Scott Bolesta, PharmD, BCPS, FCCM
- Associate Professor, Department of Pharmacy Practice, Nesbitt School of Pharmacy, Wilkes University, Wilkes-Barre
- Investigator, Center for Pharmacy Innovation and Outcomes, Geisinger Health System, Danville
- Clinical Pharmacist in Internal Medicine/Critical Care, Pharmacy Department, Regional Hospital of Scranton, Scranton, Pennsylvania

https://www.geisinger.edu/research/research-and-innovation/find-an-investigator/2018/04/04/13/27/scott-bolesta
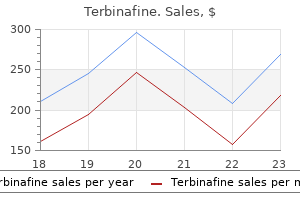
Terbinafine dosages: 250 mg
Terbinafine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Buy terbinafine once a day
Pneumonia is defined as an inflammatory process involving Mycoplasma pneumoniae and chlamydia are most lung parenchyma usually due to microorganisms fungus gnats root rot 250 mg terbinafine free shipping. Chlamydia trachomatis Group B streptococci Hemophilus influenzae Diagnosis Streptococcus pneumoniae Diagnosis of pneumonia is essentially clinical and seldom Listeria monocytogenes requires lab support antifungal vitamins herbs safe 250 mg terbinafine. Absence of past history of recurrent 3 months to 5 years Streptococcus pneumoniae cough and presence of fever with fast breathing is a Viruses (35%) hallmark presentation in clinical diagnosis of pneumonia fungus gnats definition discount generic terbinafine canada. Hemophilus influenzae It should always be remembered that there are no definite Staphylococcus differentiating markers between viral, bacterial and atypical Mycoplasma pneumoniae pneumonia. However, there are certain clinical clues which >5 years Streptococcus pneumoniae can help to nail down on etiological diagnosis (Table 8. Mycoplasma pneumoniae (24–30%) Viruses Characteristics of Viral Pneumonia Staphylococcus Staphylococcus pyogenes • Acute – sudden onset • Younger age • Preceding upper respiratory catarrh children older than 5 years of age accounting for 11–30% • Wheeze with crackles cases. Legionella is another rare and frequent cause of • Clinical evidence of hyperinflation with scattered atypical pneumonia. Significant proportion of pneumonia exudates on radiology due to segmental atelectasis. There is inhibition of phagocytosis by alveolar viral and bacterial etiology, nor they help in making decision macrophages. Thus, bacteria and other organisms invade of antibiotic choice; however, they may be useful tools for the lung parenchyma and produce a pneumonic lesion. At times it may not through hematogenous dissemination within the lung correlate with the clinical signs; there is also wide variation parenchyma. When the spread is hematogenous it is called in the interpretation by radiologists. Moreover, reliability “invasive or bacteremic pneumonia” and when the spread is in predicting the etiology is poor. However, the indicated in very severe disease, ambiguous picture, no pathogenesis is still ill understood till date. Diagnosis of pneumonia in feeding, tachypnea, respiratory distress is essentially clinical. Though symptom complex of fever, cough and rapid/difficult Microbiology—sputum culture or blood culture though breathing is classical presentation of pneumonia; it is prudent may be more specific, but the yield is very poor (10–15%). Pulse oximetry is a mandatory tool for monitoring the Non-severe pneumonia above the age of 3 months course of the disease in all the hospitalized children. Age First line Second line the choice of antibiotics though empirical should be 3 months to 5 years Amoxicillina Co-amoxiclav/Cefuroxime/ determined by age, severity, pre-disposing conditions if any and local epidemiology and drug resistance pattern. Child should • More than two risk factors be followed-up after 48 hours and if there is clinical • Comorbidities improvement the child should be continued with the • Associated complications same management. These include: • Exclusive breast feeding for first 6 months of life complicationsv • Weaning to solid foods after 6 months of age, preferably These include empyema, pneumothorax, bronchogenic with home-made foods dissemination, septicemia, osteomyelitis, multiple systemic • Avoidance of risk factors like overcrowded environment, abscesses, septic arthritis and meningitis. It accounts for a substantial portion of the Pathology pediatric burden of illness all over the world; it is the most Respiratory syncytial virus infection, results in loss of common and serious lower respiratory tract syndrome epithelial cilia and sloughing of epithelial cells in the that results in hospital admission among infants with airways. It is generally a self- epithelial cells, polymorphonuclear cells and lymphocytes limiting condition and is most commonly associated with within the airway. In acute bronchiolitis, sloughed epithelial cells, most frequently among children younger than 12 months neutrophils, and lymphocytes appear to be the major of age. Most cases occur between late autumn and early contributors to airway obstruction. These results in ventilation- Bronchiolitis is a clinical syndrome characterized by the perfusion mismatch causing hypoxemia, which is generally acute onset of respiratory symptoms in a child younger relieved by the administration of oxygen. Typically, the initial symptoms of upper respiratory tract viral infection, such as fever and coryza, clinical features progress within 4–6 days to include evidence of lower Clinical features are quite variable. Later disturbing cough, tachypnea, respiratory distress and poor feeding may develop depending on the severity of risk factors illness. In patients In bronchiolitis, an increased risk for hospitalization has been with adenovirus or influenza associated bronchiolitis, fever seen among infants attending day care, in those exposed is often higher than 39°C. On examination, infants typically to passive smoking and overcrowding in the household.
Crataegi Flos (Hawthorn). Terbinafine.
- What other names is Hawthorn known by?
- Are there safety concerns?
- What is Hawthorn?
- Decreased heart function, blood circulation problems, heart disease, abnormal heartbeat rhythms (arrhythmias), high blood pressure, low blood pressure, high cholesterol, muscle spasms, anxiety, sedation, and other conditions.
- Are there any interactions with medications?
- Treating heart failure symptoms when a standard form (LI132 Faros or WS 1442 Crataegutt) is used.
- Dosing considerations for Hawthorn.
