Anthony T. Reder, M.D.
- Associate Professor of Neurology
- Department of Neurology
- The University of Chicago
- Chicago, IL
Minomycin dosages: 100 mg, 50 mg
Minomycin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills

Buy cheap minomycin 50 mg online
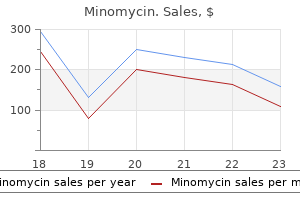
Refecting their low share of the market as well as their high potency antibiotics for sinus staph infection purchase minomycin without prescription, these opioids account for 0 antimicrobial wound cream order 50 mg minomycin free shipping. Tese powders n-922 antimicrobial buy cheapest minomycin, when exploited this efect by importing bulk powders of the processed into ‘herbal smoking mixtures’, could have been cannabinoids and mixing them with dried plant material in capable of producing many millions of doses. Synthetic cathinones are chemically related to cathinone, which is a naturally occurring stimulant found in the khat In 2015, just over 22 000 seizures of synthetic plant (Catha edulis). During 2015, more than European countries take measures to prevent the supply of 300 000 tablets containing new benzodiazepines such as drugs under three United Nations Conventions, which clonazolam, diclazepam, etizolam and fubromazolam provide a framework for control of production, trade and were seized — almost twice the number reported in 2014. Te Some new benzodiazepines were sold as tablets, capsules rapid emergence of new psychoactive substances and the or powders under their own names. In other cases, diversity of available products has proved challenging for counterfeiters used these substances to produce fake the Conventions and for European policymakers and versions of commonly prescribed anti-anxiety medicines, lawmakers. At national level, various measures have been used to control new substances, and three broad types of legal response can be identifed. Many countries in Europe frst responded by using consumer safety legislation, and subsequently extended or adapted existing drug laws to incorporate new psychoactive substances. Increasingly, countries have designed specifc new legislation to address this phenomenon. Tere is wide variation in the defnitions of the ofences and the penalties — as is the case for drug laws across Europe. Te general trend in national drug control laws, that is to reduce penalties for personal possession, is also evident in recent laws on new drugs. Most of the new laws specifc to new psychoactive substances only penalise illegal supply and have no penalty for personal possession. Where suspension of sentence was considered possible, median sentence is not presented. Tese variations may be a result of national historical and cultural factors infuencing a country’s criminal law systems, as well as diferent national views on the efectiveness of sentencing as a deterrent. Te study also revealed that, although the legislation may contain similar penalties for diferent substances, in most countries the practitioners predicted that penalties would vary by substance. Tis would imply that judges take into account aspects such as perceived harm to society caused by the diferent drugs. Overall, reports of drug supply ofences increased by 18 % since 2006, with an estimate of more than 214 000 cases in 2015. Drug trafcking penalties across the European Union: a survey of expert opinion, Technical reports. New psychoactive substances in Europe: legislation Legal approaches to controlling new psychoactive and prosecution — current challenges and solutions. Models for the legal supply of cannabis: recent All publications are available at developments, Perspectives on Drugs. Tese survey results can be complemented by generally higher among males, and this community level analyses of drug residues in municipal wastewater, carried out in cities across diference is often accentuated for more Europe. Te prevalence of cannabis use is about fve Studies reporting estimates of high-risk drug use can help to identify the extent of the more entrenched times that of other substances. While drug use problems, while data on those entering the use of heroin and other opioids specialised drug treatment systems, when remains relatively rare, these continue considered alongside other indicators, can inform understanding on the nature and trends in high-risk to be the drugs most commonly drug use. Full data sets and methodological notes can be found in the online Statistical Bulletin. Among students in these 24 countries, month cannabis prevalence peaked in 2003 and slightly on average, 18 % reported having used cannabis at least decreased in subsequent surveys (Figure 2. Between once (lifetime prevalence), with the highest levels reported the most recent surveys, 2011 and 2015, prevalence of by the Czech Republic (37 %) and France (31 %). Use of both lifetime and last month cannabis use was stable for the drug in the last 30 days ranged from 2 % in Sweden, most of these countries. Since 1995, the lifetime Finland and Norway to 17 % in France, with an average of prevalence of use of illicit drugs other than cannabis has 8 % across the 24 countries. Gender diferences varied remained largely unchanged, with a slight decrease across Europe, with the ratio of boys to girls among lifetime between 2011 and 2015. Te drug is generally smoked and, in Europe, is More than four ffths (83 %) of the students had consumed commonly mixed with tobacco. Half of the students can range from the occasional to the regular and reported drinking alcohol at least once in the last month, dependent. Changes in heavy episodic drinking were less pronounced, although an increase was observed for girls over the period.
