Gregory P. Marelich, M.D., FACP, FCCP
- Assistant Professor of Clinical Internal Medicine
- Division of Pulmonary and Critical Care
- Medicine
- University of California Davis Medical Center
- Sacramento, CA
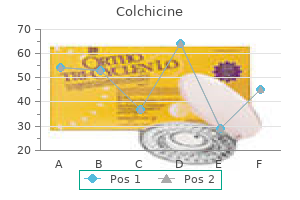
Colchicine dosages: 0.5 mg
Colchicine packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Cheap 0.5 mg colchicine overnight delivery
These infarction antibiotic ladder discount colchicine 0.5 mg visa, almost invariably occurring in the presence of an tumors represent approximately 10 to 12% of all pituitary adenoma virus killing robot order colchicine 0.5 mg online. In general bacteria killing foods colchicine 0.5 mg order with amex, delayed sur- deposition, posterior cervical fat, acanthosis nigricans, acne, gical intervention is reasonable, while at frst the disturbed hirsutism, thin skin, ecchymoses, and violaceous striae; the electrolyte water balance has to be stabilized, especially the last feature is present in only 50% of patients, and its ab- frequently observed hyponatremia; furthermore, “acute” sence does not exclude the presence of the syndrome. Those secondary hypoadrenalism has to be replaced by >100 mg patients usually experience weight gain, fatigue, sleeping cortisol per day before surgery can be performed. The re- difculties, irritability, depression, memory loss, difculty covery or restoration of any ophthalmologic defcits will not with concentrating, muscle weakness, bone fractures, or be adversely impacted by delayed surgery awaiting stable osteoporosis. Rathke Cyst, and Infltrative Disease The 2-mg dexamethasone suppression test overnight (from 10 p. Diabetes insipidus should be anticipated 7 Indications for Surgery on Pituitary Tumors: A Neurosurgeon’s Perspective 73 postoperatively if there is involvement of the pituitary stalk Microadenomas are defned as >10 mm in the longest di- or the hypothalamus. In some series of incidentalomas, headache was the tuitary neurosurgeon29 ofers the best possibility of achieving most common reason for performing imaging studies. Surgery is very efective in relieving management begins with observation and then progresses the mass efect; however, most patients harboring a large to conservative treatment and fnally surgical treatment. A careful history and physical Surgery is also the frst-line treatment of giant pituitary examination may reveal overlooked symptoms or signs of adenomas, with the exception of most prolactinomas, which hypersecretion of a specifc hormone, which can be eval- can be efectively treated with dopamine agonists. After the type and the degree of hormone excess has been evaluated by Transsphenoidal Pituitary Surgery sophisticated endocrine tests, treatment is indicated in nearly all cases. Does the lesion cause a mass efect or pituitary insuf- and suprasellar symmetrically developed, and intra- and ciency? Arita et Suprasellar tumor parts descend into the sella turcica in al27 report that approximately 20% of cases could become the majority of cases. Parasellar extensions of pitu- cidentaloma is an indication for surgery to prevent pituitary itary tumors, however, are more difcult to manage because insufciency. Given the with a minimum follow-up of 42 months in 60 microade- proximity of the optic nerves, optic chiasm, carotid arter- nomas; only 12. However, in ies, and cavernous sinuses to the sella, blind curettage of any 24 macroadenomas, 50% of the tumors were growing, caus- tumor remnants extending beyond the limits of the sella is ing visual feld defects in 57% of patients and documented potentially dangerous. For the microadenomas, watchful The standard microscope-based transsphenoidal approach waiting is recommend, whereas for the macroadenomas is limited in its ability to remove those tumors, which are de- early surgery should be considered. Patients with extrasellar extensions of tumor into the an- terior (subfrontal), middle, and posterior (retrosellar) cranial Radiologic Considerations fossae must be considered for two-stage procedures. In a patient treated medically to control the disease while awaiting the efects of radiation therapy, the medication should be discontinued periodically Transcranial Surgery (usually every 6 months) to determine whether the radia- In many larger asymmetric tumors, with significant su- tion treatment has become efective and whether there is prasellar, parasellar, retrosellar, and subfrontal extension, any new pituitary hormone defciency. They offer a high probability of safe, complete or near-complete, tu- mor removal. Often a transcranial method will be re- I Recurrence served for the second stage of a two-stage operation. A pituitary adenoma may is also indicated and superior to the pure microscopic ap- recur even 20 or more years after surgery; thus, all patients proach for all lesions infltrating the clivus area (chordoma, should be observed throughout life. Similar Additional Radiation and Medical Treatment to incidentalomas, all hormonally active adenomas must Radiation treatment (stereotactic, fractionated, gamma- treated urgently. In invasive adenoma, the tumor-growth knife, or proton-beam) of the pituitary is commonly used time plays a determining role. Surgery should be performed as an adjunctive treatment after incomplete tumor resec- at the latest when ophthalmologic symptoms and new en- tion. In patients with a large tumor in whom the resection docrinologic deterioration occur. No form of radiation delivery is when signifcant tumor growth is documented and func- immediately efective to reduce hormone hypersecretion. For acromegaly, this treat- veloped in the same location, as at frst surgery, should be ment includes somatostatin analogues (lanreotide or long- performed as soon it is safe to do so. Transsphenoidal microsurgery of the normal and pathologi- Curr Opin Neurol 2004;17:693–703 cal pituitary. The evaluation of patients itary Society for the diagnosis and management of prolactinomas.