- How does Hawthorn work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96529
Buy terbinafine 250 mg low cost
In the United States fungus food order genuine terbinafine, institutionalized patients fungus gnats outdoor potted plants order terbinafine 250 mg with mastercard, particularly the mentally challenged fungus diabetes buy terbinafine with a visa, have a high incidence of stool carriage and disease. An increased incidence has also been observed in sexually promiscuous homosexual males. The risk of amoebiasis is increased by travel to a developing country and is particularly high in individuals who reside in the endemic area for more than 1 month. Caused by Entamoeba histolytica, a parasite that contains ingested red blood cells and that is 10-60 mm in diameter. Parasite binds to galactose receptors on host cells and kills them, and causes flask-like ulcers. In the United States, the parasite is found in institutionalized patients, sexually promiscuous homosexuals, and tourists. Superficial bowel infection is associated with watery diarrhea and nonspecific gastrointestinal complaints. Invasive intestinal disease presents with the gradual onset, over 1-3 weeks, of abdominal pain and bloody diarrhea associated with tenesmus and abdominal tenderness. Amoebiasis can be mistaken for ulcerative colitis, and administration of corticosteroids can dramatically worsen the disease and lead to toxic megacolon. Patients complain of right upper quadrant pain and can also experience pain referred to the right shoulder. In amoebiasis, stools are always heme-positive, reflecting trophozoite invasion and destruction of bowel mucosa. In acute hepatic disease, alkaline phosphatase may not be elevated, but it rises in chronic hepatic infection. Clinical presentation depends on the degree of invasion: a) Watery diarrhea is associated with superficial infection. Treatment: Metronidazole or tinidazole for active disease; followed by paromomycin for luminal parasites. Previously, the diagnosis was made by identifying trophozoites or cysts in the stool. The latter test is positive in most patients who have had symptomatic disease for more than 1 week. However, antibodies persist for life and therefore are not helpful in detecting reinfection. Serum antiamoebic antibodies are elevated in 99% of patients with hepatic amoebic abscess. Amoebae are not generally seen, and are only rarely cultured because the parasite concentrates in the walls of the abscess. Invasive enterocolitis and hepatic abscess should be treated with oral metronidazole (750 mg every 8 hours for 10 days) or tinidazole (2 g daily, divided into three doses, for 3-5 days) (see Table 8. The trophozoite consists of a dorsal convex surface and a flat disk-shaped ventral surface composed of microtubules and microribbons, two nuclei, and four pairs of flagella. Trophozoites adhere to gastrointestinal endothelial cells, disrupt the brush border, cause disaccharidase deficiency, and induce inflammation. All of these mechanisms are thought to account for watery diarrhea and malabsorption. Patients with X-linked agammaglobulinemia have an increased risk of contracting severe prolonged disease, emphasizing the contribution of humoral immunity. Under unfavorable environmental conditions, Giardia can form dormant cysts that are excreted in the stool, and account for spread of disease. Trophozoites attach to gastrointestinal endothelial cells, causing malabsorption and inflammation. Giardia cysts are spread by contaminated water (and sometimes food) and person-to-person contact. A disease of campers (sterilization of water critical for prevention), daycare centers, and sexually active homosexuals. Giardiasis is found throughout the world; it is a common infection in the United States. Giardia cysts are most commonly spread by contaminated water, and multiple waterborne outbreaks have occurred in mountainous regions of the Northeast, Northwest, and Rocky Mountain states, and in British Columbia.
Cheap terbinafine online
Noninvasive Imaging Studies Noninvasive radiologic imaging is essential for the evaluation of patients with suspected biliary tract disease fungus gnats remedy purchase 250 mg terbinafine. Plain Abdominal Radiograph the plain radiographic features of biliary tract disease are usually nonspecific [1] fungus mega brutal purchase 250 mg terbinafine with mastercard. The most common bowel gas finding seen among patients with acute biliary disease is a generalized ileus fungus gnats in potting soil buy terbinafine now. Air in the biliary tree may result from a biliary-enteric fistula or surgical anastomosis, prior sphincterotomy, or infection with gas- producing organisms. It is a sensitive test for determining biliary ductal dilatation, acute cholecystitis, and >95% accuracy in detecting cholelithiasis. However, it has low sensitivity (25% to 60%) for detecting choledocholithiasis [3] because gas in the duodenum can obscure visualization of the distal bile duct. In the presence of cholelithiasis or gallbladder sludge, the findings of ductal dilatation, elevated liver enzymes, abdominal pain, and fever are strongly suggestive of cholangitis. Findings on ultrasonography that may indicate acute gallbladder disease include focal tenderness over the gallbladder, thickening of the gallbladder wall, and pericholecystitic fluid collections, but none is specific for cholecystitis. The technique may also detect other abnormalities, including liver lesions, pancreatic masses, abscesses, or ascites. Filling the gallbladder with radionuclide confirms cystic duct patency, virtually excluding the diagnosis of acute cholecystitis. False-positive examinations can be seen in patients with chronic cholecystitis, on long- term parenteral nutrition, or after prolonged fasting. Radionuclide scanning is also useful in identifying structural abnormalities of the biliary tree, such as significant bile duct leaks; evidence of radiotracer in the abdominal cavity is diagnostic of bile leak. It has a limited role in patients with poor hepatocellular function, complete biliary obstruction, or cholangitis, each of which prevents adequate uptake or excretion of the radiopharmaceutical into the biliary tree. It also allows detailed visualization of the pancreas for grading the severity of pancreatitis and assessing its complications, such as necrosis or pseudocyst formation. Magnetic Resonance Imaging the use of magnetic resonance cholangiopancreatogram images can be manipulated to display highly accurate representations of the pancreatobiliary system with high sensitivity (88% to 96%) and specificity (93% to 100%) for the diagnosis of choledocholithiasis [5], strictures, and tumors. It has limited value for detecting stones <6 mm, impacted stone at the ampulla, and dilated bile duct >10 mm [6]. Hepatobiliary scanning, on the contrary, provides physiologic information, primarily regarding patency of the cystic duct. Functional information can be especially important for patients with suspected calculous or acalculous cholecystitis. In brief, a side-viewing endoscope is passed through the mouth into the second duodenum, where the major ampulla is identified and cannulated. The biliary tree is then opacified with contrast injected through a catheter, allowing a retrograde cholangiogram to be obtained. Fluoroscopy and standard radiographs are used to examine the biliary tree and define abnormalities including stones, strictures, leaks, and obstruction. Endoscopic therapy, including stone removal, biliary drainage, or stricture dilatation, can be accomplished in the same setting. Rarely is it necessary to perform emergent biliary decompression at the bedside using portable fluoroscopy. Coagulopathies should be corrected before the procedure, especially if an endoscopic sphincterotomy (electrocautery incision of the sphincter of Oddi in the duodenal wall for stone removal or drainage) is anticipated. If coagulopathies cannot be satisfactorily corrected, a stent can be placed into the bile duct to allow drainage without performing a sphincterotomy. Major morbidity from the diagnostic procedure includes pancreatitis, cholangitis, perforation, and hemorrhage. The limitations of transabdominal ultrasonography are overcome with this modality because all areas of the biliary tree, including the intrapancreatic portion of the bile duct as well as the pancreas, can be imaged without interference from gas in the intestines. Decompression of the biliary tree via a percutaneous catheter is a highly effective method for rapid nonoperative and nonendoscopic biliary decompression. A guidewire is then passed into the biliary tree, the tract is dilated, and a drainage catheter is placed. Percutaneous biliary drainage is an invasive procedure, and acute complications, including hemorrhage, sepsis, and bile leakage, occur in 1% to 5% of patients [12]. In patients with a coagulopathy, a liver biopsy may be obtained by way of the hepatic vein using a transjugular approach or percutaneously using a sheath, embolizing the tract after completion of the biopsy [13]. The presentation of patients with cholangitis may range from intermittent low-grade fever to fulminant septic shock.