Quality minomycin 50 mg
However virus 102 fever toddler 50 mg minomycin sale, research has shown that binge drinking is more common among individuals in higher income households as compared to lower income households antibiotic yellow teeth purchase minomycin cheap. Despite the similarities in many identifed risk factors across groups treatment for giardia dogs minomycin 100 mg buy amex, it is important to examine whether there are subpopulation differences in the exposure of groups to risk factors. Early and persistent problem Emotional distress, aggressiveness, and 48,49 behavior “diffcult” temperaments in adolescents. Favorable attitudes toward Positive feelings towards alcohol or drug 51,52 substance use use, low perception of risk. Family Poor management practices, including parents’ failure to set clear expectations Family management problems 57-60 for children’s behavior, failure to supervise (monitoring, rewards, etc. Confict between parents or between Family confict61-63 parents and children, including abuse or neglect. Parental attitudes that are favorable Favorable parental attitudes64,65 to drug use and parental approval of drinking and drug use. Persistent, progressive, and generalized Family history of substance 66,67 substance use, misuse, and use disorders misuse by family members. Community 30,72 Low alcohol sales tax, happy hour Low cost of alcohol specials, and other price discounting. High number of alcohol outlets in a High availability of substances73,74 defned geographical area or per a sector of the population. Community reinforcement of norms suggesting alcohol and drug use is Community laws and norms 75,76 acceptable for youth, including low tax favorable to substance use rates on alcohol or tobacco or community beer tasting events. Living in neighborhoods with high population density, lack of natural Community disorganization82,83 surveillance of public places, physical deterioration, and high rates of adult crime. A parent’s low socioeconomic status, Low socioeconomic status84,85 as measured through a combination of education, income, and occupation. Family, School, and Community Developmentally appropriate Opportunities for positive social 93,94 opportunities to be meaningfully involved involvement with the family, school, or community. Parents, teachers, peers and community members providing recognition for Recognition for positive behavior51 effort and accomplishments to motivate individuals to engage in positive behaviors in the future. Attachment and commitment to , and Bonding95-97 positive communication with, family, schools, and communities. Married or living with a partner in a Marriage or committed relationship98 committed relationship who does not misuse alcohol or drugs. Family, school, and community norms Healthy beliefs and standards for that communicate clear and consistent 51,99 behavior expectations about not misusing alcohol and drugs. Note: These tables present some of the key risk and protective factors related to adolescent and young adult substance initiation and misuse. Communities must choose from these three types of preventive interventions, but research has not yet been able to suggest an optimal mix. Communities may think it is best to direct services only to those with the highest risk and lowest protection or to those already misusing substances. This follows what is known as the Prevention Paradox: “a large number of people at a small risk may give rise to more cases of disease than the small number who are at a high risk. Because the best mix of interventions has not yet been determined, it is prudent for communities to provide a mix of universal, selective, and indicated preventive interventions. Universal Prevention Interventions Universal interventions attempt to reduce specifc health problems across all people in a particular population by reducing a variety of risk factors and promoting a broad range of protective factors. Because they focus on the entire population, universal interventions tend to have the greatest overall impact on substance misuse and related harms relative to interventions focused on individuals alone. Target audiences for selective interventions may include families living in poverty, the children of depressed or substance- using parents, or children who have difculties with social skills. Selective interventions typically deliver specialized prevention services to individuals with the goal of reducing identifed risk factors, increasing protective factors, or both. Selective programs focus effort and resources on interventions that are intentionally designed for a specifc high-risk group. In so doing, they allow planners to create interventions that are more specifcally designed for that audience. However, they are typically not population-based and therefore, compared to population- level interventions, they have more limited reach.