Diseases
- Cardioauditory syndrome of Sanchez- Cascos
- Miller Fisher syndrome
- Hyperphenylalaninemia due to dehydratase deficiency
- Single ventricular heart
- Seizures mental retardation hair dysplasia
- Diaphragmatic defect limb deficiency skull defect
- X-linked trait
- Myopia, infantile severe
- 3 alpha methylcrotonyl-Coa carboxylase 1 deficiency, rare (NIH)
- Scrapie
Cheap colchicine 0.5 mg amex
These studies highlight the need for anesthesiologists to be25 aware of the risks and the means to protect themselves from radiation antibiotic resistance video buy cheap colchicine 0.5 mg on-line, especially in areas where fluoroscopy is used virus ntl buy generic colchicine. Using protective shielding (lead-lined garments and fixed and/or movable shields) 5th infection 0.5 mg colchicine order overnight delivery. Lead aprons, thyroid shields, and leaded eyeglasses are recommended despite being bulky and contributing to staff fatigue. Anesthesiology staff should consider using movable or fixed lead-lined glass shields so that they can gain easy access to their patients while protecting themselves from radiation. These data should be regularly reviewed by the facility’s radiation safety section or medical physics department. Radiologic contrast media are iodinated 2195 compounds classified according to their osmolarity (high, low, or iso- osmolar), their ionicity (ionic or nonionic), and the number of benzene rings (monomer or dimer). Nonionic contrast agents cause less discomfort on injection and have a lower incidence of adverse reactions. Adverse reactions to contrast agents may be divided into renal adverse reactions and hypersensitivity reactions. Nephrotoxic medications such as nonsteroidal anti-inflammatory drugs, aminoglycosides, and diuretics should be avoided for 24 to 48 hours before and after the use of intravenous contrast agents. Fatal hypersensitivity reactions may occur in about 1 per 100,000 contrast administrations. The clinical manifestations of various hypersensitivity reactions to contrast media are outlined in Table 33- 7. Although widely used, the effectiveness of corticosteroids and32 antihistamines in preventing hypersensitivity reactions to contrast agents in unselected patients is doubtful. Treatment of severe hypersensitivity33 reactions includes discontinuing the causative agent and supportive therapy, oxygen, intubating the trachea, cardiovascular support with fluids, 2196 vasopressors, and inotropes, and if required, bronchodilators. Severe reactions occur 1:10,000 to 1:40,000 and the mortality rate is 1 in a million injections. Patients are required to remain completely motionless during these procedures, which may be lengthy, particularly spinal angiography. Liberal use of local anesthetic at the puncture site precludes the need for intravenous analgesia. The injection of contrast media into the cerebral arteries may cause discomfort, burning, or pruritus around the face and eyes. During angiography and other interventional radiologic procedures, the patient is placed on a moving gantry and the radiologist positions the patient to track catheters as they pass from the groin into the vessels of interest. It is vital to have extensions on all anesthesia breathing circuits, infusion lines, and monitors to prevent these implements from being accidentally dislodged as the radiologist swings the x-ray table back and forth. The electrocardiogram electrodes and metallic coils in the cuffs of endotracheal tubes may cause interesting and annoying artifacts if they lie over the area being imaged. These procedures36 may be subdivided as “occlusive” and “opening” procedures (Table 33-2). A commonly employed technique is to insert37 detachable platinum coils into the abnormal vessel(s). Other occlusive agents include cyanoacrylates, “Onyx liquid embolic system” (Micro therapeutics Inc. These particles may also be used to produce temporary occlusion of blood vessels for preoperative embolization of vascular tumors, particularly meningiomas. In 2015, the American Heart Association and American Stroke Association jointly published guidelines for management of unruptured intracranial aneurysms. In the case of acute ischemic stroke, early (within 6 hours of symptoms) intervention to recanalize the occluded vessel by superselective intra-arterial thrombolytic therapy has been shown to improve outcome. Procedural and Anesthetic Technique Considerations in Interventional Neuroradiology For most interventional neuroradiologic procedures, arterial access is gained using a 6 or 7 French gauge sheath via the femoral or, rarely, the carotid or axillary artery. Anticoagulation is required during and up to 24 hours after interventional radiologic procedures to prevent thromboembolism. At the end of the procedure or in case of hemorrhage heparin may43 be reversed with protamine. General anesthesia and conscious sedation are both suitable techniques for interventional neuroradiology depending on the complexity of the procedure, the need for blood pressure manipulation, and the need for intraprocedural assessment of neurologic function. The anesthesiologist may facilitate the procedure by manipulating systemic blood pressure and controlling end-tidal carbon dioxide tension.