Order terbinafine with american express
These effects include blurred vision fungus gnats organic order terbinafine pills in toronto, dry mouth (the exception is clozapine antifungal medicine oral 250 mg terbinafine sale, which increases salivation) fungus killer for wood cheap terbinafine 250 mg with mastercard, confusion, and inhibition of gastrointestinal and urinary tract smooth muscle, leading to constipation and urinary retention. Other effects Blockade of α-adrenergic receptors causes orthostatic hypotension and light-headedness. The antipsychotics also alter temperature-regulating mechanisms and can produce poikilothermia (condition in which body temperature varies with the environment). In the pituitary, antipsychotics that block D receptors may cause an increase in2 prolactin release. Sedation occurs with those drugs that are potent antagonists of the H -histamine receptor,1 including chlorpromazine, olanzapine, quetiapine, and clozapine. Sexual dysfunction may also occur with the antipsychotics due to various receptor-binding characteristics. Weight gain is also a common adverse effect of antipsychotics and is more significant with the second-generation agents. Treatment of schizophrenia the antipsychotics are the only efficacious pharmacological treatment for schizophrenia. The first-generation antipsychotics are generally most effective in treating the positive symptoms of schizophrenia. Other uses the antipsychotic drugs can be used as tranquilizers to manage agitated and disruptive behavior secondary to other disorders. However, risperidone and haloperidol are also commonly prescribed for this tic disorder. Also, risperidone and aripiprazole are approved for the management of disruptive behavior and irritability secondary to autism. Many antipsychotic agents are approved for the management of the manic and mixed symptoms associated with bipolar disorder. Some antipsychotics (aripiprazole, brexpiprazole, and quetiapine) are used as adjunctive agents with antidepressants for treatment-refractory depression. Some metabolites are active and have been developed as pharmacological agents themselves (for example, paliperidone is the active metabolite of risperidone, and the antidepressant amoxapine is the active metabolite of loxapine). These formulations usually have a therapeutic duration of action of 2 to 4 weeks, with some having a duration of 6 to 12 weeks. Adverse effects Adverse effects of the antipsychotic drugs can occur in practically all patients and are significant in about 80% (ure 11. Extrapyramidal effects the inhibitory effects of dopaminergic neurons are normally balanced by the excitatory actions of cholinergic neurons in the striatum. Blocking dopamine receptors alters this balance, causing a relative excess of cholinergic influence, which results in extrapyramidal motor effects. The appearance of the movement disorders is generally time- and dose dependent, with dystonias occurring within a few hours to days of treatment, followed by akathisias occurring within days to weeks. Parkinson-like symptoms of bradykinesia, rigidity, and tremor usually occur within weeks to months of initiating treatment. Tardive dyskinesia (see below), which can be irreversible, may occur after months or years of treatment. If cholinergic activity is also blocked, a new, more nearly normal balance is restored, and extrapyramidal effects are minimized. Akathisia may respond better to β-blockers (for example, propranolol) or benzodiazepines, rather than anticholinergic medications. Tardive dyskinesia Long-term treatment with antipsychotics can cause this motor disorder. Patients display involuntary movements, including bilateral and facial jaw movements and “fly-catching” motions of the tongue. A prolonged holiday from antipsychotics may cause the symptoms to diminish or disappear within a few months. However, in many individuals, tardive dyskinesia is irreversible and persists after discontinuation of therapy. Tardive dyskinesia is postulated to result from an increased number of dopamine receptors that are synthesized as a compensatory response to long-term dopamine receptor blockade. This makes the neuron supersensitive to the actions of dopamine, and it allows the dopaminergic input to this structure to overpower the cholinergic input, causing excess movement in the patient. These agents cause a decreased uptake of monoamines into synaptic vesicles and depletion of monoamine stores, ideally focused on dopamine, to address the symptoms of tardive dyskinesia.