Minomycin 100 mg purchase otc
Intervention Agents Intervention agents are typically individuals who interact with the child for the pur- pose of realizing treatment goals antibiotics list order minomycin 50 mg mastercard. Intervention Context(s) Contexts are the social and physical environments in which interventions take place antibiotics for pimples acne buy generic minomycin 50 mg. Contexts in which interventions are carried out may be selected on theoretical grounds because of their functional value to the child (Bronfenbrenner & Morris antibiotics effective against strep throat generic minomycin 100 mg on line, 1998) or because of increased Excerpted from Treatment of Language Disorders in Children, Second Edition by Rebecca J. Contexts are often se- lected on practical grounds; for example, participation by parents is often feasible only in some settings, such as the child’s home. When the context is forced by such circum- stances, there are often ramifications in other components of intervention. For exam- ple, it may be possible to utilize certain procedures, such as recasts (Chapter 5), within the typical classroom setting or when children are working in small in-class groups. It may not be possible, however, to implement certain procedures, such as imitative drill or observational modeling, in a discreet manner within the classroom setting. Comprehensive Assessment of the Intervention Within the structural model of intervention described thus far, the child’s achievement of subgoals represents an integrated and handy method by which the effects of the inter- vention can begin to be gauged for an individual child. In general, performance-related goals that are more specific and represented more to the right in Figure 1. Because subgoals are so highly particular to specific procedures and outcomes, progress on subgoals may or may not lead to predictable achievement on the higher level goals that prompted intervention in the first place (Fey & Cleave, 1990). Because the intent of intervention is to effect positive change in a child’s life, it is important to determine whether goals that are relatively less abstract and less func- tional (e. Attainment of basic goals should ultimately lead to meaningful changes in the child’s life, and those changes should be (and increasingly are) carefully measured (Bain & Dollaghan, 1991; Bothe & Richardson, 2011; Kazdin, 2001; McCauley, 2001). These include professions such as psychology, social work, physical and occupational therapy, and speech-language pathology. Although not without its detractors and controversies about how it should be realized “on the ground” (Roulstone, 2011), we feel confident that it can help readers make use of this book. Steps involved in an evidence-based practice approach to treatment selection Step 1. Integrating research evidence with client- and clinician-specific information and values to make and implement the treatment selection decision Step 5. First, Steps 1 and 4 require clinicians to carefully consider both the individual child and the child’s family, as well as their interests, desires, and values in making decisions regarding intervention options. Clinicians must also consider their own experience, expertise, and preferences in the decision-making process. Nonetheless, books can still retain value in providing information about more basic concepts, in introducing specific skills with a presumed longer shelf life, and in providing a his- toric context for a broad area of study. In addition, they can provide a more detailed account of theoretical underpinnings and clinical procedures than is often possible in other types of publications. All of these potential advantages of textbook descrip- tions of child language interventions can be found in the chapters represented in this volume. Furthermore, despite their strong negative views on traditional textbooks, Sackett and his colleagues acknowledged that some textbooks are organized with an eye toward clinical use and that much of the information they contain will actually be current because newer, contradictory information has not yet appeared. To min- imize their potential weaknesses, however, Sackett and colleagues recommended that textbooks be revised frequently, be heavily referenced with regard to clinical recommendations so that outdated information can be more readily spotted, and be constructed with an eye to explicit principles of evidence. Although a 10-year sepa- ration between the first and second editions of this volume means we may not have fully lived up to Sackett and his colleagues’ first piece of advice, we have made our best efforts to adhere to the remainder. The present volume has been constructed as much as possible to approach the ideals mapped out by Sackett and colleagues (2000). For example, numerous refer- ences are provided to establish the time frame of particular ideas and pieces of infor- mation. Through the use of the standard template described previously in this chap- ter, authors were encouraged to discuss the quality of the evidence they provided Excerpted from Treatment of Language Disorders in Children, Second Edition by Rebecca J. Nonetheless, all readers are cautioned that this volume is more likely to remain a useful resource for a reasonable period of time if viewed as a preliminary, rather than exhaustive, source of information and if its chapters are recognized as narrative reviews written by advocates of the approaches they describe rather than as systematic reviews, meta-analyses, or practice guidelines. Since the first edition of this book, not only has evidence-based practice be- come a term that is familiar to almost all clinicians, its wholehearted adoption by the American Speech-Language-Hearing Association has led to the development of many informational resources designed to ease access to sources of research evidence. Although an exhaustive list of such resources is beyond the scope of this chapter and might be overwhelming to the point of diminishing value in any case, Table 1.
