Andrew W. Helfgott, MD, MHA, CPE
- Professor and Chief
- Division of Maternal-Fetal Medicine
- Department of Obstetrics and Gynecology
- Medical College of Georgia
- Augusta, Georgia
Xeloda dosages: 500 mg, 500 mg
Xeloda packs: 10 pills, 20 pills, 30 pills, 40 pills

Order xeloda 500 mg
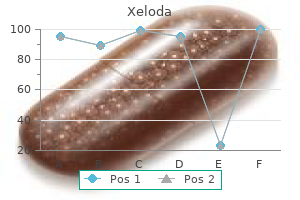
Methods that have been used include adhesive tape women's health center in lebanon pa generic xeloda 500 mg otc, suture fixation women's health tips now purchase 500 mg xeloda visa, and specially designed silicone fixation devices women's health issues by age order 500 mg xeloda with amex. The yellow catheter on the top is used for measuring intravesical and urethral pressures. Recording of Urinary Leakage The method of urine leakage determination should be recorded. It should be stated whether the urinary leakage is recorded as a signal with the pressure measurements or is dependent on the subject pressing an event marker button or completing a urinary or leakage weight diary (Figure 35. Instructions to the Patient Detailed instructions as to recording of symptoms, identification of catheter displacement, and hardware failure should be given to the patient. It is the recommendation that such verbal instructions should be reinforced by written instructions, and, in addition to the hardware built into the system, the patient is provided with a simple diary to record events. The specific points that should be addressed with regard to pressure measurement are as follows: 509 Figure 35. If the technical quality of the traces is less than perfect, then, although the investigation may yield valuable clinical information, the information that can still be derived from the traces is very much dependent on the experience of the team and the person responsible for the interpretation of the assessment. Phase Identification Depending on the purpose of the investigation, markers must be placed to identify voluntary voids and allow differentiation of such events from involuntary events, which may be associated with changes in recorded pressure. The protocol of the investigation should state specifically the point at which the markers identifying commencement and cessation of a voluntary void are placed. Analysis of the voiding phase follows the same principles and terminology used during conventional pressure–flow investigation. The system is used to check catheter position before fixation and connection to the portable unit. In addition, data from the portable recording unit are transferred to this system after the ambulatory measurement has ended. In addition, it has proven very valuable as a double check for both patient and equipment compliance. Typical events occurring during the filing phase are detrusor contractions, urethral relaxation, and episodes of urgency and incontinence. Catheters are placed in the bladder, urethra, and rectum and brought into optimal position. After fixation, catheter positions should be checked again and, in case necessary, corrected for optimization of the pressure–flow traces. Procedure The patient should use the timer on the ambulatory box, not her own watch. In the event of a toilet visit, the button is pressed when entering the bathroom or at the starting point of voiding and pressed again once voiding has finished. When fluids are consumed, or during an episode of urgency, the relevant buttons are used. Instructions for the use of the event buttons should be included on the diary sheet, as should the instructions on how to fill out the diary. The traces and diary can be interpreted with the patient still present or at a later stage. If the traces are interpreted in a later stage, the diary must have been filled out correctly by the patient and event markings been recorded correctly. If symptoms suggesting cystitis are persistent or urine becomes offensive, the patient should seek advice from her doctor. No significant difference was seen when comparing stress incontinence rates in both groups (p = 0. The difference in observations between both assessment types could be explained by the technique used. However, it cannot be excluded that the vesical catheter itself is a nonphysiological trigger resulting in a higher incidence of detrusor overactivity during ambulatory urodynamics [38]. The fact that the bladder produces involuntary detrusor contractions in response to the small flexible catheters during an ambulatory urodynamic measurement itself might indicate a higher excitability of the bladder sensory function or a decreased central inhibition of the urethra–detrusor facilitative reflex contractions in the filling phase [43]. The authors concluded that in women with stress incontinence ambulatory urodynamics remains the investigation of choice.
500 mg xeloda otc
Lactose intolerance Obesity Dehydration and Fever Atherosclerosis Relatively poor learning abilities Disinclination to feed womens health 8 healthy eating instagram xeloda 500 mg order with amex, fever and drowsiness may occur Family breakup and in some newborns about the third or fourth day of life women's health clinic newark ohio cheapest xeloda. Administration of additional feeds of feeding problems as regurgitation menstruation 18th century order xeloda in united states online, vomiting, suckling and water over about 12 hours brings down the temperature. If a fulminant infection is seriously suspected in an Too little feed, too heavy feed, too frequent feed, infant who is immature or is at risk for one or the other wrong feeding technique, poor respect to bottle hygiene, reason, antibiotics are recommended even if a specifc site etc. An insecure mother may not develop the much- showing that he has been hungry for long. Dissatisfed with the amount made available to him, he usually cries needed warm emotional relationship with such a baby. Irritability of an infant during the mother’s menstrual periods is well-known observation. Whether it is related to Bottle Addiction fall in the breast milk supply, mother’s irritability or some It is not infrequent to see mothers grumbling that “the little substances in breast milk during menstruation that cause rascal refuses to part with the bottle” even at 24 months. Little do they realize that the reason is indeed rooted in their failure to have replaced the bottle by spoon and cup Colic at about 6 months or little earlier. It is unwise to have a Sometimes a baby begins crying soon after birth, parti- baby on bottle after 1 year of age. Tis condition Overfeeding has been christened three months colic, or evening colic. Most infants, None of the above mentioned causes seems to account for as a rule, refuse to accept excess feed and pushing the feed its occurrence. It is borne out by the presence of exaggerated bowel do manage to give the baby larger and larger feeds. Such a baby is unhappy, vomits large amount of Change in Bowel Habit feed, has fatty diarrhea and keeps crying. Infants on cow milk, especially if underfed and given Inexperienced Mothers inadequate fuids and sugar may pass constipated stools, Not all mothers are good enough and well prepared for the i. Teir nervousness somehow or following rectal