Dawn Sollee, PharmD
- Assistant Director
- Florida/USVI Poison Information Center-Jacksonville
- Associate Professor
- Department of Emergency Medicine
- College of Medicine
- University of Florida
- Jacksonville, Florida
Hyzaar dosages: 50 mg, 12.5 mg
Hyzaar packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
50 mg hyzaar otc
Management in either situation includes close serial assessment of the fetal heart rate and observation for the development of heart failure arrhythmia quizzes order hyzaar online pills. In one study from two tertiary referral centers blood pressure 9060 order hyzaar 12.5 mg without a prescription, only 9 of 16 such pregnancies intended to carry to term resulted in live births blood pressure medication start with l order hyzaar australia, and only 3 were still alive at 1 year of age (314). The presence of maternal hypothyroidism or vitamin D deficiency further increases the risk (318). Concern for myocardial involvement may justify additional fetal echocardiographic assessment in the third trimester even if the rhythm has remained sinus throughout gestation (29). Untreated, fetal mortality ranges from 9% to 34%, with risk of death increased in those diagnosed before 20 weeks, or with a ventricular rate <50 bpm, fetal hydrops, or impaired left ventricular function at diagnosis (322,323,324). Treatment may also be considered in fetuses manifesting with complete block to prevent dilated cardiomyopathy (29,322,324). Tachycardia Fetuses with any tachyarrhythmia of >180 bpm should undergo a complete fetal echocardiographic evaluation and consultation (29,307). Delivery may be considered in fetuses close to term with sustained tachycardia or evidence of compromise, weighing the risk of prematurity versus risks of maternal therapy. Fetuses with sustained tachycardia (>50% of time monitored) who are not near-term, or fetuses with intermittent tachycardia but evidence of ventricular dysfunction or hydrops should be treated pharmacologically transplacentally (29). Rather, treatment is aimed at sufficient arrhythmia control such that ventricular dysfunction or other evidence of significant compromise improves and resolves. Hydropic fetuses incur a greater mortality and medical management is more difficult with reduced efficacy of transplacental drug transfer (338,339). A summary of the medications most commonly used in the management of fetal arrhythmias are outlined in Table 5. It is estimated that 50% to two-thirds of neonates will require antiarrhythmia therapy (301,340). Genetic disorders are thought to be even more prevalent in the fetal population than in the newborn population, given the potential of fetal death. This can be performed by chorionic villus sampling or amniocentesis at appropriate gestational ages, or most recently maternal serum testing (341). However, while maternal serum testing has high sensitivity and specificity for Trisomy 21, sensitivity is poorer for Trisomy 13 and 18, and specificity is low for sex chromosome abnormalities (342). Fetal Cardiac Intervention Fetal cardiac intervention is attractive given the potential to halt the progression of cardiovascular disease while still in the protective maternal environment (202). Fetal cardiac interventions were described as early as 1975, when maternal propranolol administration was used to treat fetal tachycardia (343). Current fetal cardiac interventions can generally be divided into three categories: (1) pharmacologic, (2) ultrasound-based, and (3) invasive. Diagnosis and treatment of fetal cardiac disease: A scientific statement from the American Heart Association. Diagnosis and treatment of fetal cardiac disease: A scientific statement from the American Heart Association. Pharmacologic Transplacental pharmacologic therapy for fetal arrhythmia has been utilized for decades, and is discussed in more detail in the fetal arrhythmia of this chapter. This is typically administered by oral or intravenous routes to the mother, although direct amnioinfusion has been described. Less-described therapies that are still being investigated include administration of digoxin for fetal heart failure, indomethacin to achieve restriction or closure of the ductus arteriosus in the setting of Ebstein anomaly or dysplastic tricuspid valve, and administration of oxygen to mothers for fetuses with left heart hypoplasia (138,226,238,345,346). The tenet of maternal hyperoxygenation is that increased maternal oxygen delivery results in a fall in fetal pulmonary vascular resistance and in turn, pulmonary venous return flow to the fetal left heart (116,124). Chronic maternal hyperoxygenation has also been described as a therapy for fetal left heart hypoplasia (345). Invasive Procedures Apart from pharmacologic intervention, the most frequent fetal cardiac interventions currently performed are catheter-based. While “open” fetal cardiac surgery has been described in isolated reports, the utility and efficacy of this approach are not clear (202,344). While fetal aortic valvuloplasty was initially performed in only a few centers, it is now performed throughout the world, although with significant variation in volume between centers (354,355). Fetal death after aortic valvuloplasty is reported to occur in 11% to 20% (349,350,355). While reports suggest that fetal aortic valvuloplasty significantly improves the likelihood of ultimately having a biventricular repair, patients still nearly universally require addition postnatal interventions, and no clear survival benefit has been demonstrated to date from this procedure (349,354,355).