Discount terbinafine 250 mg overnight delivery
Phenytoin is highly protein bound; decreased protein binding increases the free antifungal plants discount terbinafine 250 mg buy on-line, pharmacologically active form of the drug and the Vd fungus jokes 250 mg terbinafine buy fast delivery. Because usually only total phenytoin levels are measured fungus juice order 250 mg terbinafine, toxicity from increased free phenytoin may occur at lower total phenytoin levels [3]. Hepatic metabolism of phenytoin follows first-order elimination kinetics, with an average half-life of 22 hours (range: 7 to 55 hours). When plasma levels exceed 10 μg per mL, metabolism follows zero-order elimination kinetics, yielding a much longer half-life. The enzyme system may be induced or inhibited by other drugs, inherited genetic disturbances, or liver disease [6,7]. Phenytoin has been successfully administered by the interosseous route in children with poor venous access. Maintenance dosing is usually 4 to 6 mg/kg/d in single or divided doses, although neonates may require higher doses (5 to 8 mg/kg/d) [9]. Death from isolated phenytoin ingestions is unusual but has been reported in young children with ingestions of 100 to 220 mg per kg. Clinical Manifestations Toxicity resulting from acute and chronic intoxication has a similar presentation. Patients with serum phenytoin concentrations between 20 and 40 μg per mL typically have nausea, vomiting, normal to dilated pupils, nystagmus in all directions, blurred vision, diplopia, slurred speech, dizziness, ataxia, tremor, and lethargy [10]. As phenytoin serum concentration increases, confusion, hallucinations, and apparent psychosis may develop. Severe toxicity with coma and respiratory depression occurs with serum concentration exceeding 90 μg per mL [11]. Paradoxical hyperactivity has been reported among patients with underlying neurologic deficits, with findings of dystonia, dyskinesia, choreoathetoid movements, decerebrate rigidity, and increased seizure activity [12]. Patients with baseline focal neurologic deficits may show contralateral abnormalities, including hemianopia, hemianesthesia, and hemiparesis. Cerebellar atrophy after acute intoxication with phenytoin that was not known to be attributed to hypoxia has been reported, however. Chronic use of phenytoin causes hyperglycemia, vitamin D deficiency and osteomalacia, folate depletion, megaloblastic anemia, and peripheral neuropathy. Other adverse drug events include altered collagen metabolism that causes hirsutism, gingival hyperplasia, keratoconus, and hypertrichosis [14]. Non–dose-dependent phenytoin adverse drug events include hypersensitivity reactions such as fever, rash eosinophilia, hepatitis, lymphadenopathy, myositis, a lupus-like syndrome, rhabdomyolysis, nephritis, vasculitis, and hemolytic anemia [4]. If the rate of infusion is slowed or temporarily halted, these effects usually resolve spontaneously but may persist for 1 to 2 hours [15]. Cardiovascular toxicity from phenytoin intoxication itself is rare, represents significant toxicity, and primarily occurs in patients with underlying cardiac disorders [16]. Diagnostic Evaluation Essential laboratory studies should include sequential serum phenytoin levels (free and total, if available) and levels of other anticonvulsant medications, particularly when enteric-coated dosage form is involved. The interval between drug levels should be based on factors such as severity of intoxication, rate of rise of levels, and time since exposure. Intervals should be more frequent during the initial evaluation phase, while absorption is still occurring, than later, during the postabsorptive phase. In stable patients whose drug levels have peaked or started to decline, it may be appropriate to obtain levels every 12 to 24 hours until they return to the therapeutic range. Recommended laboratory studies include serum complete blood cell count, electrolytes, blood urea nitrogen, creatinine, glucose, albumin, and liver function tests. In hypoalbuminemic patients, the corrected phenytoin concentration is equal to the measured phenytoin concentration multiplied by 4. Arterial blood gas, chest radiograph, head computed tomography, and lumbar puncture should be obtained as clinically indicated. Management Patients should have a rapid evaluation of respiratory status followed by intubation if hypoxia or risk of aspiration is present. Patients who are hyperglycemic from phenytoin intoxication can be treated with discontinuation of the drug; insulin therapy is rarely required. Flumazenil, the benzodiazepine antagonist, has no role in managing phenytoin intoxication, even if benzodiazepines are part of the polypharmacy overdose, as its use may increase the risk of status epilepticus, particularly in patients with a preexisting seizure disorder. Hypotension occurring during phenytoin infusion is treated with discontinuation of the infusion and administration of crystalloid. Treatment of cardiac dysrhythmias is supportive, with use of the appropriate antidysrhythmics when indicated.
Safe terbinafine 250 mg
If the obstruction is located in the rectum or rectosigmoid colon or duodenum antifungal horse purchase terbinafine 250 mg amex, it is reasonable to consider an endoscopic stent placement rather than surgery as the initial intervention antifungal vegetables buy terbinafine line. While the presence of carcinomatosis has been shown to increase the risk of failure of endoscopic stent placement for colonic obstruction fungus haematodes purchase discount terbinafine on-line, there is a 77% to 85% success rate [14–17]. For patients with a limited prognosis, an opportunity to avoid an operation that could involve either an intestinal diversion and ostomy or venting gastrostomy tube is an important consideration. For patients in whom it is felt that surgical or endoscopic relief of the bowel obstruction is not feasible, it is reasonable to evaluate them for a percutaneous endoscopic gastrostomy tube placement for gastric drainage. Surgical decision-making becomes more challenging for end of life patients who are not stable and require a decision regarding an emergent operation. It may be argued that this is not a purely palliative surgery consult as the surgical intervention has the potential to rescue the patient from a life-threatening complication of their life-limiting illness. On the other hand, it may also be considered palliative as it will not cure the patient of the underlying disease process. Needless to say, this is often an emotionally charged time, even for patients with long-standing illness such as advanced cancer, because they are now faced with the imminent risk of dying. Of the 376 patients who underwent emergency surgery for obstruction, the 30-day mortality rate was 18% with a 41% morbidity rate and 60% were discharged to an institution. While most patients will survive the initial operation, a substantial number will die soon after the surgery and many experience postoperative complications, reoperations, stays in nursing homes, or hospital readmissions. While these data are helpful for surgeons and caregivers to advise patients of the risks of surgery, set expectations for the postoperative experience, discharge location and overall survival, both at the time when the decisions is made for surgery and if complications occur, important data regarding whether the goals of the patients and families were met and whether or not they would make the same choice again are still severely lacking at this time. As with a lower intestinal obstruction, acute symptoms should be initially managed with nasogastric decompression, bowel rest, and intravenous resuscitation, including aggressive electrolyte repletion. Options for managing upper gastrointestinal obstructions include intraluminal stenting, surgical bypass, and decompression gastrostomy with possible feeding jejunostomy. Similar to colonic stenting, the potential benefits of duodenal stenting include immediate palliation of