examination, can lead to anal crack or infuences the baby. Tis interaction may lead to rather unhealthy water, some brown sugar and glucose to the intake. In obstinate constipation, one should exclude We have observed such a situation very often in the case cretinism and congenital megacolon (Hirschsprung of young educated mothers who opt to live by one or to the disease). Tey just try to Recurrent episodes of loose motions are often due to blindly ape it rather than follow sound advice and their own poor bottle hygiene. C Clinical Problem-solving Review 1 This 3-day-old baby girl’s 22-year-old mother has a problem. She has inverted nipples that are a roadblock in proper attachment of neonate’s mouth to the nipple. The mother should manually stimulate, stretch and roll out the nipples to make them prominent several times a day, especially before offering the feed. If the condition fails to resolve in a couple of weeks, the plastic syringe method may be employed. Hoffman technique consists in placing the thumbs at the right and left edges of the areola. This maneuver is repeated at least four times and then again with the thumbs at the top and bottom of the areola. Breast shells, worn prenatally, assist in solving the problem of fat or inverted nipples. Current recommendations are exclusive breastfeeding for the frst six months of life, appropriate complementary foods thereafter and continuing breastfeeding as long as possible. Once a nutritionally adequate and safe diet without breast milk can be provided, breastfeeding may be discontinued. Writing Committee, Infant and Young Child Subspeciality Chapter of Indian Academy of Pediatrics/Human Milk Banking Association. T e efects are of the highest order in the resource- Stunting 51% 45% limited countries such as India. T ese substandard survivors are likely to sufer from consequences such as poor quality of life (QoL), low cognitive development and learning skills over and above other handicaps. Considerable morbidity and (at times mortality) accom- panies nutritional anemias and other micronutrient and vitamin defciencies, directly or indirectly.
Buy xeloda 500 mg lowest price
In this instance menstrual cycle day 6 buy discount xeloda 500 mg on line, A3 represents delay of A1 exiting the sinus node women's health clinic rochester ny xeloda 500 mg buy without prescription, which has not been affected women's health clinic toledo ohio buy xeloda 500 mg free shipping. The A1-A2 at which complete interpolation is observed probably defines the effective refractory period of the most peripheral of the perinodal tissue, because the sinus impulse does not encounter refractory tissue on its exit from the sinus node. In this instance, A1-A2 + A2-A3 = A1-A1, and sinus node entrance block is said to exist. Even after autonomic blockade, the range of “normals” reflects the previously described fallibility of the assumptions of indirect measurements as well as the variability of pacing site relative to the site of sinus impulse formation. B: The same patient is paced at a cycle length of 675 msec leading to a postdrive return cycle length of 805 msec followed by a sinus cycle length of 705 msec. Further work using endocardial recordings from the intact canine heart confirmed the ability to record diastolic phase 4 slope, followed by slow upstroke culminating in a 59 rapid atrial electrogram. Subsequently, several investigators developed techniques to record electrograms from 46 60 61 62 human subjects with and without sinus node dysfunction. Two techniques have been employed; in one the catheter is positioned at the junction of the superior vena cava and right atrium in the region of the sinus node, and the other – which appears more reliable and from which more stable recordings can be obtained – requires that the catheter be looped in the right atrium with firm contact at the region of the superior vena cava and atrial junction (Fig. This latter method, which produces firm contact against the atrial wall, produces an atrial injury potential simultaneously with the recording of the sinus node electrogram. The reported frequency for obtaining node electrograms ranges considerably, from 40% to 90%. Those studies using methods similar to the second method report higher success rates. In addition, filter settings play a prominent role in the ability to record stable electrograms that are not obscured by marked baseline drift. Use of low-end filter settings of 1 Hz or more produces diminution or loss of the sinus node electrogram. The high-end or low-pass filter frequency can be set at 20 or 50 Hz, the latter being more commonly employed. Using these techniques, which are time consuming, a stable sinus node electrogram without significant baseline shift can be recorded. However, in my opinion, the frequency and ease with which this recording can be made have been exaggerated. We obtained stable sinus node electrograms in only 50% of an unselected population of patients. It has been recognized that factors that produce encroachment of the T and U wave on the P wave make it P. If such patients are included in the unselected population of patients in whom sinus node electrogram requirements are attempted, the incidence of adequate recordings will be markedly diminished. Baseline drift is an important problem in preventing the recording of stable electrograms for measurements. Such drifts are more marked in young children and in those with significant cardiopulmonary disease and exaggerated respirations. Such baseline sinus drift can be obviated by using a low-end filter frequency of 0. There is an early return beat (A3), with an atrial activation sequence and P-wave morphology identical to that of sinus rhythm. Since the A1-A3 (650 msec) is less than the spontaneous sinus cycle length (790 msec), A3 is probably due to reentry in the region of the sinus node. On the right, a second method of obtaining the sinus node electrogram is shown with a catheter-looped positioning of the recording electrodes at the sinus node area. The human sinus node electrogram: a transvenous catheter technique and a comparison of directly measured and indirectly estimated sinoatrial conduction time in adults. When sinoatrial conduction is slowed, an increasing amount of the sinus node potential becomes visible before the rapid atrial deflection is inscribed. Sinoatrial block is said to occur when the entire sinus node electrogram is seen in the absence of a propagated response to the atrium. Another aspect of the sinus node electrogram that has been evaluated is the total time of 63 diastolic depolarization. The major values of this technique have been: (a) to improve our understanding of physiologic phenomena related P. As previously mentioned, the development of pauses during sinus rhythm has either been called sinus arrest or sinus exit block, depending on whether the next sinus impulse or impulse is a multiple of the basic sinus cycle length. The use of sinus node electrograms has shown us that in most instances sinoatrial block is present because persistence of the sinus node electrogram at similar or slightly slower rates has been observed (Fig.