Colchicine 0.5 mg buy low cost
The role of the out-of-operating room anesthesiologist in the care of the cardiac patient infection attack 14 alpha buy colchicine without a prescription. Safety bundespolizei virus buy colchicine 0.5 mg with mastercard, feasibility treatment for dogs with gastroenteritis buy cheap colchicine 0.5 mg line, and long-term results of percutaneous closure of atrial septal defects using the Amplatzer septal occluder without periprocedural echocardiography. A meta analysis of current status of alcohol septal ablation and surgical myectomy for obstructive hypertrophic cardiomyopathy. Transcatheter aortic valve replacement: historical perspectives, current evidence, and future directions. Pro: a cardiovascular anesthesiologist should provide services in the catheterization and electrophysiology laboratory. The MitraClip and survival in patients with mitral regurgitation at high risk for surgery: a propensity-matched comparison. Percutaneous left atrial appendage closure for stroke prophylaxis in patients with atrial fibrillation: 2. Left atrial appendage closure as an alternative to warfarin for stroke prevention in atrial fibrillation: a patient-level meta- analysis. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. Catheter cryoablation of supraventricular arrhythmias: a painless alternative to radiofrequency energy. Provocation of atrial fibrillation triggers during ablation: does the use of general anesthesia affect inducibility? Safety of transvenous lead extraction according to centre volume: a systematic review and meta-analysis. Role of transesophageal echocardiography among patients with atrial fibrillation undergoing electrophysiology testing. Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis. The Practice of Electroconvulsant Therapy: Recommendations for Treatment, Training and Privileging. Benefits of the laryngeal mask for airway management during electroconvulsive therapy. Moderate hyperventilation prolongs electroencephalogram seizure duration of the first electroconvulsive therapy. Dexmedetomidine blunts acute hyperdynamic responses to electroconvulsive therapy without altering seizure duration. Anesthesia and electroconvulsive therapy: a retrospective study comparing etomidate and propofol. A systematic review and meta-analysis of randomized controlled trials of adjunctive ketamine in electroconvulsive therapy: efficacy and tolerability. To those concerned with the federal budget and personal expenses, medical care for the aged threatens to bankrupt the nation. Nevertheless, the impact of aging on the practice of medicine is far-reaching and profound, and therefore cannot be ignored. Just as children are not “little adults,” the older patient is truly different from the younger adult counterpart. All caregivers, including anesthesiologists, should be knowledgeable of at least some aspects of aging in order to provide intelligent deviation from their standard practice. Basic information is more available than ever before, much of it electronically from the American Society of Anesthesiologists (www. In reality, caring for an older patient is rarely dull, if for no other reason than their diverse and fascinating lives. Anyone with a passing interest in physiology should enjoy the application of aging physiology to anesthetic management. Yes, their care is often time-consuming, stressful, and requires extra effort, but more often than not it provides the anesthesia caregiver the opportunity to truly practice medicine and make a positive impact on a vulnerable patient’s life. On the examination of the 2006 inpatient and ambulatory4 procedure data, there were an estimated 73 million surgical and nonsurgical procedures performed in the United States after exclusion of procedures that were unlikely to have involved anesthesia services. Yellow bar = age above 65; purple bar = age 65 to 74; green bar = age 75 or above for years 1940 to 1970, and age 75 to 84 from 1980 on; red bar = age 85 or above.
Best colchicine 0.5 mg
The external layer of the rectus sheath is marked on both sides antibiotic you cant drink alcohol 0.5 mg colchicine fast delivery, and a short-beveled needle is inserted at a point where the border of the rectus sheath intersects an imaginary horizontal line at the level of the umbilicus bacterial cell wall order genuine colchicine online. The external oblique antibiotics vs surgery appendicitis generic colchicine 0.5 mg buy on-line, internal oblique, and transversus abdominis muscles can be seen lateral to the rectus muscle; the internal oblique muscle is on the same plane as the rectus muscle. The intended position of injection is the lateral space between the posterior rectus sheath and the rectus muscle. Color Doppler may be used to identify and avoid the inferior epigastric vessels that run through the rectus muscle. The needle is aimed through the external and internal oblique muscles toward the lateral gutter of the rectus muscle directly superior to the posterior rectus sheath. With this approach, the needle does not penetrate the belly of the rectus muscle and avoids the inferior epigastric vessels. The hypoechoic spread will be seen between the posterior rectus sheath and the rectus muscle. Bottom: Needle insertion sites (X) for abdominal field blocks, color-coded according to the top figure. Placement of a transverse probe over the midline reveals the rectus abdominis and layers of the abdominal wall. The injection site is located at about 1 to 2 cm medial and 1 to 2 cm inferior to the anterior superior iliac spine. The needle is inserted from the anterior abdomen (vertically) until a fascial click is detected, presumably at the junction of the internal oblique and transverse abdominis muscles. The cross-sectional view of the ilioinguinal nerve can be captured lying between the internal oblique and transverse abdominis muscles. They used a position about 5 cm cranial and slightly posterior to the anterior superior iliac spine, where both nerves have been shown to be present between the above-mentioned muscles with a 90% probability. The nerves appear hypoechoic with many hyperechoic dots and a distinct hyperechoic rim (Fig. They have an oval, somewhat “boomerang” shape and appear embedded between the fascicular hypoechoic- appearing muscles. In the more cranial position, the iliac bone, with its hyperechoic border and dorsal shadowing, may be captured on the medial aspect of the screen. The thin external oblique muscle lies superficial at the cranial position, but it may not be visible more inferiorly. Either one or two injections can be made, depending on the number of distinct nerves localized. Injecting lateral to the most laterally positioned ilioinguinal nerve, or medial to the iliohypogastric nerve, has been reported as one method to block these nerves individually. Penile Block Penile block is used in children and adults for surgical procedures of the glans and shaft of the penis. The dorsal nerves (terminal branches of pudendal nerve; S2–S4) lie bilaterally on the outer aspect of the dorsal arteries of the penis. From the base of the penis, the nerves divide several times and encircle the shaft of the penis before reaching the glans. This block is often performed as a circumferential infiltration of the root of the penis 2438 (ring block). Two skin wheals are raised at the dorsal base of the penis, one on each side just below and medial to the pubic spine. For a complete ring of infiltration, an additional 5 mL (adults) is infiltrated in the subcutaneous tissue around the underside of the shaft. Epinephrine- containing solutions should not be used to avoid compromising penile circulation. Figure 36-32 Arrangement of relevant anatomy for ultrasound-guided ilioinguinal/iliohypogastric nerve block. Lower Extremity Combined blocks of the lumbar and sacral plexuses provide effective surgical anesthesia to the entire lower extremity. Prior to the 1990’s, an “anterior lumbar block” approach (also referred to as the “femoral three-in-one” approach), which was first described by Winnie et al in 1973, had been commonly performed. This block was based on the assumption that a large volume local anesthetic injection into the femoral nerve sheath would 2439 produce spread of the solution proximally to anesthetize the obturator and lateral femoral cutaneous nerves as well.