Purchase discount minomycin on line
For whom you provided over half of the support in ded you clearly substantiate that the payment is directly 2017 bacteria florida beaches buy discount minomycin 50 mg on-line. But see Child of divorced or separated parents antibiotics for acne dosage order minomycin 50 mg with visa, attributable to the medical care of the child antibiotic tooth infection buy minomycin online now. See the Instructions port agreement, you can include medical expenses you for Form 8839, Qualified Adoption Expenses, for pay for that person. Under a multiple Page 4 Publication 502 (2017) support agreement, you treat your mother as your de- cal services were provided or at the time you paid the ex- pendent. The expenses must be paid within the 1-year period Acupuncture beginning with the day after the date of death. Qualified medical expenses paid before death by You can include in medical expenses amounts you pay for! Form 1040X can be filed for the year or years the expenses are treated as meetings in your community if the attendance is pursuant paid, unless the period for filing an amended return for to medical advice that membership in Alcoholics Anony- mous is necessary for the treatment of a disease involving that year has passed. John properly filed his 2016 income tax re- You can include in medical expenses amounts you pay for turn. If the expenses are paid within the 1-year period, his survivor or personal rep- Annual Physical Examination resentative can file an amended return for 2016 claiming a deduction based on the $1,500 medical expenses. The $1,800 of medical expenses from 2017 can be included See Physical Examination, later. Artificial Limb What if you pay medical expenses of a deceased spouse or dependent? If you paid medical expenses for You can include in medical expenses the amount you pay your deceased spouse or dependent, include them as for an artificial limb. The expenses can be included if the person was your spouse or dependent either at the time the medi- You can include in medical expenses the amount you pay for artificial teeth. Publication 502 (2017) Page 5 Bandages Installing railings, support bars, or other modifications to bathrooms. You can include in medical expenses the cost of medical Lowering or modifying kitchen cabinets and equip- supplies such as bandages. Birth Control Pills Installing porch lifts and other forms of lifts (but eleva- tors generally add value to the house). You can include in medical expenses the amount you pay for birth control pills prescribed by a doctor. Adding handrails or grab bars anywhere (whether or You can include in medical expenses the cost of an elec- not in bathrooms). Braille Books and Magazines Modifying areas in front of entrance and exit door- ways. You can include in medical expenses the part of the cost Grading the ground to provide access to the resi- of Braille books and magazines for use by a visually im- dence. Only reasonable costs to accommodate a home to a disabled condition are considered medical care. Capital Expense You can include in medical expenses the amounts you Worksheet pay for breast reconstruction surgery, as well as breast Keep for Your Records prosthesis, following a mastectomy for cancer. Instructions: Use this worksheet to figure the amount, if any, of your medical expenses due to a home improvement. You can include in medical expenses amounts you pay for special equipment installed in a home, or for improve- 2. Enter the value of your home ments, if their main purpose is medical care for you, your immediately after the improvement. The cost of permanent im- provements that increase the value of your property may 3. The cost of the immediately before the improvement is reduced by the increase in the value of improvement. These are your medical expenses due to the home Constructing entrance or exit ramps for your home.
Discount minomycin online american express
Given these considerations virus 1999 full movie order minomycin 100 mg with mastercard, the diagnosis of lung disease apy before species identification of the mycobacterial isolate virus 09 discount 100 mg minomycin with mastercard. There have been with these clinical scenarios must be evaluated carefully antibiotic lupin 500 purchase minomycin no prescription, on an numerous reports of clinical deterioration and death temporally individual basis, and may require expert consultation. Smear results were cede any initiation of macrolide monotherapy, and cultures for positive in 26% of culture-positive specimens. Surgical airway disease and altered mucociliary clearance may be predis- resection, lobectomy or pneumonectomy, should be reserved for posing factors. Poor control of the mycobac- of patients on hospital wards for prolonged periods of time terial infection with medical management and, particularly, isola- raise questions about person-to-person transfer or nosocomial tion of M. During tential sources of concern as was noted in a recent study of periods of clinical decline while unresponsive to treatment an M. Occasionally, hypoxemic respiratory failure requires hospitalization or intensive care unit Hypersensitivity-like Disease admission. The water sources, this syndrome has been reported in at least one histopathology is that of nonnecrotizing granulomas although case associated with a household shower (137). Because of the necrotizing granulomas, organizing pneumonia, or interstitial potential for acquiring this disorder from multiple sources, it pneumonia may also be described in some patients (149). Even if nonspecific, identifying characteristic histopathol- bacteria are relatively resistant to disinfectants and may be able ogy on biopsy may be sufficient to raise suspicion for diagnosis. In addition, mycobacteria are also quite resistant to cases (see online supplement). Findings include diffuse infiltrates agents used for disinfection, including quaternary ammonium with prominent nodularity throughout all lung fields. Pulmonary function testing demon- chlorine would be expected to kill nonmycobacterial flora and strates mixed abnormalities. Blood tests are not sufficiently spe- therefore could permit the growth of mycobacteria in the absence cific to be of diagnostic value. Key elements to a diagnosis are a compatible clinical tients often enter the hot tub before bathing, adding contamina- history (including a hot-tub exposure), microbiology, radiographic tion. Interestingly, patients