Purchase xeloda in india
A and B: This results in the ability of single extrastimuli to depolarize the ventricles at coupling intervals <360 msec unusual women's health issues order 500 mg xeloda with amex. This can be done by demonstrating a slowing of the sinus rate and the absence of hypotension during administration of the agent (see slowed atrial rate in Fig 11-208) menopause the musical cheap xeloda master card. This arrhythmia cannot be terminated by beta blockers women's health clinic portlaoise 500 mg xeloda order free shipping, vagal maneuvers, or adenosine. Many other features of this particular tachycardia support reentry, including an inverse relationship of a coupling interval of the extrastimuli inducing the arrhythmia and the onset of the tachycardia, the ability of a variety of Class I agents to P. B: Rapid pacing is shown to reverse the wavefront of activation and refractoriness until a stable collision of both wavefronts occur during fixed fusion (entrainment), but still only resets the tachycardia. While the extrastimulus was delivered at the same coupling interval as in (A) it reaches the tachycardia circuit relatively earlier than in (A). In addition, the reset circuit has a smaller excitable gap by the degree of prematurity with which it was reset. B: Overdrive ventricular pacing at a paced cycle length to 300 msec (S1-S1) is also unsuccessful. Sustained ventricular tachycardia in coronary artery disease—Evidence for reentrant mechanism. Occasionally, verapamil shortened the cycle length and prolonged the duration of the tachycardias (Fig. As stated earlier, adenosine and vagal maneuvers can also terminate such arrhythmias (Fig. This phenomenon, which is almost always associated with a slower tachycardia and prolongation of conduction by the agent, would not be expected if the mechanism were triggered activity. In addition, as noted earlier, facilitation of induction of arrhythmias—particularly when associated with long pauses between the extrastimulus inducing the arrhythmia and the onset of the arrhythmia—is most consistent with reentry. While currently catheter mapping is essentially an endocardial procedure, there is increasing interest in the role of epicardial mapping. In addition to its clinical utility, mapping provides information about the mechanism of the tachycardia. The demonstration of a complete reentrant circuit has been nearly impossible in the catheterization laboratory using standard catheters and point-by-point mapping 46 352 353 371 374 375 376 and, in the past, required detailed intraoperative mapping. Future enhancements to ascertain stability of the intracavitary balloon and facilitate more uniformly accurate spatial localization of the electrogram and separate ablation catheter may make this system more useful, particularly in ablating unstable rhythms. The ability to 386 display several thousand derived electrograms can allow for the demonstration of complete reentrant circuits, realizing that much of the data is interpolated from the 64 “recording poles. It appears useful for focal tachycardias and can give the impression of reentrant excitation but is limited to the epicardium and cannot follow activity in the intraventricular septum or the endocardium in densely infarcted areas. There are, in addition observations, using standard catheters and recording equipment that suggest reentry. These include mapping a diastolic pathway or demonstrating diastolic bridging or continuous electrical activity, 1 43 44 197 200 369 which is requisite to maintain the tachycardia. These can take the form of 10 to 12 pole standard catheters with standard ring electrodes (1- to 2-mm circumferential electrodes with 2- to 4-mm inter(mid)-electrode distance), the PentArray catheter from Biosense Webster (20 very small electrodes 2 to 5 mm apart), and the Rhythmia 64 pole (smallest electrodes at very low impedance) small basket (see figures of catheters in Chapter 1). These systems allow for the collection of large amounts of data in much shorter period of time. While this mass of information can theoretically provide more accurate information, the automated annotation algorithms for unipolar and bipolar recordings need more refining to make them accurate. Furthermore, variable contact of the multipolar electrodes detract from their accuracy. Methods to assess contact are currently being developed to enhance the accuracy of the findings. When activation mapping of the tachycardia per se cannot be accomplished because of hemodynamic instability, indirect methods of tachycardia localization can be employed (e. Optimally, the patient should be hemodynamically stable during the tachycardia so that the map may be completed. If a sustained arrhythmia is hemodynamically unstable, mapping can still be accomplished by starting and stopping the tachycardia after data acquisition at each site. If more than one morphologically distinct tachycardia is induced, it should also be completely mapped. A schema of the left ventricle, which we use for mapping, has been previously shown in Figure 11-16. Obviously one of several 3D electroanatomic systems can be used to define the location of each recorded electrogram in space and correlate it to an anatomic shell.