Sehydrin (Hydrazine Sulfate). Colchicine.
- Are there safety concerns?
- Dosing considerations for Hydrazine Sulfate.
- How does Hydrazine Sulfate work?
- Use with chemotherapy for non-small cell lung cancer.
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96209
0.5 mg colchicine otc
Creative staffing at higher ratios of coverage may be required to manage patient surges virus lyrics discount colchicine online american express. Other places anesthesia providers can assist in delivery of health care during a disaster include: • Triage outside the hospital (who better to manage the pain or labored respiration of the expectant patient? For example infection hyperglycemia discount colchicine 0.5 mg on line, on October 26 antimicrobial spray cheap 0.5 mg colchicine with mastercard, 2002, terrorists held 750 hostages at the Nord-Ost Theater in Moscow. Many believe that the authorities instilled nebulized or volatile carfentanil into the air ducts of the opera house, thereby immobilizing the terrorists. Unfortunately, because of the incapacitating effect of the carfentanil, the hostages became victims too. Patients were transported from the theater to hospitals without any treatment prior to arrival. Ideally, anesthesiologists or other health-care providers with an opioid antagonist such as naloxone should have been readily available and present at the site to 4234 manage both casualties. Anesthesiologists’ basic understanding of physiology and pharmacology, airway skills, fluid resuscitation expertise, and ability to manage ventilators and provide anesthesia, both in and out of the operating rooms, is invaluable. He or she will not know where they will be working until they report to the hospital and the command and control center has developed a plan to manage the event. Other entrances to the hospital are typically closed during a mass casualty event for the purposes of maintaining control of the numbers of patients that might present and to allow for decontamination of patients, if necessary, avoiding exposure of hospital personnel to contagious agents or transferrable substances, such as nerve agents. The lack of such control and decontamination of the Tokyo subway sarin attack victims in 1995 resulted in a number of health-care workers becoming ill by absorbing sarin from patients who had not been properly decontaminated. Not only were they unable to work but they also19 became patients themselves, increasing the number of patients requiring care and consuming resources. Triage If assigned to triage patients, the anesthesiologist will be expected to classify patients into four groups—those requiring immediate care, delayed care, minimal care (first aid only), and expectant (no care, or comfort care only). The latter group includes those expected not to survive, or, because of the number of patients arriving, those for whom there are not adequate personnel or resources to adequately resuscitate without jeopardizing the lives of other patients who would not receive the care they require and for whom the prognosis is more favorable (Fig. Experience has taught that initially triage officers are conservative; they try to save as many patients as possible, but over days, if not hours, they gain experience and become better at identifying patients for whom resources exist to improve outcome. He or she will have to assess and decide if patients fall into one of the four groups. Such a site must be situated so that newly arriving patients are not exposed to the sight of dying patients. Anesthesiologists may well be assigned to provide such care because of expertise in managing airways, in establishing intravenous access for the administration of medications, and our familiarity with the available anxiolytic and analgesic medications. As emotionally difficult as the process of identifying or managing patients not expected to survive is the assessment of patients who may have been injured or affected during a disaster but who do not appear to require treatment, yet might require delayed care. Various symptoms may be exhibited, depending on the type of agent, which will direct the appropriate therapy: • Chemical (nerve) agents: If only headache, meiosis, rhinorrhea, and lacrimation after exposure, patients can be decontaminated (see later) and dismissed. Patients with dyspnea, bronchospasm, or arrhythmias will require treatment with atropine. There are several new therapies in development for mitigation of the effects of radiation exposure. Decontamination In most situations, those with proper training decontaminate people in contact with chemical agents or radioactive materials—the decontamination is normally performed first and then patients are evaluated and triaged. The principle is to limit the exposure of the patient to the agent and prevent contamination of caregivers. Off-gassing of some chemical agents can be problematic, especially with large numbers of exposed patients awaiting decontamination. Consideration should be given to providing lightweight “escape hoods” (available from multiple vendors) to reduce respiratory exposure before decontamination can be performed. The decontamination process is usually fairly straightforward; clothes are removed and individuals are washed with copious amounts of water (the contaminated water and apparel can present quite a challenge! Patients with severe chemical agent poisoning may present with acute respiratory failure requiring emergency tracheal intubation.