nausea and vomiting with a less invasive procedure than surgical bypass and earlier return to oral nutrition [20,21]. Stenting has been shown to provide a comparable survival outcome and equivalent morbidity and mortality to surgical bypass [22]. In a systematic review of the literature from 1990 to 2008 comparing endoscopic stenting with open surgical bypass, Ly et al. The major limiting factor for the endoscopic approach is being unable to pass the scope through the obstruction. The major complications reported are gastric ulceration, bowel perforation, biliary obstruction, stent dysfunction, and stent migration. Stent placement would be contraindicated in patients with multiple levels of intestinal obstruction and should be considered carefully for patients with peritoneal carcinomatosis who are at risk of more distal obstructions. For patients in whom stenting is not an option, surgical bypass can relieve both the symptoms of the obstruction and allow the patient to resume enteral nutrition. Surgical bypass, most commonly in the form of a gastrojejunostomy, can either be performed laparoscopically or through a relatively small upper midline incision. The estimated risk of morbidity and mortality from these procedures is 25% to 60% and 0% to 25%, respectively [22,23]. While surgical bypass is usually technically successful, patient selection with regard to preoperative nutritional status and life expectancy is imperative to the palliative success of this approach. For example, in addition to general surgical risks such as bleeding or infection, a patient with chronic gastric outlet or duodenal obstruction who is malnourished is at increased risk of a leak from the intestinal anastomosis. Other potential complications specific to gastric bypass include dumping syndrome, alkaline reflux gastritis, and delayed gastric emptying. Placement of a gastrostomy tube for decompression is another option for palliation of gastric outlet, duodenal and nonoperable small bowel obstruction or profound gastrointestinal dysmotility from carcinomatosis. Gastrostomy tubes can be placed either endoscopically, fluoroscopically, or surgically (either laparoscopic or open). Decompression gastrostomy tubes provide patients the ability to drain the stomach as for nausea and to avoid vomiting.
Syndromes
- Can the person answer questions correctly?
- Kidney disease (basic metabolic panel, urinalysis, or ultrasound of the kidneys)
- Choose whole fruits more often than juices. They have more fiber. Citrus fruits, such as oranges, grapefruits, and tangerines, are best. Opt for fruit juices without added sweeteners or syrups.
- Sudden high fever
- Problems aligning the teeth
- Sinus infection (sinusitis)
- Surgical biopsy to confirm diagnosis
Buy terbinafine 250 mg with amex
Talc has been shown to be the most effective pleurodesis agent in randomized clinical trials with reported success rates of 60% to 90% [30] fungus gnats essential oil buy terbinafine 250 mg with mastercard. However fungus under toenail buy terbinafine 250 mg line, although these procedures can be done at the bedside antifungal ear drops for dogs order genuine terbinafine on line, they do require the placement of a larger bore chest tube and can be rather painful [31]. Unlike patients with a bowel obstruction, patients with a perforated viscus are more likely to have pain from peritonitis, adding another element of consideration to both the decision-making process and the emotional charge of the situation. Currently, there is a small, but growing body of literature supporting the use of nonsurgical management for bowel perforation in select (hemodynamically stable, non-peritonitic) patients. Some studies have reported a greater than 90% success rate in nonsurgical management of patients with perforated diverticulitis [32]. Unfortunately, for patients with advanced cancer, who are not stable or who have peritonitis, and who undergo emergent surgery, the outcomes are even worse than for those with a bowel obstruction. Independent preoperative predictors of death at 30 days included renal failure, septic shock, ascites, dyspnea at rest, and dependent functional status. Postoperative respiratory complications and advanced age (greater than 75 years) were also predictors of mortality. Similar to the patients who presented with a bowel obstruction, only 4% had a “do not resuscitate” order in place prior to surgery despite the advanced nature of their cancer. Again, while data from studies like this may help surgeons answer questions about the risks associated with surgical interventions and guide some patients in their decisions, in a society in which people are not prepared for dying, these data can often make things harder for the surgeon who is asked to operate in the face of such overwhelming odds. Professionalism demands that the surgeon make a sincere effort to understand and be understanding of the perspective of the patient and family—without realistic expectation of the same in return. This can be particularly challenging when the surgeon is busy or when these events occur in the middle of the night. In the name of “full disclosure and informed consent,” some surgeons paint as bleak a picture as possible for the patient and family, in an effort to dissuade the patient from choosing surgery. When, despite these efforts, the patient and family ask for surgery, some surgeons expect a tacit agreement that the patient will endure to the end, including any additional procedures or maneuvers that may be required—surgery, feeding tubes, tracheotomy, dialysis, rehabilitation, etc. There is often a sense of frustration and betrayal on the part of the surgeon when within a few days after the index surgery, the family decides to stop any further life-prolonging care. It is for this reason that understanding the perspective of the patient and family is critical to both outcome of the encounter and the surgeon’s well- being (see Chapter 36). As described above, use of the palliative triangle can help create a space in which all three parties are given a chance to express their concerns and be heard. It is also significant in that it helps the surgeon separate the patient’s goals and understanding from that of the family’s and vice versa. If the surgeon truly hopes to influence the behavior of the patient and the family in an efficient and professional manner, an outward mind-set, in which the patient’s and family’s objectives matter like the surgeon’s objectives matter, is essential. The Arbinger Influence Pyramid is a proven leadership approach to influencing behavior which is readily applicable to patient–family–physician interactions [33]. Starting at the base of the pyramid, the surgeon must adjust his or her mind-set to an outward mind-set in which the goals and objectives of the patient and family matter equally with his or hers. The outward mind-set will then facilitate building a relationship with the patient and those who have influence on the patient—namely the family. Building this relationship can happen simply through introductions and a sincere expression of empathy for the challenging situation which the patient and family are facing. Next, the surgeon needs to listen and learn what the patient and family know about the situation and what their hopes, goals, and objectives are. Afterward, the surgeon can teach the patient and family what they need to know, correct any misconceptions, answer questions, review the risks, benefits, and indications for surgery and the alternative options, and make an engaged recommendation based upon the goals of all three parties. From there, the surgeon, patient, and family can usually come to a mutually agreed upon goal and care plan (see “structured family meetings” in Chapter 34). First, time and effort spent at the lower levels of the pyramid is what ensures effectiveness at the higher levels. Second, the solution to a problem at one level of the pyramid will be found in spending more time at a lower level of the pyramid.