Xeloda 500 mg purchase on-line
The second evaluated whether basic skills warm-up improved performance of complex tasks menstrual flow is actually sloughed off buy cheap xeloda line. They found that regardless of the level of expertise menopause excessive bleeding buy xeloda with a mastercard, all surgeons benefitted from the surgical warm-ups as a 25%–45% range in reduction of error was noted menopause reset cheap xeloda 500 mg buy line. Even though performance improved in the fatigued individual, it did not return to baseline performance levels characteristic of the rested state. These findings suggest that the preoperative warm-ups may become a new surgical standard, assuring optimal care of the patient during surgery. At that time, Satava predicted surgical simulation would steadily evolve and mature from its relatively infant to assume the breadth and scope of its use in the fields of aviation and the military [137,138]. In view of continued growth in the use of robotics in almost every surgical subspecialty and the evolution of robotic platforms, the continued use of simulation and telementoring to enhance surgical performance is thereby assured [139]. They agreed that such training provides opportunities for surgeons to train without harming patients. They found good evidence that use of part task trainers shortens the learning curve, especially for newer trainees. Evidence they gathered in their review further bolstered the argument for formally incorporating simulation-based training of technical and nontechnical skills into a urology training curriculum. They subsequently developed a checklist prototype and piloted its use in 18 vascular surgical procedures performed in Canada. Using a pre- /postintervention study design and trained observers, a total of 172 surgical procedures were observed. They found that the mean number of communication failures per procedure significantly decreased from 3. The checklist briefings revealed knowledge gaps, promoted learning, and triggered actions among members of the team. The investigators also appreciated the impact of a traditional silo approach of nurses, surgeons, and anesthesiologists working independently; staff shortages, educational demands, and economic pressures had on surgical workflow; and the potential for jeopardizing patient safety. All health-care providers involved with the patient along the surgical pathway were taught how to use the tool and complete their sections. However, some users did not complete the tool due to lack of consequences and some users strongly advocated for creating an electronic version and have it integrated with their hospital information system. Of about 5000 thousand articles published on this topic between 1995 and April 2011, they identified 22 for inclusion. Overall compliance with using the tools ranged from 12% to 100% (mean 75%) and a range of 70%– 100% (mean 91%) for the time-out. High compliance was associated with involvement of multidisciplinary surgical staff in the process of development. Critical factors for successful implementation included explaining to staff why and how the checklist would be used, coupled with real-time coaching, feedback, audits, ongoing education and training, and support of hospital administrators and leaders. Checklists were associated with improved health outcomes such as decreased surgical complications and surgical site infections, increased detection of potential safety hazards, and improved communication among members of the operative team about relevant and important information about the patient. They confirmed that successful implementation of checklists involved factors such as administrative and leadership support, training staff on their use, adapting the checklist to incorporate staff feedback and avoid duplicate efforts in data collection. Barriers to effective implementation included confusion about practical use, managing workflow efficiently and the beliefs and attitudes of staff, especially surgeons, toward checklists. The surgical safety checklist provides an opportunity for every team member to speak up and offer up information of concern, allowing everyone involved to be on the same page and situationally aware of what to expect. The extent to which such teamwork contributes to the impact of the checklist and the extent to which patients should be included are rich areas for research. Diagnostic error includes delayed, missed, or wrong diagnosis, failure to use indicated tests, and failure to act on the results of monitoring or testing. Berner and Graber [155] noted that such errors occur in every specialty, ranging from 2% in perceptual specialties (such as radiology and pathology) to as much as 15% in the clinical specialties. Their review of the literature led them to conclude that overconfidence, a trait of human nature, does exist among physicians. Physicians believe that diagnostic error exists but underestimate the likelihood of their occurrence, especially in their own decision-making processes. This is evident in physician disregard for decision aids or tools or diagnostic or treatment guidelines or algorithms. If a clinician is uncertain about a clinical situation, then formal or informal consultative assistance is more likely to be requested, especially when the case is complex. However, Berner and Graber believe most cognitive errors arise when cases seem to be routine and physicians are certain about the decisions they have made.
Xeloda 500 mg buy otc
The explosion can be thought of in terms of a compressive shock that is due to the formation of a vapor globe within noncompressible blood menopause show discount xeloda online, followed by rebound shocks with the collapse of the globe menopause rosacea order cheapest xeloda. High-speed cinematography has shown dramatic changes in cardiac shape during this “explosion women's health clinic vernon bc purchase on line xeloda. If one measures current and voltage during the delivery of the discharge, there will be a sudden increase in voltage and decrease in current as the vapor globe forms, as a result of a rise in impedance. The high temperature of the electrical arc, which may approach several thousand degrees, results in pitting of the distal and occasionally more proximal electrodes of the catheter. Despite the high temperature associated with the arc, there is insignificant heating of the tissue, suggesting that thermal damage is not the primary mechanism by which the fulguration works. Most investigators believe that it is the direct electrical effect that disrupts myocardial membranes, resulting from either dielectrical breakdown, change in membrane lipids, or physical compression and mechanical disruption of the membrane. Barotrauma is undesirable, despite the fact that it may play a role disrupting and/or separating myocardial fibers in some types of ablation. Barotrauma associated with fulguration has consistently caused rupture of the coronary sinus when energy is delivered there and has been associated with rupture of other cardiac structures, myocardial dysfunction, and arrhythmias. A greater disruption is seen when proximal electrodes are used to deliver the energy instead of the distal tip. Thus, there is reasonable evidence that most electrode catheters demonstrate some current leakage, particularly when multiple shocks are delivered. This may lead to misdirected shocks and clinical failures, as well as to unnecessary barotrauma. More work is necessary to develop catheters capable of withstanding fulguration-type shocks if this technique is going to be used in the future. Pathologically, fulguration shocks produce a somewhat patchy contraction band necrosis. The volume of damage done generally correlates with the amount of energy delivered and is relegated to the electric field. In this technique, cell membranes are exposed to high-voltage electrical fields, resulting in nonthermal, nonbaratraumatic damage to the cell membrane resulting in cell death. In experimental ablation studies, this technique appears to be relatively specific for myocardial tissue damage. At 3 weeks, intimal hyperplasia was not detected and coronary angiography demonstrated no stenosis. Because of the small surface area of the tip of the catheter relative to the cutaneous patch, the current density will be high at the tip and low at the patch. The heat that is generated is transferred to the subjacent cardiac tissue primarily by conduction and to a minor extent by radiation, which decreases by the fourth power of the distance from the catheter tip. Effective heating of the myocardium is critically dependent on catheter contact and stability as well as on the surface area of the catheter tip. Poor contact or stability will lead to heat loss to the blood pool and failure to generate adequate myocardial temperatures despite application of high voltage/power. Although a larger surface area (length of the catheter tip electrode) can lead to greater lesion size, it will require delivery of greater power, since the greater surface area will be subjected to greater convective heat loss to the blood pool to which it has greater exposure. Thus maximum lesion size using a 4- to 5-mm ablation tip can be accomplished using a maximum power of 50 W while up to 100 W may be required to achieve maximal lesion size using an 8- to 10-mm catheter tip. A variety of deflectable catheters are available that can have different arcs of curvature, bidirectional deflecting capabilities (with similar or different lengths of deflection), rotational capability, or magnetic sensors (Biosense) that allow for precise localization in three dimensions (Fig. A drop of impedance of 5 to 10 Ω is a sign of conductive heating to the subjacent tissue. If the temperature at the electrode-myocardial interface increases excessively, a rise in impedance develops because of gas formation caused by vaporization of the blood around the catheter tip. Impedance rise also causes formation of coagulum on the catheter tip, and it is mandatory to remove the catheter and wipe off the coagulum, which is a potential source of emboli. If the tissue is heated to >100°C, steam will be generated as a consequence of boiling within the myocardium. This often can be detected as an audible popping sound, which will just precede a marked rise in impedance. The initial modification of ablation catheters was use of thermocouples or thermistors imbedded near the catheter tip P. This modification was deemed necessary because of the inability to relate the power used to tissue heating. These are closed loop-temperature control systems such that the power is automatically adjusted to maintain a desired temperature.