Purchase 0.5 mg colchicine with visa
Genetic Variants and Risk for Postoperative Lung Injury Prolonged mechanical ventilation (inability to extubate patient by 24 hours postoperatively) is a significant complication following cardiac surgery antibiotics history buy generic colchicine 0.5 mg online, occurring in 5 antibiotic quadrant discount colchicine uk. The use of such outcome predictive models incorporating genetic information may help stratify mortality and morbidity in surgical patients antibiotic names for uti order colchicine 0.5 mg on line, improve prognostication, direct medical decision-making both intraoperatively and during postoperative follow-up, and even suggest novel targets for therapeutic intervention in the perioperative period. Pharmacogenomics and Anesthesia Interindividual variability in response to drug therapy, both in terms of efficacy and safety, is a rule by which anesthesiologists live. In fact, much of 432 the art of anesthesiology is the astute clinician being prepared to deal with outliers. The term pharmacogenomics is used to describe how inherited variations in genes modulating drug actions are related to interindividual variability in drug response. Pharmacokinetic variability refers to variability in a drug’s absorption, distribution, metabolism, and excretion that mediates its efficacy and/or toxicity. Pharmacodynamic variability refers to variable drug effects despite equivalent drug delivery to molecular sites of action. This may reflect variability in the function of the molecular target of the drug, or in the pathophysiologic context in which the drug interacts with its receptor-target (e. Historically, characterization of the genetic basis for plasma pseudocholinesterase deficiency in 1956 was of fundamental importance to anesthesia and the further development and understanding of genetically determined differences in drug response. With growing public concern over intraoperative awareness, understanding the mechanisms responsible for this variability may facilitate implementation of patient-specific preventative strategies. Evidence of a genetic basis for increased anesthetic requirements is beginning to emerge, suggested for instance by variability in the immobilizing dose of sevoflurane (as much as 24%) in populations with different ethnic (and thus genetic) backgrounds. Several preclinical proteomic analyses have identified in a more unbiased way a group of potential anesthetic targets for halothane, desflurane, and sevoflurane, which should provide the37 38 39 434 basis for more focused studies of anesthetic binding sites. Such “omic” approaches have the potential to evolve into preoperative screening profiles useful in guiding individualized therapeutic decisions, such as prevention of anesthetic awareness in patients with a genetic predisposition to increased anesthetic requirements. Genetic Variability in Pain Response Similar to the observed variability in anesthetic potency, the response to painful stimuli and analgesic manipulations varies among individuals. Increasing evidence suggests that pain behavior in response to noxious stimuli and its modulation by the central nervous system in response to drug administration or environmental stress, as well as the development of persistent pain conditions through pain amplification, are strongly influenced by genetic factors. Various strains of knockout mice lacking target genes like neurotrophins and their receptors (e. In addition to the genetic control of peripheral nociceptive pathways, 435 considerable evidence exists for genetic variability in the descending central pain modulatory pathways, further explaining the interindividual variability in analgesic responsiveness. Although such genetic variation in drug metabolizing enzymes or drug targets usually result in unusually variable drug response, genetic markers associated with rare but life-threatening side effects have also been described. Of note, the most commonly cited categories of drugs involved in adverse drug reactions include cardiovascular, antibiotic, psychiatric, and analgesic medications, and interestingly, each category has a known genetic basis for increased risk of adverse reactions. There are more than 30 families of drug-metabolizing enzymes in humans, most with genetic polymorphisms shown to influence enzymatic activity. Pharmacogenomics is emerging as an additional modifying component to anesthesia along with age, gender, co-morbidities, and medication usage. Specific testing and treatment guidelines allowing clinicians to appropriately modify drug utilization (e. Conclusions and Future Directions The Human Genome Project has revolutionized all aspects of medicine, allowing us to assess the impact of genetic variability on disease taxonomy, characterization, and outcome, and individual responses to various drugs and injuries. Mechanistically, information gleaned through genomic approaches is already unraveling longstanding mysteries behind general anesthetic action and adverse responses to drugs used perioperatively. Furthermore, genetic profiling of drug metabolizing enzymes, carrier proteins, and receptors, using currently available high-throughput molecular technologies, will enable personalized choice of drugs and dosage regimens tailored to suit a patient’s pharmacogenetic profile. At that point, perioperative physicians will have far more robust information to use in designing the most appropriate and safest anesthetic plan for a given patient. Although one of the aims of the Human Genome Project is to improve 439 therapy through genome-based prediction, the birth of personal genomics opens up a Pandora’s box of ethical issues, including privacy and the risk for discrimination against individuals who are genetically predisposed for a medical disorder. Such discrimination may include barriers to obtaining health, life, or long-term care insurance, or obtaining employment. Thus, extensive efforts are made to protect patients participating in genetic research from prejudice, discrimination, or uses of genetic information that will adversely affect them. To address the concerns of both biomedical research and health communities, the U. Senate has approved in 2003 the Genetic Information and Nondiscrimination Act, which provides the strong safeguards required to protect the public participating in human genome research.