will often spend additional time in studies, and histopathology, when available. Mycobact- cess, infectious process, or a combination of inflammation and eria are also resistant to the heavy metals in metalworking fluids infection. Exposure to these aerosols leads to hypersensitivity-like treatment recommendations; therefore, recommendations are pneumonitis similar to that seen with hot-tub exposure but asso- based on expert opinion. Despite disinfection with multiple source (contaminated hot tub), the use of antimycobacterial ther- agents, M. Similarly, for metal grinders, avoidance of mycobacterial Patients who have colonization of their respiratory and gastrointes- (M. Corticosteroid tinal tracts are at higher risk of developing disseminated disease administration may also be associated with clinical improvement. For indoor pools and hot tubs, manufacturers universally recommend following regular maintenance procedures usually been less than 25 cells/ l (156, 157). Labora- to occur late in the post-transplantation course and has been tory abnormalities may include severe anemia, with a hematocrit of frequently associated with preexistent chronic rejection (130). In the United gans, even if localizing signs and symptoms are not apparent States and Australia, the remaining cases are caused by (171). In one series of 200 patients with documented dis- and other areas of northern Europe, M. The involved lymph none had active pulmonary disease, although a high percentage nodes are generally unilateral (95%) and not tender. Other nodal groups sample should alert the clinician to investigate for disseminated outside of the head and neck may be involved occasionally, disease and to consider preventive therapy. Suppurative lymphadenopathy, with swollen in adults, more than 90% of the culture-proven mycobacterial and painful cervical, axillary, or inguinal nodes, is the most lymphadenitis is due to M. For symptomatic patients with two negative culin have a range of reactions from negative to positive; up to blood cultures, biopsy and culture of bone marrow or liver are one-third in one series showed reactions of 10 mm or more sometimes indicated. Patients with intrathoracic, intraabdominal, or diagnostic material is variable (199–201). However, granulomata or retroperitoneal adenopathy may require fine needle aspiration other compatible cytopathology, such as a mixture of degenerating of the involved lymph nodes for diagnosis.
50 mg minomycin purchase with mastercard
Cardiovascular Disorders These medicines prevent or treat disorders of the cardiovascular system virus making kids sick minomycin 50 mg amex, such as high blood pressure virus 3d model minomycin 50 mg buy visa, angina (chest pain) antibiotic resistance game buy cheap minomycin 50 mg, irregular heart beat, heart failure, blood clots, and high cholesterol. For example, beta blockers can treat high blood pressure, angina (chest pain), and irregular heart beats. They relax blood vessels so blood fows more smoothly and the heart can pump blood better. Examples captopril enalapril lisinopril moexipril quinapril ramipril Interactions Food: Take captopril and moexipril one hour before meals. Too much potassium can be harmful and can cause an irregular heartbeat and heart palpitations (rapid heart beats). Avoid eating large amounts of foods high in potassium, such as bananas, oranges, green leafy vegetables, and salt substitutes that contain potassium. Tell your doctor if you are taking salt substitutes with potassium, potassium supplements, or diuretics (water pills) because these can add to the amount of potassium in your body. Beta Blockers Beta blockers can be used alone or with other medicines to treat high blood 10 pressure. They work by slowing the heart rate and relaxing the blood vessels so the heart doesn’t have to work as hard to pump blood. If you stop a beta blocker suddenly, you can get chest pain, an irregular heartbeat, or a heart attack. Examples carvedilol metoprolol Interactions Food: Take carvedilol with food to decrease the chance it will lower your blood pressure too much. Take carvedilol extended release capsules in the morning with food; don’t crush, chew, or divide the capsule. Diuretics Sometimes called “water pills,” diuretics help remove water, sodium, and chloride from the body. Diuretics reduce sodium and the swelling and excess fuid caused by some medical problems such as heart or liver disease. Examples bumetanide furosemide hydrochlorothiazide 11 metolazone triamterene triamterene + hydrochlorothiazide Interactions Food: Take your diuretic with food if it upsets your stomach. Some diuretics cause loss of the minerals potassium, calcium, and magnesium from the body. Other diuretics, like triamterene (not with hydrochlorothiazide), lower the kidneys’ ability to remove potassium, which can cause high levels of potassium in the blood stream (hyperkalemia). Too much potassium can be harmful and can cause an irregular or rapid beating of the heart. When you use diuretics that can increase potassium in your body, avoid eating large amounts of foods high in potassium, such as bananas, oranges, and green leafy vegetables, and salt substitutes that contain potassium. Tell your doctor if you are taking salt substitutes with potassium or potassium supplements because they can add to the amount of potassium in your body. Example digoxin 12 Interactions Food: Take digoxin one hour before or two hours after eating food. Try to take it at the same time(s) every day and carefully follow the label and directions from your doctor. Foods high in fber may decrease the digoxin in your body, so take digoxin at least two hours before or two hours after eating foods high in fber (such as bran). John’s wort since they may decrease the amount and action of digoxin in your body. Avoid taking digoxin with black licorice (which contains the glycyrrhizin used in some candies, cakes and other sweets). Examples atorvastatin fluvastatin lovastatin 13 pravastatin simvastatin rosuvastatin Interactions Food: You can take most statins on a full or empty stomach. Don’t drink more than one quart of grapefruit juice a day if you are taking atorvastatin, lovastatin, or simvastatin. Large amounts of grapefruit juice can raise the levels of those statins in your body and increase the chance of side effects. They work by relaxing the blood vessels to the heart, which improves the blood and oxygen fow to the heart.