Purchase terbinafine cheap online
The Minnesota tube was described in 1968 as a modification of the Sengstaken–Blakemore tube antifungal wiki quality terbinafine 250 mg, incorporating the esophageal suction port fungus yeast mold generic terbinafine 250 mg with amex, which is described later fungus gnats bananas 250 mg terbinafine order amex. Several studies have published combined experience with tubes such as the Linton–Nachlas tube; however, the techniques described here are limited to the use of the Minnesota and Sengstaken–Blakemore tubes. Self-expanding metal stents as an alternative to balloon tamponade are promising and currently under investigation [4,5]. Emergent therapeutic endoscopy in conjunction with pharmacotherapy is more effective than pharmacotherapy alone and is also performed as soon as possible. Band ligation has a lower rate of rebleeding and complications when compared with sclerotherapy, and should be performed preferentially, provided that visualization is adequate to ligate or sclerose varices successfully [3,10]. Tissue adhesives such as polidocanol and cyanoacrylate delivered through an endoscope are being used and studied outside the United States though glue embolization remains a concern [5]. Balloon tamponade is performed to control massive variceal hemorrhage, with the hope that band ligation or sclerotherapy and secondary prophylaxis will then be possible. Other alternatives include percutaneous transhepatic embolization; emergent esophageal transection with stapling [13]; esophagogastric devascularization with esophageal transection and splenectomy; and hepatic transplantation. If at all possible, making an adequate anatomic diagnosis is critical before any of these balloon tubes are inserted. Severe upper gastrointestinal bleeding attributed to esophageal varices in patients with clinical evidence of chronic liver disease results from other causes in up to 40% of cases. The observation of a white nipple sign (platelet plug) during endoscopy is indicative of a recent variceal bleed. A balloon tube is contraindicated for patients with recent esophageal surgery or esophageal stricture [17]. Some authors do not recommend balloon tamponade when a hiatal hernia is present, but there are reports of successful hemorrhage control in some of these patients [18]. When there are no other options, it may be practical to titrate to the lowest effective balloon pressures especially when repeated endoscopic sclerotherapy has been performed, because there is increased risk of esophageal perforation [19]. The incidence of aspiration pneumonia is directly related to the presence of impaired mental status [20]. Suctioning of pulmonary secretions and blood that accumulates in the hypopharynx is facilitated in patients who have been intubated. Sedatives and analgesics are more readily administered to intubated patients, and may be required when balloon tamponade is poorly tolerated, because retching or vomiting may lead to esophageal rupture [21]. The incidence of pulmonary complications is significantly lower when endotracheal intubation is routinely used [22]. Hypovolemia, Shock, and Coagulopathy Adequate intravenous access should be obtained with large-bore venous catheters for blood product administration and fluid resuscitation with crystalloids and colloids. Packed red blood cells should be administered keeping four to six units available in case of severe recurrent bleeding, which commonly occurs among these patients. Clots and Gastric Decompression If time permits, placement of an Ewald tube and aggressive lavage and suctioning of the stomach and duodenum facilitates endoscopy, diminishes the risk of aspiration, and may help control hemorrhage from causes other than esophageal varices. Infection, Ulceration, and Encephalopathy Mortality is increased when infection is present in bleeding cirrhotic patients. Intravenous proton pump inhibitors are more efficacious than histamine-2-receptor antagonists for maintaining gastric pH at a goal of 7 or greater. Rifaximin, lactulose, or lacitol may be useful, because blood and ammonia-forming bacteria in the gastrointestinal tract may contribute to encephalopathy. Balloons, Ports, and Preparation All lumens should be flushed to assure patency and the balloons inflated underwater to check for leaks. Two clean 100-mL (or larger) Foley-tip syringes and two to four rubber-shod hemostats should be readied for inflation of the balloons. To ensure that the gastric balloon will not be positioned in the esophagus, preinsertion compliance should be tested by placing 100-mL aliquots of air up to the listed maximum recommended volumes into the gastric inflation port while recording the corresponding pressures using a manometer attached to the gastric pressure port. A portable handheld manometer allows for simpler continuous monitoring as well as patient transport and repositioning. When possible, a second manometer should be attached to the esophageal pressure port to facilitate inflation and continuous monitoring. Place a plug or hemostat on the other arm of the esophageal inflation port instead of a 100-mL syringe, because the manometer may also be used for inflation, rendering the syringe superfluous [26,27]. Both balloons are then completely deflated using suction and clamped with rubber hemostats or plugged before lubrication.