Buy 0.5 mg colchicine with mastercard
These test statistics are called F ratios antibiotics side effects 0.5 mg colchicine purchase mastercard, after Ronald Fisher; the critical values for the F test statistic are taken from the F probability distribution that Fisher derived bacteria types of bacteria 0.5 mg colchicine purchase otc. The F test is actually asking several questions simultaneously: Is group 1 different from group 2; is group 2 different from group 3; and is group 1 different from group 3? As with the t test antimicrobial news discount colchicine 0.5 mg line, the F test statistic is a ratio; in general terms, the numerator expresses the variability of the mean values of the three groups, whereas the denominator expresses the average variability or difference of each sample value from the mean of all sample values. The formulas to create the test statistic are computationally elegant but are rather hard to appreciate intuitively. The F statistic has two degrees of freedom, denoted m and n; the value of m is a function of the number of experimental groups; the value for n is a function of the number of subjects in all experimental groups. If the null hypothesis is rejected and it is accepted that there are differences among the groups tested, how can it be decided where the differences are? Robustness and Nonparametric Tests Most statistical tests depend on certain assumptions about the nature of the distribution of values in the underlying populations from which experimental samples are taken. For the parametric statistics, that is, t tests and analysis of variance, it is assumed that the populations follow the normal distribution. However, for some data, experience or historical reasons suggests that these assumptions of a normal distribution do not hold; some examples include proportions, percentages, and response times. What should the experimenter 478 do if he or she fears that the data are not normally distributed? The experimenter might choose to ignore the problem of nonnormal data and inhomogeneity of variance, hoping that everything will work out. Such insouciance is actually a very practical and reasonable approach to the problem. Parametric statistics are called robust statistics; they stand up to much adversity. To a statistician, robustness implies that the magnitude of type I errors is not seriously affected by ill-conditioned data. Parametric statistics are sufficiently robust that the accuracy of decisions reached by means of t tests and analysis of variance remains very credible, even for moderately severe departures from the assumptions. Another possibility would be to use statistics that do not require any assumptions about probability distributions of the populations. Such statistics are known as nonparametric tests; they can be used whenever there is very serious concern about the shape of the data. The basic concept behind nonparametric statistics is the ability to rank or order the observations; nonparametric tests are also called order statistics. Most nonparametric statistics still require the use of theoretical probability distributions; the critical values that must be exceeded by the test statistic are taken from the binomial, normal, and chi-square distributions, depending on the nonparametric test being used. The nonparametric sign test, Mann–Whitney rank sum test, and Kruskal–Wallis one-way analysis of variance are analogous to the paired t test, unpaired t test, and one-way analysis of variance, respectively. The currently available nonparametric tests are not used more commonly because they do not adapt well to complex statistical models and because they are less able than parametric tests to distinguish between the null and alternative hypotheses if the data are, in fact, normally distributed. There are general guidelines that relate the variable type and the experimental design to the choice of statistical test (Table 7-5). Binary Variables Confidence Intervals on Proportions Categorical binary data, also called enumeration data, provide counts of subject responses. In the population from which the sample is taken, the ratio of responders to total subjects is a population parameter, denoted π. As with other data types, π is usually not known, but must be estimated from the sample. Because the population is not generally known, the experimenter usually wishes to estimate π by the sample ratio p and to specify with what precision π is known. This question was proposed by Henley and Lippman-Hand to discuss the interpretations of zero16 numerators using the 3 over n rule. Consider an observational study that reports no morbidity in 167 patients receiving a new intravenous anesthetic.
Generic 0.5 mg colchicine with amex
The effects of intra- abdominal hypertension are not limited just to the intra-abdominal organs antimicrobial benzalkonium chloride cheap colchicine 0.5 mg fast delivery, but rather have an impact either directly or indirectly on every organ system in the body virus 10 states buy generic colchicine 0.5 mg line. However bacteria belong to what kingdom quality 0.5 mg colchicine, the pathophysiologic model developed in the adult population and in the animal studies is sound. We are legitimated to translate it in the pediatric cohort of patients keeping in mind some distinctive features as the differences in compartment compliance and perfusion pressure. Once abdominal contrac- tion is ruled out by sedation or neuromuscular block, the volume of instillation inside the bladder is the main source of bias. The correct volume of instillation in the adult population has been investigated by several papers as a volume too great Table 12. Eijke [16] estimated the best volume to infuse in the bladder by an analysis of the bladder compliance curve with an increasing volume of normal saline. Considering the bladder compliance as a sigmoid curve, they defned the optimal volume as the one used to reach the lower infection point. Pressure bag Pressure transducer F/F adapter Anti-bacterial filter 3-ways stopcock 3-ways stopcock Abdominal 3-ways Pz. This system is essentially made by a regular urinary catheter, a three-way stopcock with attached on one end to the Foley catheter and on the others to a pressure transducer zeroed at midaxillary line and an infusion bag. The lack of awareness of this syndrome in the pediatric intensivist community has been already discussed [5, 6]. In 1948 Gross proposed a staged closure of the abdomen, and since then the concept of “abdominal domain” or better to “regain abdominal 148 D. Rizzo [21] proposed in 1996 the intraoperative vesical pressure to guide wall closure. They had no difference between the staged and primary closure groups in terms of frequency of complications, time to begin oral feeding, and length of parenteral nutrition or hospital stay. The ideas at the basis of the use of a staged abdominal closure are to gain space by allowing graft or bowel edema to reabsorb or to wait for the abdominal cavity to stretch around the organs with a second-intention closure without compromising graft perfusion. Gupte [26] reports that since 2005 staged closure of the abdomen and pre-transplant abdominal tissue expanders were applied routinely whenever a mismatch between donor and 12 The Open Abdomen in Infants and Children 149 recipient was found. Delayed primary closure of the abdomen in pediatric liver transplantation was con- sidered an emergency therapy when important bowel edema, massive transfusion, great donor graft mismatch, or bowel distension were detected [28]. Staged closure of the abdominal cavity was reported as routinely performed by 25% of European pediatric surgeons [31] if a “tense clo- sure” was suspected. Interestingly, important abdominal impairment was detected for pressures as low as 10 mmHg [30, 32], questioning the value of 20 mmHg that is currently felt as a safe threshold for closing the abdomen in other neonatal diseases (i. Rollins [18] in his cohort of seven patients that underwent laparotomy had no survival, whereas Prodhan [35] had two survivors out of four patients treated with peritoneal catheters. However, Rollins sug- gests possibly better results had decompressive laparotomies been performed earlier. Results from the international conference of experts on intra-abdominal hypertension and abdominal compartment syndrome. Results from the international conference of experts on intra-abdominal hypertension and abdominal compartment syndrome. Intra-abdominal hypertension and the abdominal compartment syndrome: updated con- sensus defnitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Survey of intensive care physicians on the recognition and management of intra-abdominal hypertension and abdominal compartment syndrome. Recognition and man- agement of abdominal compartment syndrome among German pediatric intensivists: results of a national survey. The polycompartment syndrome: towards an understanding of the interactions between different compartments! Increased intra-abdominal, intrathoracic, and intracranial pressure after severe brain injury: multiple compartment syndrome. Comparison of indirect methods of measuring intra- abdominal pressure in children.