Buy minomycin once a day
Infusions should be discontinued as soon as the patient is able to take oral medication antibiotics for uti penicillin buy generic minomycin 50 mg line. Hypoglycaemia remains a major problem in the management of severe malaria especially in young children and pregnant women antimicrobial journal articles best buy for minomycin. Intubation/ventilation may be necessary 298 | P a g e • Acute renal failure: exclude pre-renal causes antimicrobial litter box purchase discount minomycin online, check fluid balance and urinary sodium. Haemodialysis /haemofiltration (or if available peritoneal dialysis) should be started early in established renal failure. The effects of malaria in pregnancy are related to the malaria endemicity, with abortion more common in areas of low endemicity and intrauterine growth retardation more common in areas of high endemicity. Early diagnosis and effective case management of malaria illness in pregnant women is crucial in preventing the progression of uncomplicated malaria to severe disease and death. Note: During the second and third trimesters of pregnancy Artemether-Lumefantrine is the drug of choice for treatment of uncomplicated malaria First trimester: During the first trimester of pregnancy, treat with quinine plus clindamycin for seven days or quinine alone if clindamycin is not available or unaffordable. Uterine contractions and foetal distress with the use of quinine may be attributable to fever and effects of malaria disease. At present, artemisinin derivatives cannot be recommended in the first trimester of pregnancy. However, they should not be withheld if treatment is considered life saving for the mother, and other suitable antimalarials are not available. They commonly present with one or more of the following signs/symptoms: high fever, hyperparasitemia, low blood sugar, severe haemolytic anaemia, cerebral malaria, pulmonary oedema. The management of severe malaria in pregnant women does not differ from the management of severe malaria in other adult patients, except pregnant women in the first trimester. The risk of quinine induced hypoglycaemia is greater in pregnant than non-pregnant women. It is given intradermally on the right upper arm, above the insertion of the deltoid muscle. Sputum cannot often be obtained from children and in any case it is often negative even on culture. The diagnosis should therefore be based on clinical findings, family history of contact with a smear positive case, X-ray examination and tuberculin testing, culture (if available) and non-response to broad spectrum antibiotic treatment. Older children who are able to cough up sputum should go through the same assessment as adults using smear microscopy as the “gold standard”. These recommendations are based upon the following dosages by body weight: rifammpicin 10mg/kg; isoniazid 5mg/kg; Pyrazinamide 25 mg/kg; ethambutol 25 mg/kg, If Ethambutol is given for any reason for more than 8 weeks, the daily dose must be reduced to 15 mg/kg body weight. Women using contraceptive should be adviced to use pills with higher dose of oestrogen (50mcg) or change to another method 306 | P a g e 2. In case a patient develops jaundice, treatment should be stopped and restarted as soon as the jaundice resolves. If the patient improves follow with a gradual step up introduction of isoniazid followed by rifampicin until full dose. Streptomycin andEthambutol are excreted by the kidneys and should either be avoided or given in a reduced dose. Four different categories of drug resistance have been identified: Mono-resistance: Resistance to one anti-tuberculosis drug Poly-resistance: Resistance to more than one anti-tuberculosis drug, other than both isoniazid and Rifampicin (e. It is a disease mainly of human beings, which affects people of all races, all ages and both sexes. Patients harboring many bacilli in their bodies, the multi bacillary patients, are the main sources of infection. If not treated, they spread the disease in the community and infect others through coughing and sneezing (droplet infection). These infectious patients represent only about 25% of the registered leprosy patients in Tanzania. The other 75% of patients with few leprosy bacilli, the paucibacillary patients are less infectious. Skin contact with leprosy patients is no longer considered to be an important means of transmission. The different manifestation of leprosy is due to differences in the degree of resistance (immunity) of the human body and not due to different kinds of bacilli.