50 mg hyzaar order free shipping
From external inspection of the heart arrhythmia band order 50 mg hyzaar fast delivery, there may be obvious clues that there are significant abnormalities of the coronary artery circulation hypertension medical definition purchase 50 mg hyzaar with mastercard. The coronary arteries may be obviously thickened and nodular blood pressure chart youth buy hyzaar with mastercard, and rarely the coronary arteries may be seen connecting with the pulmonary trunk. Severe abnormalities may be readily apparent with epicardial aneurysmal dilation (Fig. So-called dimples may be observed on the epicardial surface of the heart, usually, but not exclusively, in association with the subepicardial coronary arteries. Such dimples may be considered the external stigmata of ventriculocoronary connections and may indicate the site of such connections. In patients with a well-formed infundibulum the imperforate pulmonary valve exhibits three semilunar cusps with complete fusion of the commissures (Fig. The pulmonary valve is primitive in patients with a diminutive right ventricle and a severely narrowed or atretic infundibulum. Great Veins, Atrial Septum, Coronary Sinus, and Venous Valves A peculiar relationship exists between persistent right venous valve, ventriculocoronary connections, and pulmonary atresia with intact ventricular septum. It would be too simplistic, indeed incorrect, to speculate that a persistent venous valve is causal to right heart hypoplasia. Stenosis and atresia of the coronary sinus ostium have been observed, with decompression through an unroofed coronary sinus–left atrium fenestration. C: Nearly normal tricuspid valve in a patient with a normal-sized right ventricle. D: Severely dysplastic tricuspid valve in a newborn with large right ventricle and severe tricuspid regurgitation; the right ventricle is very thinned. E: Profound Ebstein anomaly of the tricuspid valve in a newborn with large right ventricle and severe tricuspid regurgitation. Because of the obligatory right-to-left shunt at atrial level, with rare exception, there is either a patent foramen ovale or true secundum atrial septal defect. Premature closure of the foramen has been observed in this disorder, usually with fetal death. Rarely, if the interatrial septum is intact or nearly so, alternative pathways for systemic venous return have been recognized, including coronary sinus–left atrial fenestration. The septum primum may assume aneurysmal proportions in patients with a restrictive atrial septal defect, and its herniation through or obstruction of the left ventricular inflow has been observed. Tricuspid Valve The tricuspid valve is rarely normal in patients with pulmonary atresia and intact ventricular septum. This atrioventricular valve demonstrates the continuum of abnormalities and a functional impact that ranges from extreme stenosis to profound regurgitation (21) (Fig. The stenotic valve can demonstrate a hypoplastic obstructive annulus that may be muscularized with a very abnormal valve apparatus consisting of a thickened free valve margin, shortened dysplastic chordae, and papillary muscle abnormalities. In this situation, the valve exhibits both profound displacement with the severest form of Ebstein anomaly and dysplasia. In some severely regurgitant valves, the valve is not displaced, but it is extremely dysplastic. Rarely, the valvar orifice may be virtually unguarded, a situation similar to profound Ebstein anomaly (22). The most severely stenotic and obstructive tricuspid valve is observed in patients with the most hypoplastic of right ventricles. Conversely, patients with a large right ventricle usually have severe tricuspid regurgitation with a valve exhibiting features of Ebstein anomaly and dysplasia. This latter malformation represents a major management challenge with a poor overall prognosis. Right Ventricle Clinicians and pathologists have attempted to characterize the size of the right ventricle in this disorder for decades. Methodologies have included angiocardiographic volumetric analysis, a variety of measurements of the inlet/outlet axis and the convention advocated P. This reflects the deviation of the valvar diameter from that expected for body surface area and was based on an early pathologic study of the normal quantitative anatomy. Although there is no consensus as to whether the morphologically right ventricle is embryologically a bipartite or tripartite structure, there are examples of congenitally malformed hearts that may support the view of the right ventricle as a tripartite structure. Taking this latter approach, the normal right ventricle can be considered to be composed of confluent inlet, apical trabecular, and outlet components.