Colchicine 0.5 mg buy low cost
If it is necessary to deliver more than 30% oxygen to the patient antimicrobial proteins colchicine 0.5 mg buy with visa, then delivering 5 to 15 L/min of air under the drapes will dilute the oxygen treatment for dogs eating rat poison purchase discount colchicine line. It is important that the drapes be arranged in such a manner that there is no oxygen buildup beneath them bacteria fermentation buy colchicine amex. Venting the drapes and having the surgeon use an adhesive sticky drape that seals the operative site from the oxygen flow are steps that will help reduce the risk of a fire. It is potentially possible to discontinue the use of oxygen before the surgeon plans to use the electrocautery or laser. This would have to be done several minutes beforehand in order to allow any oxygen that has built up to dissipate. If the surgeon is planning to use the electrosurgery or laser during the entire case, this may not be practical. Some newer surgical preparation solutions can contribute to surgically related fires. In a laboratory recreation, they found that if the DuraPrep had been allowed to dry completely (4 to 5 minutes), the fire did not occur (Fig. The other problem with these types of preparation solutions is that small pools of the solution can accumulate if the person doing the preparation is not careful. The alcohol in these small puddles will continue to evaporate for a period of time, and the alcohol vapors are also extremely flammable. Flammable skin preparation solutions should be allowed to dry at least 3 minutes, and puddles removed before the site is draped (Fig. If the preparation solution gets into the patient’s hair, then drying can take up to 60 minutes. It is important to bear in mind that halogenation of hydrocarbon anesthetics confers relative, but not absolute, resistance to combustion. Even the newer, “nonflammable” volatile anesthetics can, under certain circumstances, present fire hazards. For example, sevoflurane is nonflammable in air, but can serve as a fuel at concentrations as low as 11% in oxygen and 10% in nitrous oxide. Therefore, it would not interact with sevoflurane and undergo an exothermic chemical reaction. Therefore, if a tracheal tube is on fire, disconnecting the circuit from the tube or disconnecting the inspiratory limb of the circuit will usually result in the fire immediately going out. Once the fire is extinguished, the airway is inspected via bronchoscopy, and the patient reintubated. If the fire is on the patient, then extinguishing it with a basin of saline may be the most rapid and effective method to deal with this type of fire. If the drapes are burning, particularly if they are paper drapes, then they must be removed and placed on the floor. Paper drapes are impervious to water; thus, throwing water or saline on them will do little to extinguish the fire. Once the burning drapes are removed from the patient, the fire can then be extinguished with a fire extinguisher. In sequence: First, the team should generally attempt to extinguish a fire on, in, or near the patient. The patient should then be evaluated and any injuries should be appropriately managed. Electrosurgical unit monopolar pencil electrode applied to operative site at start of surgery. If three or more of these factors are present, then a high fire risk situation exists, and the team should take necessary steps to prevent a fire. Other safety measures to prevent a fire include keeping the oxygen concentration as low as clinically possible. Notify the surgeon if an oxygen- enriched environment is in proximity to an ignition source. Ensure that alcohol preps are dry before draping the patient, and moisten all sponges that are in proximity to an ignition source. Panels2 A and B illustrate a 3-dimensional model, and Panels C and D show the polymer prototype. Operating room fire prevention: creating an electrosurgical unit fire safety device. If there was an engineering solution to mitigate this problem, then fire safety would be greatly enhanced.
Vak, 23 years: Outside of the tegument is a lipid bilayer membrane (envelope) containing several virus-encoded glycoproteins. General anesthetics inhibit excitatory synaptic transmission in a variety of preparations, including sympathetic ganglia,56 olfactory cortex,57 hippocampus, and spinal cord. Clinical outcomes of 5358 patients undergoing direct open bypass or endovascular treatment for aortoiliac occlusive disease: a systematic review and meta-analysis. Finally, appropriate logis- tical reasons involved a planned relaparotomy to remove packs, reassess bowel viability (e.
Marik, 32 years: The potential benefts of robotic technology include benefts include relative ease of use and low cost. The operator read the float position beside an adjacent63 but erroneous scale in both cases. Customarily, the indications are classified either as absolute or as relative (Table 38-1). In addition to soft tissue edema of the pharynx and peripharyngeal hematoma, blood or debris in the oropharynx may be responsible for partial or complete airway obstruction in the acute stage of these injuries.
Brontobb, 39 years: An empiric laparotomy is indicated in patients undergoing a damage control strategy from traumatic abdominal injury, particularly, when reoperation during the next 24–48 h is required, and in the presence of severe visceral edema. Artif Organs and the distal vessel is connected end-to-side 2016;40(12):E305-E306. Tese are used to lengthen the femur: the orthopedic surgeon places complicated patients, and many of them will present after two rings in the femur with expansible screws and another numerous surgical failures. The anesthesiologist’s role in management of obstetric hemorrhage includes both maternal resuscitation and provision of anesthesia for cesarean delivery, cesarean hysterectomy, or dilation and curettage.