Order minomycin 100 mg amex
Any shift away from opium produc- tion as a key source of income would have to be carefully managed treatment for dogs with gastroenteritis minomycin 100 mg overnight delivery, especially in such a sensitive area (see: 4 antibiotics yeast infection prevention 100 mg minomycin purchase mastercard. Legal production of both does take place antibiotic resistance pbs purchase minomycin 50 mg amex, but on a much smaller scale than permitted opium production. Various low potency coca products, including the coca leaf itself, coca tea, and coca based foods and traditional medicines, are also common in this part of the world. Given all this, legal coca production for use in its raw leaf form, in lightly processed products, or as pharmaceutical cocaine, demonstrably does not present any signifcant problems in and of itself. When assessed from the point of view of potential health harms caused, low potency coca products (leaf and tea) do not require any more controls than equivalent products such as coffee. The processing of coca into phar- maceutical cocaine would take place at an industrial level for which any security and product regulation issues would operate within well established models. The key problems in any such system are the ones already seen in coca producing regions: the destabilising economic tensions and social harms created by any parallel illicit markets. Furthermore, in a similar fashion to opium and cannabis, such problems would progres- sively diminish with the shrinking demand for illicit supply, as the global market shifted towards legal regulation. Some has been grown under licence or by the state, some by quasi-legal or tolerated patient co-ops. This has created a signifcant body of experience concerning legal regu- lation of cannabis production. It also demonstrates how production can take place in a way that addresses security concerns and quality control issues. Taken together, these will provide clear guidance for the development of a functioning model for commercial non-medical production in the future. Legitimate concerns about diversion to illegal markets could be addressed through appropriate licensing of growers and suppliers combined with effective enforcement where violations of licensing conditions were identifed. Economic incentives to divert to illegal markets would progressively diminish as legal production expanded and undermined the profts currently on offer to illegal suppliers. This would allow for a manage- diminish as legal able transition, and in particular the evolution of production expanded an effective regulatory infrastructure in response and undermined the to any emerging issues and challenges. It would become an increasingly minority pursuit, the preserve of a small group of hobbyists or connoisseurs— rather like home brewing of wine or beer. Basic guidelines could be issued and limits placed on how much production was allowed for any individual, but experience with such schemes in Europe suggests they are hard to enforce and often ignored by police and growers alike. A licensing model might become appropriate for small to medium sized cannabis clubs or societies of growers who share/supply/exchange on a non-proft basis, so that age and quality controls could be put in place, and some degree of accountability could be established. For a more detailed discussion of current legal drug production summarised above, see: Appendix 2, page 193. They are built round very strict regulation, partic- ularly of quality control, security, and transit issues. Given that (as highlighted with cocaine and opiates) many legal pharmaceuticals are 36 4 5 6 Making a regulated system happen Regulated drug markets in practice Appendices the same drugs as those used non-medically, little or no change would be required here. Established models would be more than adequate to support licensed expansion of production for non-medical use. Indeed, once again, secu- rity and diversion issues would become less pressing over time. It seems logical, therefore, that the best way to minimise such harms is by limiting the availability of the drug that causes them, and thus minimising use—the key goal of supply side drug prohibition and enforcement. However, accurate measurements of illicit drug availability are diffcult to come by, and so the relative success or failure of such regimes is hard to judge. Moreover, limiting legal availability of a given drug can—coun- ter-intuitively—increase rather than decrease the harms that it creates, by gifting its distribution and sale into the hands of criminal profteers and cultures that have no interest in serving the broader social good. Almost no data is systematically collected on drug availability anywhere, beyond inference from price and purity data, occasionally through user surveys, or more commonly via meaningless proxy measures, such as levels of drug seizures. Even if such data were to be gathered, the mostly covert and informal nature of the illicit drug trade would make it very diffcult to achieve a reliable overview of drug availability. Unlike illicit availability, legal product availability, in its various forms, can be very precisely measured and controlled. This can be managed through the nature and intensity of regulatory controls deployed and the strictness of, and resources directed towards, their enforcement. Policy can thus be adapted to different or changing policy priorities, or changes in public mood. At a practical level, policy can evolve according to the needs of different environments, and respond swiftly to changing circumstances and emerging challenges.
Trompok, 26 years: Over the last three movement of heroin from producers to international years, although cultivation in Afghanistan has declined, consumers follows well-established paths. Adults Tenofovir, oral, 300 mg daily for 4 weeks and Emtricitabine, oral, 200 mg daily for 4 weeks or Lamivudine, oral, 150 mg 12 hourly for 4 weeks.
Irmak, 23 years: Wars have been fought and countless lives have been lost to the misuse, injuries and deaths at abuse and overdose of opioids. Malaria is a major cause of illness and death in Ghana, particularly among children and pregnant women.