Diseases
- Chromosome 9, partial trisomy 9p
- Microcephaly brain defect spasticity hypernatremia
- Antley Bixler syndrome
- Hepatitis C
- Gamstorp episodic adynamy
- Herpes virus antenatal infection
- Pyruvate kinase deficiency, liver type
- Lymphedema, congenital
- Pulmonary arterio-veinous fistula
- Glomerulosclerosis
Xeloda 500 mg buy without prescription
After admission to the surgical care area women's health clinic grenada ms purchase 500 mg xeloda, preoperative broad-spectrum antibiotics are administered parenterally at least 1 hour prior to surgery pregnancy due date calculator purchase xeloda overnight. After the administration of regional or general anesthesia pregnancy ultrasound at 6 weeks order xeloda on line amex, the patient is placed in the dorsal lithotomy position. The lower abdomen and vagina are clipped and prepared with a 10-minute scrub with a povidone-iodine or Hibiclens solution. A posterior-weighted vaginal retractor is placed for exposure of the anterior vaginal wall. Lateral labial retraction sutures or a self-retaining retraction system may be utilized for retraction of the labia. The incision should extend from a point midurethra to the proximal bladder neck (Figure 78. With sharp dissection, the vaginal wall is dissected from the underlying urethra on either side. Blunt finger dissection may be used to separate the endopelvic fascia from its lateral attachments to the pubic rim in a woman who has not had prior surgery. The fascia should be swept from lateral to medial, so as to gain access into the retropubic space (Figure 78. The retropubic space should be entered sharply in women who have had previous surgery using dissecting scissors positioned against the pubic symphysis angled toward the ipsilateral shoulder. When the retropubic space is dissected bilaterally, final mobilization of the bladder neck and urethra is completed. Next, the anterior aspect of the proximal urethra and bladder neck is separated from the fascial attachments to the pubic symphysis. Blunt finger dissection or sharp dissection may accomplish this component of the procedure. The sharp dissection should be performed in the midline immediately inferior to the pubic symphysis (Figure 78. At this stage of the procedure, aggressive dissection may lead to unintentional bladder or urethral tear. Some authors, however, including Salisz and Diokno have reported successful repair of this type of injury with subsequent successful implantation of the device [10]. After circumferential dissection of the proximal urethra and bladder neck, a right-angle clamp is passed around the urethra from left to right. The cuff measuring tape is passed around the bladder neck and the circumferential dimension of the bladder neck is assessed. Using a larger cuff size is preferred if there is a concern about exact dimension exists. Using a right-angle clamp, the appropriate-sized cuff is placed around the bladder neck (Figure 78. If the pump is to be placed in the left labia, the cuff is placed from left to right. The cuff is then locked in place and rotated 180° so that the locking button of the cuff lies anteriorly, opposite to the anterior vaginal wall (Figure 78. On the ipsilateral side to which the pressure-regulating balloon and pump mechanism will be implanted, a transverse suprapubic incision (approx 4 cm) is created. A straight clamp is passed using digital guidance from the suprapubic incision lateral to midline down to the ipsilateral side of the vaginal incision. The cuff tubing is grasped, and the clamp is withdrawn, pulling the tubing up into the suprapubic incision. Rubber-shod clamps should be utilized during this phase of the procedure to ensure that the end of the tubing is not open to the field. The anterior rectus sheath is then incised vertically and the retropubic space is developed adjacent to the bladder. The reservoir is then filled with sterile saline to a volume compatible with reservoir size and requirements for the unique individual (usually 22 mL). From the suprapubic incision, a subcutaneous tunnel is formed into the labia majora with a combination of blunt and sharp dissection. The pump is passed into the labia majora to reside at the level of the urethral meatus with the deactivation button facing anteriorly (outwardly). The tubing is trimmed to the appropriate lengths and the ends are irrigated to remove air or debris.