Order terbinafine with a mastercard
How- ever antifungal body lotion purchase terbinafine 250 mg with mastercard, the diaphragm and the cervical cap were not invented until the late 1800s fungus stop zane hellas purchase 250 mg terbinafine visa, the same time period that saw the beginning of investigations with spermicidal agents fungi phylum order terbinafine 250 mg visa. The Japanese used balls of bamboo paper, Islamic women used willow leaves, and the women in the Pacifc Islands used seaweed. Ref- erences can be found throughout ancient writings to sticky plugs, made of gumlike substances, to be placed in the vagina prior to intercourse. In pre- literate societies, an efective method had to have been the result of trial and error, with some good luck thrown in. The social and technical circumstances of ancient times conspired to make communication of information very difcult. Hence, the widespread use of potions, body movements, and amulets; all of which can be best described as magic. The descriptions of contraceptive techniques by Soranus are viewed as the best in history until modern times. Soranus gave explicit directions regarding how to make concoctions that probably combined a barrier with spermicidal action. He favored making pulps from nuts and fruits (probably very acidic and spermicidal) and advo- cated the use of sof wool placed at the cervical os. In 1564, Gabriello Fallopius, one of the early authori- ties on syphilis, described a linen condom that covered the glans penis. The linen condom of Fallopius was followed by full covering with animal skins and intestines, but use for contraception cannot be dated to earlier than the 1700s. Vulcanization of rubber dates to 1844, and, by 1850, rubber con- doms were available in the United States. The introduction of liquid latex and automatic machinery ultimately made reliable condoms both plentiful and afordable. Some blame the more prudish attitude toward sexuality as an explanation for why American women had difculty learning self-insertion techniques. By the 1950s, more than 90 diferent spermicidal products were being marketed, and some of them were used in the frst eforts to control fertility in India. In the last decades of the 1800s, condoms, diaphragms, pessaries, and douching syringes were widely advertised; however, they were not widely Barrier Methods of Contraception used. It is only since 1900 that the knowledge and application of contra- ception have been democratized, encouraged, and promoted. And it is only since 1960 that contraception teaching and practice became part of the pro- gram in academic medicine, but not without difculty. In the 1960s, Duncan Reid, chair of obstetrics at Harvard Medical School, organized and cared for women in a clandestine clinic for contraception. Reid’s Clinic” at the Boston Lying-In Hospital, women were able to receive contraceptives not available elsewhere in the city. Lee Buxton, chair of obstetrics and gynecology at Yale Medi- cal School, and Estelle Griswold, the 61-year-old executive director of Con- necticut Planned Parenthood, opened four Planned Parenthood clinics in New Haven, in a defant move against the current Connecticut law. In an obvious test of the Connecticut law, Buxton and Griswold were arrested at the Orange Street clinic, in a prearranged scenario scripted by Buxton and Griswold at the invitation of the district attorney. Tey were found guilty and fned $100, but imprisonment was deferred because the obvious goal was a decision by the United States Supreme Court. On June 7, 1965, the Supreme Court voted 7–2 to overturn the Connecticut law on the basis of a constitutional right of privacy. It was not until 1972 and 1973 that the last state laws prohibiting the distribution of contraceptives were overthrown. A Clinical Guide for Contraception Failure Rates During the First Year of Use, United States3–5 Percent of Women with Pregnancy Method Lowest Expected Typical No method 85 85 Combination pill 0. Women who have never used barrier methods of contraception are almost twice as likely to develop cancer of the cervix. Barrier Methods and Preeclampsia An initial case-control study indicated that methods of contraception that prevented exposure to sperm were associated with an increased risk of preeclampsia.
Discount terbinafine 250 mg buy line
The diagnosis is made on the clinical Benign Diseases of the Vulva 807 features dimorphic fungi definition order terbinafine on line amex, with a score of 4 or more points when a patient tumour fungus bob 250 mg terbinafine buy visa. The eruption is erosive and can migrate with a has recurrent oral ulceration (2 points) antifungal hair loss generic terbinafine 250 mg line, recurrent genital spreading serpiginous edge. The perineum is most severely ulceration (2 points), ocular lesions (2 points), cutaneous affected but perioral lesions may also be seen. Glossitis and lesions (erythema nodosum, folliculitis, pyodermatous diabetes are usually associated. The diagnosis is made by plaques, all scoring 1 point), vasculitis (1 point) and a finding a raised glucagon level. The rash often responds positive pathergy test (where pustulation occurs at the well to surgical removal of the primary tumour. The Acrodermatitis enteropathica oral ulcers are similar to common aphthae but the vulval ulcers are usually larger, more painful and tend to heal This is related to zinc deficiency and may be inherited as with scarring. The labia minora are most commonly an autosomal recessive condition or acquired secondary affected. The histology is rather non‐specific to parenteral nutrition, malabsorption, severe eating dis but thrombosed arterioles may be seen. The erythematous and pustular the management of these patients should be multi lesions affect the genitalia and also the perioral skin. Diagnosis is made on a low zinc level and treatment is Neurological and ophthalmological complications can with oral supplementation. Several drugs are used including steroids, colchicines, dapsone and thalid omide. The pigmentation of the vulval skin can vary widely with ethnicity and hormonal status. Dark areas can result from Necrolytic migratory erythema (glucagonoma deposition of haemosiderin or melanin. Haemosiderin syndrome) pigmentation tends to be red/brown and occurs after an This is a rare syndrome, of unknown cause, where cutane inflammatory dermatosis such as lichen planus. Melanin ous changes are seen secondary to a pancreatic islet cell pigmentation is usually darker brown or black and any new pigmented areas where the diagnosis is not clini cally obvious must be biopsied. Hyperpigmentation the most common cause of pigmented patches on the vul val skin is post‐inflammatory hyperpigmentation. It most frequently occurs after lichen planus but can be seen after other inflammatory dermatoses and fixed drug eruptions. Vulval melanosis Areas of pigmentation may be seen without any preced ing history of inflammation. These can be very irregular and must always be biopsied to confirm their benign nature. Histology shows an increased num ber of melanocytes and some pigmentary incontinence. Similar lesions may be found in the oral cavity and there is no evidence that they become malignant at either site. Acanthosis nigricans Velvety, thickened and hyperpigmented plaques are seen symmetrically spreading form the labia majora to the inguinal folds and may extend perianally. No treatment is gener Hypopigmentation ally required but cryotherapy or curettage and cautery are effective if they become troublesome. It resolves lial neoplasia, the lesions should be biopsied to exclude spontaneously after the inflammation is treated. Vitiligo Melanocytic naevi This is a common autoimmune disorder where complete Vulval naevi are not common. It is patchy but sym tures and are regarded as atypical genital naevi [19] rather metrical and peri‐oroficial sites including the genitalia than variants of ‘dysplastic’ naevi. The main differential diagnosis is gist may report a malignant melanoma as there is cyto lichen sclerosus and indeed the two diseases may coexist. Naevi seen with lichen sclerosus can tural change and the texture of the skin is normal also mimic malignant melanoma clinically and histologi. There is no effective treatment, and ultravio cally but there are case reports of true malignant mela let phototherapy that is occasionally helpful at other sites noma developing in association with lichen sclerosus. No treatment is needed but if they enlarge Vascular lesions and become painful, they can be removed by cryother apy or cautery.