Syndromes
- Amputation if the disease spreads through an arm or leg
- Breathing difficulty
- Infection
- Urinary tract infection
- Infection
- Rapid heart rate
Hyzaar 50 mg low cost
A ship carrying this type of cargo should declare its inventory to the city fre department hypertension follow up hyzaar 50 mg mastercard, type and amount blood pressure chart 5 year old 50 mg hyzaar order visa. Furthermore blood pressure medication voltaren 50 mg hyzaar for sale, ships carry- ing this type of cargo should be berthed in an isolated area of the har- bor so that if something does go wrong, it will not impact other ships or infrastructure. The fre department should mobilize all of its resources immediately to combat the blaze. The city manager should stay in close contact with the fre department and alert hospitals that a crisis is currently unfolding. In addition, the city manager should seek out assistance from sur- rounding municipalities and state ofcials. If possible, the ship needs to be moved well away from any infrastructure and other ships. If the ship cannot be moved, then other ships that are in the vicinity need to be moved away from the area. Additionally, there is no telephone service since the telephone operators are on strike and there is no one to perform their function. You have dis- patched the city’s two fre trucks and the volunteer frefghters have arrived on the scene with an additional two fre trucks, but the fre cannot be contained with just water (Moore Memorial Public Library, 2007). The city manager needs to make sure that the area is cleared of workers and citizens to avoid casualties. If possible, an airplane equipped with fre-retardant chemicals needs to be obtained to help fght the blaze. Since you have no electronic communica- tions through the telephone system, other means will need be made available, such as setting up runners or getting volunteers with short-wave radios to assist with communication eforts. Since you have no hazardous materials team, local ofcials and state ofcials need to be contacted to obtain critical resources that can be used to fght a chemical fre. You need to make a public plea for the telephone operators to come back to work and of strike so that your communication system will be operable. Stage 5 of the Disaster The ship’s crew had only been able to remove 3 of 16 boxes of small arms ammuni- tion. In an attempt to douse the blaze, the captain of the ship has had steam poured into the cargo hold. Unfortunately, the steam turned the ammonium nitrate into poisonous nitrous oxide gas vapors, which fll the ship. The area needs to be completely evacuated since the fre is out of control and there is no viable means to fght the fre at this point. All ships need to be cleared of the harbor and chemicals that are in the dock area need to be relocated if at all possible. Additional frst responders will be needed to seal of the area and ensure that all of the evacuations have taken place. Stage 6 of the Disaster The steam has super heated the ammonium nitrate and has caused the ship’s fuel and oil tanks to leak, which is feeding the fre. The city manager needs to make sure that his police department keeps bystanders away from the disaster site by sealing of roadways leading to the harbor. Unfortunately there is not much that the city manager can do at this point since the fre is out of control and the city lacks proper frefghting equipment to take care of the situation. You should evacuate all of your frefghters from the area to avoid any of them getting hurt or killed. The explosion causes fooding around the initial area and also fattens a plant and several buildings in the nearby vicinity. You learn that the fre chief and 27 fre- fghters were killed, which leaves you with a huge shortage of trained frst respond- ers. In addition, you have no operational hospital in your city (Moore Memorial Public Library, 2007). The city manager needs to contact nearby cities with hospitals to manage anyone who has been injured in the fre or the blast. Search and rescue teams need to be formed to look for survivors in the buildings that were destroyed. The city manager will need to set up a makeshift hospital with as many medical volunteers as possible to assist with the wounded until those patients can be taken to a proper medical facility. Stage 8 of the Disaster The explosion killed hundreds of bystanders, pedestrians, and workers, and obliter- ated several buildings. The telephone operators have gone back on the job in this time of crisis and have telephoned a number of nearby agencies and municipalities for assistance.