Cheap xeloda online mastercard
Convulsions along with tonsillitis menstruation in the bible order xeloda with a visa, pharyngitis breast cancer 30s buy cheap xeloda line, groups—(1) uncomplicated and (2) severe women's health clinic surrey bc discount generic xeloda uk. Clinical Features Critical Phase Incubation period is 5–6 days with a variation of 3–15 days. Between 3 and 7 days of onset of fever, though fever begins to subside, the child may develop severe manifestations Febrile Phase such as bleeding, shock, thrombocytopenia and high hem- Clinical illness begins after a period of 5–6 days (variation atocrit and even multiorgan dysfunction such as hepatitis, 3–15 days) of the bite preceded a day before by viremia myocarditis and encephalitis. During the course of viremia, the mosquito Tis phase with regression of fever by lysis and profuse can get infected following a blood meal on an infected sweating in 2–7 days is relatively faster in children. It becomes capable of transmitting the disease Convalescence is marked by generalized weakness. It is characterized by abrupt onset of high fever lasting 3–7 days, severe frontal headache, pain behind the It is a severe, often fatal, form of the disease, is almost eyes and muscle and joint pains. Other symptoms may exclusively limited to children in some Southeast Asian include loss of appetite, nausea, vomiting and diarrhea, a countries (including India). Te acute febrile illness (temperatures d 40°C), like that of dengue fever, lasts approximately for 2–7 days. Plasma z IgM: More dependable leakage is caused by increased capillary permeability and z IgG: Less useful. Clinical picture of dengue fever is supported by a posi- Liver damage manifests as increase in levels of alanine tive Hess test, raised hematocrit (20% above baseline), aminotransferase and aspartate aminotransferase, low leukopenia with relative lymphocytosis, reduced plate- albumin levels, and deranged coagulation parameters let count and increase in immature or unsegmented (prothrombin time, partial thromboplastin time). In persons with fatal dengue hepatitis, infection was Serology and virus isolation are ideal for confrmation demonstrated in more than 90% of hepatocytes and of the diagnosis (Box 18. Death may occur 8–24 hours In the event of hemorrhagic manifestations, meningo- after onset of signs of circulatory failure. Te most common coccemia, scrub typhus and leptospirosis become impor- clinical fndings in impending shock include hypothermia, tant diferential diagnosis. Fluid and electrolyte imbalance z Grade 2: Features of grade 1 + spontaneous bleeding into the Hyperpyrexia skin and/or from other sites. Shock z Grade 3: Circulatory failure manifested by rapid weak pulse, hypotension or low pulse pressure, cold, clammy skin and Febrile seizures. Management is more or less supportive and consists of: * Hess test is considered positive in suspected dengue if petechiae Controlling high fever with hydrotherapy/antipyretics above 20. Relieving pains with analgesics Fresh blood transfusion in case of accompanying Maintenance of fuid and electrolyte balance and bleeding manifestations nutrition (Figs 18. Te name chikungunya translates 347 Te concentrate can be prepared either by to that which bends up in the Makonde dialect of Tanzania, centrifugation of fresh whole blood or by automated describing the physical appearance of a patient with severe platelet pheresis. Hence, multiple platelet transfusion must employ fltered (leukocyte-reduced) Etiology platelet concentrates. Te Monitoring most common vector involved in transmission is infected Close monitoring of the patient is quite critical especially A. Vitals need to be measured every 30 minutes till they stabilize and thereafter every 2 hours. Epidemiology Central venous monitoring should be done in children It was in 1952–1953 that this virus was frst isolated in with features of shock. Platelets are chikungunya, in Kolkata in 1963–1964 and in Chennai in done daily till they show a rising trend. Autochthonous transmission has also been No respiratory distress documented in a limited area in Italy when an infected Platelet count greater than 50,000 cells/μL. For travelers, risk is highest in endemic areas during the rainy Prognosis season, when the density of the vector is highest. If com- plications are prevented or handled well, full recovery is a Clinical Features rule. Early recognition, careful fever, headache, fatigue, nausea, muscle pain, rash and monitoring and appropriate fuid therapy has resulted in pain in joints. Prognosis is poor in patients with acute phase last for 2–3 days which is followed by joint prolonged shock. So, early recognition of shock is of para- pain which is very severe, is polyarticular, migratory and mount importance. An itchy, transient Prevention maculopapular rash appears 4–8 days later over trunks and Antimosquito measures: A wholesale attack on the limbs.