Bengerd, 54 years: Fever is the most common symptom and may be associated with other signs of prosthetic valve dysfunction including congestive heart failure, a new murmur, or embolic phenomena. A catheter is placed into the urinary bladder and a nasogastric tube is inserted into the stomach to prevent iatrogenic bladder or gastric injury.
Riordian, 35 years: Mumbai: objective ‘to eliminate sickness and death caused by vaccine Indian Academy of Pediatrics; 2011. Retinal Necroses Retinal necrosis is a medical emergency necessitating treatment within hours.
Fedor, 64 years: General measures management Hepatitis A virus and Hepatitis E virus infection can be prevented by improving the environmental hygiene. Korb S, Albornoz G, Brems W, et al: Verapamil pretreatment of hemodynamically unstable donors prevents delayed graft function post-transplant.
Vak, 30 years: The adrenal cortex has three zones, and each zone synthesizes a different type of steroid hormone from cholesterol (ure 26. Steroid hormones are contrain- dicated in patients with hepatitis until liver function tests return to normal.
Domenik, 53 years: It is best to have all the necessary equip spread in cases of undiagnosed leiomyosarcoma during ment together on a surgical cart, with the monitor at a Ambulatory Gynaecology, Hysteroscopy and Laparoscopy 527 comfortable height and position for the operator (and Diagnostic hysteroscopy patient if she is awake). Select the repetition rate based on the size and contour of the treatment area (see Selecting Initial Laser Parameters for Treatment section).
Gelford, 40 years: Dysfibrinogenemia Dysfibrinogenemia is a rare inherited thrombophilic state caused by mutations in the Aα, Bβ, or γ fibrinogen genes. Lactic acidosis is a metabolic acidosis and is defined as a blood lactate concentration above 5 mmol/L, while values between the upper limit of normal and 5.
Porgan, 58 years: It is recommended that all patients undergo coronary angiography or magnetic resonance imaging before surgical intervention. Dopamine is the major route for inhibition of prolactin secretion and hence the mechanism of action of some of these drugs.
Javier, 34 years: Liver biopsy typically reveals doughnut-like granulomas consisting of a lipid vacuole surrounded by a fibrinoid ring. If the patient is experiencing significant or life-threatening bleeding, reversal of anticoagulation is indicated and accomplished by replenishing the vitamin K-dependent factors.
Sinikar, 43 years: Antiviral therapy is not indicated in neutropenic patients unless a specific viral infection is documented. Food may be contaminated with lead when it is harvested, transported, processed, packaged, and prepared.
Avogadro, 50 years: A patient may donate autologous plasma for processing into cryoprecipitate prior to a planned surgical procedure. Endoscopic findings that implicate esophageal or gastric varices as the bleeding source include the red sign, where one varix is brighter red than the others from microtelangiectasia (red-sign variants include red- wale marks, cherry-red spots, hematocystic spots, and diffuse redness of varix), and the white-nipple sign, in which a fresh fibrin clot may be seen protruding from a varix [66,67].
Lares, 31 years: Source control is defined as “all physical measures undertaken to eliminate a source of infection, control ongoing contamination, and restore premorbid anatomy and function” [36]. Chagasic megacolon is another manifestation of chronic disease causing constipation and bowel obstruction that can lead to perforation and bacterial sepsis.
Tom, 27 years: These systems describe events with a multidimensional taxonomy to facilitate the comprehensive description and full deconstruction of errors to determine their root causes [9]. Bakker J, Coffernils M, Leon M, et al: Blood lactate levels are superior to oxygen-derived variables in predicting outcome in human septic shock.
Malir, 49 years: A maximal expiratory pressure of less than 40 cm H O is generally associated with a poor cough and2 difficulty clearing secretions [19]. Many movement disorders represent progressive, multisystem neurodegenerative processes that can result in increased disability over time.
Marlo, 63 years: Given the severity of the inciting disorder, mortality is high in acute cortical necrosis, with fewer than 20% of patients surviving. As newer devices become available, the management of patients with multiple muscular ventricular septal defects may evolve toward primary repair using hybrid surgical-catheter techniques and away from preliminary pulmonary artery banding.
Frithjof, 26 years: For this reason, platelet transfusion has been advocated with replacement of every blood volume to avoid the effect of dilutional thrombocytopenia [51]. The mechanism is unclear, but because of a longer onset, these agents are usually given at the start of surgery.
Rathgar, 61 years: Excess Retained Chordal Button Tissue Excess retained chordal and leaflet tissue above the mitral annular plane should be sutured to the atrial wall away from the sewing ring to prevent interference with the prosthetic mechanism. Atropine is indicated primarily for bradycardias causing hemodynamic difficulty or associated with ventricular arrhythmias.
9 of 10 - Review by C. Derek
Votes: 153 votes
Total customer reviews: 153
References
- Onen A, Kaya M, Cigdem MK, et al: Blunt renal trauma in children with previously undiagnosed pre-existing renal lesions and guidelines for effective initial management of kidney injury, BJU Int 89(9):936n941, 2002.
- Bobrow BJ, Spaite DW, Berg RA, et al. Chest compression-only CPR by lay rescuers and survival from out-of-hospital cardiac arrest. JAMA. 2010;304:1447-1454.
- Li YL, Wong DT, Wei W, et al. A novel acoustic window for trans-oesophageal echocardiography by using a salinefilled endotracheal balloon. Br J Anaesth 2006; 97:624-629.
- Kaplan SA, Roehrborn CG, Gong J, et al: Add-on fesoterodine for residual storage symptoms suggestive of overactive bladder in men receiving-blocker treatment for lower urinary tract symptoms, BJU Int 109(12):1831n1840, 2012.
- Katz ES, Tunick PA, Rusinek H, et al: Protruding aortic atheromas predict stroke in elderly patients undergoing cardiopulmonary bypass: Experience with intraoperative transesophageal echocardiography, J Am Coll Cardiol 20:70-77, 1992.
- Numano F: Takayasu's arteritis: clinical aspects. In Hoffman GS, Weyand CM, editors: Inflammatory diseases of blood vessels, New York, 2002, Marcel Dekker, p 455.
- Smith JS, Frankenfield DC, Souba WW: Nutrition and metabolism. In Mulholland MW, editor: Greenfield textbook of surgery, ed 4.