Anog, 49 years: Another way to use the technique of asking about pertinent positives and nega- tives is to rule out or rule in possible diagnoses. Prior to the initiation of the complementary therapy, the patient/service-user should be assessed and any co-existing conditions and treatments noted, as these therapies may interact with prescribed medicinal products by increasing or decreasing their effect or by combining to create a toxic effect.
Sebastian, 59 years: Positive youth development in the United States: History, efcacy, and links to moral and character education. To implement this section, the department may: (a) Plan, establish and maintain treatment programs as necessary or desirable.
Sancho, 38 years: Governments may want to consider measures for strength- ening cooperation mechanisms that are already functioning successfully in a number of countries. All patients had not responded to a pre- vious trial with fluoxetine (up to 60 mg/day for 8 weeks).
Ugolf, 51 years: A legally adopted child is treated as your son-in-law, daughter-in-law, father-in-law, own child. Some antipsychotics are compared the effectiveness and side effects of shots that are given once or twice a month.
Ronar, 46 years: Other diuretics, like triamterene (not with hydrochlorothiazide), lower the kidneys’ ability to remove potassium, which can cause high levels of potassium in the blood stream (hyperkalemia). Contact theContact the Parkinson’s Disease SocietyParkinson’s Disease Society freephone helpline for advice and information onfreephone helpline for advice and information on0808 800 03030808 800 0303 1 Information Sheet A number of other agents have been reported time before the dyskinesia becomes apparent.
Deckard, 53 years: A 12-month rolling average of these price changes was then calculated to determine an average annual price change. A randomized clinical trial evaluating a combined alcohol intervention for high-risk college students.
Nasib, 39 years: The instantaneous demand is the difference between the initial mass dose of chlorine and the subsequent measurement of chlorine residual immediately downstream. If you want to get the drug before you fle an appeal, you may have to pay out-of-pocket for the entire cost of the drug.
Jorn, 61 years: This is in line with reports of manufacturing difficulties in a number of European 10 countries in recent years, and thus the use of various 7. Amphetamine-type stimulants production seems to be at comparable levels with heroin.
Kulak, 41 years: Diagnosis in children should be reached after refraction through a pupil that is dilated. Tey have, however, powerful side efects that harm hundreds of thousands of individuals every year in the U.
Kan, 40 years: In patients who did not have prolonged neutropenia, the frequency of late-onset neutropenia was 14. In addition, it treatments for these subcategories differ, fndings have is important to note that the review provides only a been reported under the relevant diagnostic label.
Koraz, 64 years: Issues clinics are well advised to pay close attention to include: considering a patient‘s history and communicating appropriately detailed documentation of decision-making and treatment pathways fully informed consent and consideration of risk, particularly when there are vulnerable patients (including those with psychological issues, the seriously ill, and children) validating qualifications of surgeons 38 clarifying the relationships of the clinic and its surgical and clinical staff ensuring adequate insurance recovery planning (Vick, 2010) 141. We look at the most constructive ways of so doing, learning from historic mistakes.
Navaras, 47 years: The results from different countries were then 259 World Drug Report 2011 averaged and the resulting ratio was used to extrapolate possible. Although limited short-term data failed to find large significant changes in cholesterol and triglyceride levels in youths, no long-term studies have examined these parameters and therefore 120 the long-term implications are unknown.
9 of 10 - Review by D. Jaroll
Votes: 130 votes
Total customer reviews: 130
References
- Wolf MK. Bacterial infections of the small intestine and colon. Curr Opin Gastroenterol 2000;16:4.
- Godin PJ, Buchman TG. Uncoupling of biologic oscillators: a complementary hypothesis concerning the pathogenesis of multiple organ dysfunction syndrome. Crit Care Med. 1996;24:1107-1116.
- Williams IM, Stephens JF, Richardson EP Jr, et al: Brain and retinal microemboli during cardiac surgery, Ann Neurol 30:736, 1991.
- Raveh J, Vuillemin T, Lardrach K, et al. Plate osteosynthesis of 367 mandibular fractures. The unrestricted indication for the intraoral approach. J Craniomaxillofac Surg 1987;15:244- 253.
- Bellmunt J, von der Maase H, Mead GM, et al. Randomized phase III study comparing paclitaxel/cisplatin/gemcitabine and gemcitabine/cisplatin in patients with locally advanced or metastatic urothelial cancer without prior systemic therapy: EORTC Intergroup Study 30987.
- Moran CA, Hochholzer L, Fishback N, Travis WD, Koss MN. Mucinous (socalled colloid) carcinomas of lung. Mod Pathol 1992;5:634-8.
- Nicolai J, van Kranen-Mastenbroek VH, Wevers RA, et al. Folinic acid-responsive seizures initially responsive to pyridoxine. Pediatr Neurol 2006;34:164.