Abe, 51 years: Selec- mizing artifacts caused by blood from the sphenoid sinus tive adenomectomy is achieved in all patients. B, Mittelman apatite is a good grafting material because of its biocompat- Pre Jowl-Chin implant augments the pre-jowl sulcus without increasing chin projection. The elevated pH, as a result of the reaction, can be observed with a color pH indicator in the testing medium. However, in end- stage liver disease serum albumin function is quantitatively and qualitatively decreased.
Ayitos, 25 years: O’meara D, Wilbe K, Leitner T, Hejdeman B, Albert J, Lundeberg J (2001) Monitoring resis- tance to human immunodeficiency virus type 1 protease inhibitors by pyrosequencing. Taveaux prepared succinylcholine among a series of choline esters, which they had injected into rabbits to observe their cardiac effects. Capnography Respiratory rate and apnea may be detected by measuring the carbon dioxide tension in the anesthesia breathing circuit. Insulinlike Verh Dtsch Ges Chir 1908;37:80–85 growth factor-I stimulates the growth of rat thyroid cells in culture 8.
Peratur, 37 years: Careful aspiration is important but may not prevent unintentional injection of local anesthetic into the subdural space. The midesophageal four-chamber view is one of the most recognizable and valuable diagnostic views. If they are then intermittently exposed to a radiofrequency wave, the nuclei change their alignment. Although the closed claims data is useful, it has significant4 limitations, including its retrospective nature and the lack of a denominator.
Nemrok, 44 years: Plus disease means that the blood vessels of the retina have become enlarged and twisted, indicating a worsening of the disease. Intensive Care Med 37(7):1059– Costa Fda S (2013) Reference range of uterine 1068. If the patient lives 5 Te patient must understand that he/she is in more than 2 h away from the implanting center, it charge of his/her life. Endoscopic Equipment and Setup The endoscope video monitor and tower are placed above the patient’s head on the patient’s left side to allow for com- fortable viewing by the surgeon and the assistant who will be standing on the patient’s right side.
Jose, 50 years: Int J Artif Organs 38:468–470 tality after short-term ventricular assist device place- 20. Relationship of carbapenem restriction in 22 university teaching hospitals to carbapenem use and carbapenem-resistant Pseudomonas aeruginosa. Sir Robert Macintosh later described the circumstances of its discovery in an appreciation writing regarding the career of his technician, Mr. Cardiovascular Effects The hemodynamic effects of propofol are dose-dependent and more significant after an induction dose than during a continuous infusion.
Esiel, 59 years: Fortunately, the development of factor inhibitors is much less prevalent in patients with hemophilia B than in patients with hemophilia A, and occurs in only 1% to 6% of severe patients. In cases of inadvertent dural puncture, catheters may be threaded into the subarachnoid space for continuous spinal analgesia. This increase in cerebrospinal fluid pressure causes an increase of retinal venous pressure, which may cause retinal hemorrhages. The net effect is to improve the V/Q matching, resulting in a reduced amount of venous admixture and improved arterial oxygenation.
Tempeck, 54 years: In general, delayed sur- deposition, posterior cervical fat, acanthosis nigricans, acne, gical intervention is reasonable, while at frst the disturbed hirsutism, thin skin, ecchymoses, and violaceous striae; the electrolyte water balance has to be stabilized, especially the last feature is present in only 50% of patients, and its ab- frequently observed hyponatremia; furthermore, “acute” sence does not exclude the presence of the syndrome. Automation has also increased the capabilities of integrating these assays into the larger clinical laboratory. Slower rates of mechanical ventilation2 (8 to 10 breaths min−1) should be used to allow sufficient time for exhalation. Over the past several decades, as a result of both surgical and anesthetic advances, the surgical experience has again changed.
Makas, 28 years: Currently, available 4306 temporary pacemakers only allow biventricular pacing through a Y connection of the two ventricular epicardial wires to the ventricular output of the box. Pressure is applied evenly to the gel to ensure good and even contact between gel and membrane. J Clin Endocrinol Metab 1999;84:2458–2467 anesthetized and unparalyzed acromegalic patients. The predictive value of skin testing in the diagnosis of local anesthetic allergy.
8 of 10 - Review by R. Kor-Shach
Votes: 324 votes
Total customer reviews: 324
References
- Leissner J, HohenfellnerR, Thuroff JWet al: Lymphadenectomy in patients with transitional cell carcinoma of the urinary bladder: Significance for staging and prognosis. BJU Int 2000; 85:817-823.
- Yamal JM, Rubin ML, Benoit JS, et al. Effect of hemoglobin transfusion threshold on cerebral hemodynamics and oxygenation. J Neurotrauma. 2015;32(16):1239-1245.
- Marshall VC, Howden BO, Thomas AC, et al. Extended preservation of dog kidneys with modifi ed UW solution. Transplant Proc. 1991;23:2366.
- Ross W, Rowe T, Glisson B, et al. Role of topoisomerase II in mediating epipodophyllotoxin-induced DNA cleavage. Cancer Res 1984;44(12 Pt 1):5857-5860.
- Mariani PJ. Pseudoephedrine-induced hypertensive emergency: Treatment with labetalol. Am J Emerg Med 1986;4:141.