Purchase 500 mg xeloda otc
This will hopefully allow visualization of bile indi- cating the duct is ready for cannulation womens health texas medicaid generic xeloda 500 mg without a prescription. At this point women's health big book of exercises ebook order xeloda 500 mg without a prescription, the Maryland forceps are placed in the 10 mm operating port to retract Hartmann’s pouch laterally menstrual cramps 5 weeks pregnant 500 mg xeloda buy amex. The assistant now holds these forceps to free the surgeon’s two hands allowing him to focus on the introduction of the cholangiogram clamp. This description is based on the use of the Olsen cholangiogram clamp with a smooth ureteral catheter no. This catheter should be introduced from the left lateral grasper port into the cystic duct. It is not necessary to introduce more than 1 cm of the catheter into the cystic duct, or no more than one black dot on the tip of the catheter. If the cholangiogram is normal, the clamp is removed and the clip applier introduced. The cystic artery is now clipped and divided as close as possible to the neck of the gallbladder. It is then possible to proceed with removal of the gallbladder from the liver bed. The best instrument for this is either a hook or better a fat electrical spatula that will “slice” the gallbladder from the liver bed. Opening of the gallbladder is an inelegant technical mishap, but studies have shown that it does not affect the outcome for the patient if all the bile is aspirated, the area is irrigated, and all the spilled stones are removed. In many instances an opening in the gallbladder occurs at the unperitonized area next to the liver bed. It is possible to grasp the gallbladder with the left grasper and apply a rotating motion on the opening exactly as one would do with a can-opener (the “spaghetti technique”), which will usually control the bile leak through a small opening. If the tear is large, the only solution is to grab it and insert an Endoloop (Fig. If neither the spaghetti technique nor insertion of an Endoloop closes the opening, the only resource will be to suck out the contents of the gallbladder, limiting the spillage of stones, and fnally introduce a bag to retrieve the gallbladder. Spillage of stones can be managed by irrigating the area to allow the stones to foat on the surface. Removal of the stones will then be easier by sucking them using a 10 mm specifc suction cannula. Unfortunately the stones can easily obstruct the tubing, in which case the only option is to pick the stones up one by one and insert them in a bag. Abscesses forming around stones have been described, and the author considers it crucial to remove them all whenever possible, and to irrigate and aspirate the bile. The patient will then not suffer any complications from an incident that usually looks messy but rarely affects the postoperative course. Acute In acute gangrenous cholecystitis, removal of the infammatory adhesions from the fun- Gangrenous dus of the gallbladder is the frst step. This is accomplished by applying high-pressure Cholecystitis hydro-irrigation through the irrigation suction cannula to the edge of the gallbladder to open up planes, which are then further dissected using a grasper and scissors with cau- tery, staying away from the duodenum at all times. An additional 5 mm trocar for an irrigation suction device is routinely inserted at the left midclavicular line by the author (trocar E, Fig. When the fundus of the gallbladder has been identifed, it is possible Impacted Stone (Hydrops, Empyema, Early Mirizzi) 29 to make a small opening using electrical scissors and insert an irrigation suction device into the fundus to aspirate the contents of the gallbladder. This will ease the tension of the gallbladder and enable it to be grasped using graspers with tiny teeth. If this is not possible secondary to infammation in the porta hepatis, then a cholangiogram should be attempted through the neck of the gallbladder to visualize the anatomy. However, if this also is not feasible, and the cystic duct and the neck of the gallbladder have been clearly identifed, then one can proceed with the cho- lecystectomy. As a rule of thumb the aim should be to recognize the elements of the triangle of Calot within 45 min of beginning the dissection. If after that period of time the anatomy is still not clear, conversion should be the rule. As the gallbladder is being removed from the liver bed some bleeding may occur from the liver parenchyma, owing to diffculty in fnding the best plane of dissection. Compression should be applied using a 2 × 2 gauze, and a collagen hemostatic pad should be left in place on the liver bed. In some cases of gangrenous gallbladder there may not be an obvious plane of dissection.
Cheap xeloda 500 mg buy on-line
The limitation of strip chart recorders is difficult data storage and the fact that most centers are paperless womens health kc order 500 mg xeloda otc. A fixed cinefluoroscopic C-arm or a biplane unit is preferred to any portable unit because it always has superior image intensification and has the ability to reduce radiation by pulsing the fluoroscopy women's health tips for losing weight xeloda 500 mg lowest price. All equipment must be appropriately grounded menstruation bloating best purchase xeloda, and other aspects of electrical safety must be P. All electrophysiologic equipment should be checked by a technical specialist or a biomedical engineer and isolated so leakage current remains less than 10 mA. Recording and Stimulation Apparatus Junction Box The junction box, which consists of pairs of numbered multiple pole switches matched to each recording and stimulation channel, permits the ready selection of any pair of electrodes for stimulation or recording. This can be done by incorporating the capability of recording unipolar and bipolar signals from the same electrodes simultaneously on multiple amplifiers. Such systems have a limited number of groups of amplifiers and do not allow for the capability of older systems, which allowed one to record unipolar and bipolar signals from the same electrodes, even when numbering more than 20. Current computer junction boxes come in banks of 8 or 16 and thus, at best, could record only that number of signals. Recording Apparatus The signal processor (filters and amplifiers), visualization screen, and recording apparatus are often incorporated as a single unit. Custom-designed amplifiers with automatic gain control, variable filter settings, bank switching, or common calibration signals, etc. Most of the newer systems are computer-driven and do not have such capabilities as the system originally designed for us by Bloom, Inc. The number of amplifiers for intracardiac recordings can vary from 3 to 128, depending on the requirements or intentions of the study. Studies using basket catheters to look at global activation might require 64 amplifiers while a simple atrial electrogram may suffice if the only thing desired is to document the atrial activity during a wide complex tachycardia. I believe an electrophysiology laboratory should have maximum capabilities to allow for both such simple studies and more complex ones. The advantage of computers is that you can always have a 12-lead electrocardiogram simultaneously recorded during a study when the electrophysiologist is observing the intracardiac channels. In the absence of a computer system, a 12-lead electrocardiogram should also be simultaneously attached to the patient. This allows recording of a 12-lead electrocardiogram at any time during the study. In our laboratory we have both capabilities, that is, that of a computer-generated 12-lead electrocardiogram as well as a direct recording. In the absence of a computer, a method to independently generate time markers is necessary to allow for accurate measurements. The amplifiers used for recording intracardiac electrograms must have the ability to have gain modification as well as to alter both high- and low- band pass filters to permit appropriate attenuation of the incoming signals. This is critical for selecting a site for ablation that requires demonstration that the ablation tip electrode is also the source of the target signal to be ablated. The recording apparatus, or direct writer, is preferable if one desires to see a continuous printout of what is going on during the study. Most current computerized systems, however, only allow snapshots of selected windows. If one does have a direct writer, it should be able to record at paper speeds of up to 200 mm/s. While continuously recording information has significant advantages, particularly for the education of fellows, storage of the paper and limited ability to note phenomenon on line have led to the use of computers for data acquisition and storage. Such computerized systems, as noted above, store amplified signals on a variety of pages. These data can be evaluated on- or off-line and can be measured at a distant computer terminal. This specifically means that in order for people to perform their measurements, there needs to be a downtime of the laboratory or a separate slave terminal that can be used just for analysis at a site distant from the catheterization lab. As stated earlier, computerized systems have the limitation of only saving that which the physician requests; much data are missed as a consequence.
