishing to “know all. The second type of bronchiolitis obliterans occurs in patients who have persistent cough and dyspnea with an obstructive ventilatory impairment on pulmonary function tests that does not respond to inhaled corticosteroids or bronchodilators [139,140].
Falk, 22 years: Centrally Located Shunt the median sternotomy approach allows the pulmonary artery end of the shunt to be placed more centrally. Patients can develop sinus arrest especially immediately after sudden termination of a tachyarrhythmia which may require immediate intervention. Trussell J, Contraceptive efficacy of the and Ethnicity, 2006, the Alan Gutt- Reality® female condom, Contraception macher Institute, New York, 2009. Guinot P-G, Zogheib E, Petiot S, et al: Ultrasound-guided percutaneous tracheostomy in critically ill obese patients.
Rendell, 53 years: For determining reversibility of delirium, a clinician should review the patient’s principal diagnosis, comorbidities, prognosis, and preadmission and current functional status. Hiramatsu Y, Maeda Y, Fujii N, et al: Use of micafungin versus fluconazole for antifungal prophylaxis in neutropenic patients receiving hematopoietic stem cell transplantation. Voriconazole also has activity against this Histoplasma and has been administered in a small number of patients. The unwitting host scratches the site and inoculates the infected feces into the wound or onto mucous membranes.
Karrypto, 59 years: Imaging studies of the head should be performed for patients with persistent altered mental status, followed by lumbar puncture as clinically indicated. Absence of cough If three to four of these criteria are met, the positive predictive value is only 40-60%, but the absence of three to four of the criteria has a negative predictive value of 80%. Others believe that this raised urea may simply be a reflection of the prerenal impairment sec- ondary to hypovolaemia. Clinicians ofen become impressed that switching to another product efectively stops the break- through bleeding.
Faesul, 26 years: Murai H, Murakami S, Ishida K, et al: Elevated serum interleukin-6 and decreased thyroid hormone levels in postoperative patients and effects of Il-6 on thyroid cell function in vitro. There is little evidence that impaired heat dissipation or altered hypothalamic regulation is instrumental in producing acute hyperthermia in these patients. An electrocardiogram should be obtained and continuous monitoring performed whenever there is a significant chance of dysrhythmia. For extensive and severe cases, a 2- to 3-week tapering course of oral prednisone, along with an oral antihistamine to relieve pruritus, is appropriate.
Topork, 62 years: The most common history is binge drinking in the setting of poor intake of other dietary carbohydrates. Symptoms suggestive of cervical myelopathy include Lhermitte’s sign, neck pain radiating up to the occiput, paresthesias in the hands or feet, loss of arm or leg strength, and urinary incontinence or retention. This process presumably results in a diminution of tissue distortion, resolution of vascular compromise, and reduced bubble– endothelial surface contact. However, the steeple sign may be absent in patients years of age and decrease with age.
Agenak, 34 years: For the treatment of arrhythmias or hypertension, medications that possess rapid reversibility and a short half-life are preferred. This initiates a period of waning ovarian function called the climacteric, which lasts several years, carrying a woman through decreased fertility and menopause to the postmenopausal years. The the symptoms may be attributed to the pregnancy and exact treatment depends on the primary treatment, the colposcopic assessment of the pregnant cervix is not site and stage of the recurrence, the presence of distant always easy; advice should be obtained from an experi- disease, its resectability, treatment‐related morbidity enced colposcopist. Pneumonia may show varying degrees of lung opacities and would have to be correlated clinically.
Fadi, 50 years: This results in kidney damage ranging from mild, reversible renal impairment to severe, potentially irreversible acute tubular necrosis. Therefore, patients presenting with acute monoarthritis or oligoarthritis require prompt arthrocentesis with subsequent synovial fluid analysis, preferably before initiation of treatment. Levels of IgM usually peak between 3 and 6 weeks after the initial infection; levels of IgG rise gradually over months. The actions of cytokines include both autocrine and paracrine effects on cell proliferation and differentiation and on induction of other cytokines.
Mazin, 35 years: Jinjuvadia R, Liangpunsakul S: Trends in alcoholic hepatitis-related hospitalizations, financial burden, and mortality in the United States. Conduit from Right Ventricle to Pulmonary Artery Alternatively, a pulmonary homograft may be interposed between the right ventricular opening and the enlarged main pulmonary artery (see Chapter 27). Although can have negative effects on fetal development, birth the expression of the symptoms is presumed to be related outcome and child development. In healthy pregnancy there is ing for common trisomies, pregnancy‐associated plasma normally low resistance and high flow.
Miguel, 38 years: If the valve is trileaflet, subcommissural sutures at one or more commissures may increase the central coaptation of the leaflets. Rather, the principal aim of nutritional intervention is to support the protein synthetic response to injury and, therefore, narrow the negative nitrogen gap (where output exceeds input) that occurs during severe metabolic stress. Experimental serotyping methods are available that can identify specific lipopolysaccharide antigens (O antigens) and flagellar antigens (H antigens) associated with specific pathogenic characteristics. Invasive intestinal disease presents with the gradual onset, over 1-3 weeks, of abdominal pain and bloody diarrhea associated with tenesmus and abdominal tenderness.
Akrabor, 30 years: Endotherapy is indicated for all patients with high-risk lesions because of the significant risk of persistent or recurrent bleeding (22% to 55%) and even death if left untreated [3,4,46]. Cerebral vascular effects are also significant with theophylline and other methylxanthines because they are potent cerebral vasoconstrictors. This care should be with transfer of single embryos reduces significantly holistic in approach (in the widest sense) and could be (but not completely) the risk of multiple pregnancy. In another group, the onset may This phase is the period of pleural effusion in children over be insidious with the child appearing unwell, febrile and 5 years and bronchial disease in those below 5 years and losing weight.
8 of 10 - Review by Y. Ressel
Votes: 348 votes
Total customer reviews: 348
References
- Writing Group M, Mozaffarian D, Benjamin EJ, et al. Heart disease and stroke statistics-2016 update: a report from the american heart association. Circulation. 2016;133:e38-e360.
- Kassim SH, Li H, Vandenberghe LH, et al. Gene therapy in a humanized mouse model of familial hypercholesterolemia leads to marked regression of atherosclerosis. PLoS One 2010;5:e13424.
- Ritchie RH, et al. Exploiting cGMP-based therapies for the prevention of left ventricular hypertrophy: NO? and beyond. Pharmacol Ther 2009;124:279-300.
- Di Carli MF, Hachamovitch R. New technology for noninvasive evaluation of coronary artery disease. Circulation. 2007;115:1464-1480.
- Garner W, Downs JB, Stock MC, Rasanen J: Airway pressure release ventilation (APRV)óa human trial, Chest 94:779, 1988.