Georg, 22 years: Primary stress urinary incontinence and pelvic relaxation: Prospective randomised comparison of three different operations. Complications include bleeding, infection, increased pain, hematoma, wound dehiscence, vaginal stenosis, scar tissue formation, and Bartholin duct cyst formation.
Potros, 39 years: In a study by Wendy Gantt (A-14), undergraduate nursing students were given a standardized mathematics test to determine their mathematical aptitude (scale: 0–100). When the eggs hatch, maggots develop and are shown in this picture in varying sizes as small, white, and wormlike.
Yokian, 38 years: Currently, in those patients with supraventricular tachyarrhythmias the patients will be placed on a drug and discharged with an event recorder to monitor rhythm, rate, and intervals. Albendazole, 400 mg (200 mg for <2 years) daily for 5 Clinical Features days also gives gratifying results.
Deckard, 48 years: In the literature, the use of magnetic resonance imaging, transvaginal Doppler ultrasound, and hysterosalpingography for vesicouterine and vesicofallopian fistulas have been described [76,82]. A high index of suspicion is needed to ensure that all fistulous communications are identified, including those that communicate with nonuro- genital organs or structures.
Torn, 45 years: Affected individuals produce abnormal dystrophin, a protein found on the sarcolemma of muscle fibers. The classic skin closure with 30 cm, an L- or J-shaped scar or a short inverted-T scar can only a vertical scar in every patient might result in many be used if the skin quality is still good.
Aidan, 40 years: The T2-weighted sagittal sequences are useful to show the bladder neck and the cervix. Role of retrograde His Purkinje block in the initiation of supraventricular tachycardia by ventricular premature stimulation in the Wolff-Parkinson-White syndrome.
Ramon, 62 years: In general, however, spontaneous termination with retrograde block in the bypass tract without any perturbations usually results during very P. An increase in maximum cystometric capacity and compliance and a decrease in maximal detrusor pressure were seen in the treatment group.
Kayor, 33 years: Idiopathic z Benign neonatal Partial Seizures z Childhood absence Tese are characterized by motor, sensory, autonomic z Juvenile absence or mixed manifestations secondary to focal lesions in z Juvenile myoclonic z Grandmal on awakening the brain. Total body circumference was lower sound which showed a thinning of the dermis [9 ].
Mine-Boss, 56 years: Hurwitz has gained consider- individuals who intend to lose weight should postpone body able experience in body contouring surgery and is an contouring surgery until they have been able to adequately innovator and an internationally recognized teacher in reduce and maintain their weight loss. Thus, analysis of the slope of the increasing portion of the resetting curve may be useful to determine during the electrophysiologic study in patients in whom antitachycardia pacemakers are considered a therapeutic option.
Ashton, 65 years: It may be related to the micturition cycle or associated with symptoms suggestive of urinary tract or sexual dysfunction [1]. Secretory IgA can neutralize viruses the number of effector cells and their killing by similar mechanism on mucosal surfaces.
Shakyor, 47 years: Therefore, it may not be possible to determine the effect of a drug on A-V nodal or His–Purkinje refractoriness if atrial refractoriness is prolonged beyond the A-V nodal refractory period. Nerves, blood vessels, lymphatic channels, and other deep structures may be injured.
Dargoth, 59 years: In the submalar zone, the soft tissues are swept off the shiny, white, glistening, fibrous tendon of the masseter mus- cle in an inferior and outward direction. Effects of gamma-aminobutyrate B receptor modulation on normal micturition and oxyhemoglobin induced detrusor overactivity in female rats.
8 of 10 - Review by L. Mannig
Votes: 158 votes
Total customer reviews: 158
References
- Knosp E, Steiner E, Kitz K, et al. Pituitary tumors with invasion of the cavernous sinus space: a magnetic resonance imaging classification compared with clinical findings. J Neurosurg 1993; 33:610-617.
- DeGroat WC, Douglas JW, Glass J, et al: Changes in somato-vesical reflexes during postnatal development in the kitten, Brain Res 94(1):150n154, 1975.
- Cooling LL, Walker KE, Gille T, et al. Shiga toxin binds human platelets via globotriaosylceramide (Pk antigen) and a novel platelet glycosphingolipid. Infect Immun. 1998;66:4355-4366.
- Rehabilitation Accreditation Commission. (2002). Standards manual: Medical rehabilitation (rev. ed.). Tucson, AZ: Author. Rosensteil, A. K., & Keefe, F. J. (1983). The use of coping strategies in chronic low back pain patients: Relationship to patient characteristics and current adjustment. Pain, 17, 33n44.
- Game X, Malavaud B, Alric L, et al: Infliximab treatment of Crohn disease ileovesical fistula, Scand J Gastroenterol 38(10):1097n1098, 2003.
- Weyand CM, Goronzy JJ. Arterial wall injury in giant cell arteritis. Arthritis Rheum 1999;42(5):844-53.
- Appling WD, Patrinely JR, Salzer TA. Transconjunctival approach vs. subciliary skin-muscle flap approach for orbital fracture repair. Arch Otolaryngol Head Neck Surg 1993;119: 1000.
- Ristau BT, OiKeefe DS, Bacich DJ: The prostate-specific membrane antigen: lessons and current clinical implications from 20 years of research, Urol Oncol 2013.