Hyzaar 12.5 mg order without prescription
Calcium content may be reduced due to a disorder of calcium metabolism blood pressure medication causing low blood pressure hyzaar 50 mg with amex, as in osteomalacia or hyperparathyroidism prehypertension pediatrics order 12.5 mg hyzaar mastercard, or to a reduc- tion in protein matrix hypertension over 55 purchase hyzaar 50 mg amex, as in osteoporosis. The radiological diagnosis of decreased bone density is often diffcult, espe- cially as the appearances of the bones are markedly affected by radiographic exposure factors. The main causes of generalized decrease in bone density are: • osteoporosis • osteomalacia • hyperparathyroidism • multiple myeloma, which may cause generalized loss of bone density, with or without focal bone destruction. Each of these conditions may have other radiological fea- tures that enable the diagnosis to be made, but when they Fig. There is a are lacking, as they frequently are in osteoporosis and periosteal reaction which is present bilaterally along the shafts of the radius and ulna and the metacarpals. In this case, it was osteomalacia, it becomes very diffcult to distinguish associated with a bronchial carcinoma. The remaining bone is normally min- eralized and appears normal histologically, but because the matrix is reduced in quantity there is necessarily a reduction in calcium content. Osteoporosis predisposes to fractures, particularly of the vertebral bodies and hips. Postmenopausal and senile osteoporosis are the common- est forms: up to 50% of women over 60 years of age have osteoporosis. A radiological diagnosis of osteoporosis is only made after other diseases have been excluded. Bone destruction, which could indicate metastatic carcinoma or myeloma, and evidence of hyperparathyroidism and osteomalacia should be sought, because these conditions can closely resemble osteoporosis. Although there is an overall decrease in bone density, the cortex stands out clearly, as if pencilled in. An important feature is collapse of the vertebral bodies, repre- senting compression fractures, which result in the vertebral bodies appearing wedged or biconcave. There is decreased bone density may be involved and the disc spaces often appear widened. Many of the trabeculae the partial collapse of several of the vertebral bodies and the are resorbed but those that remain stand out clearly. Disuse osteoporosis can be caused by localized pain or immobilization of a fracture (Fig. Besides a reduc- tion in density and thinning of the cortex, the bone may Screening for osteoporosis sometimes have a spotty appearance (Fig. Refex sympathetic dystrophy syndrome (Sudeck’s atrophy) Because osteoporosis is such a prevalent problem and, once is a disorder of the sympathetic nervous system, compris- established, is diffcult to treat, attempts have been made ing severe osteoporosis and oedema of the soft tissues to develop screening tests for the at-risk population in following a fracture. The remaining bones of the right foot show a marked reduction in bone density with well-defned cortex. Bone mineral density is expressed as Rickets and osteomalacia a T score, which is the number of standard deviations above or below the mean for a young, healthy adult popu- In these conditions there is poor mineralization of osteoid. Although If this occurs before epiphyseal closure, the condition is bone density can be accurately and reproducibly measured, known as rickets; in adults the condition is known as osteo- bone mineral density is a poor predictor of an individual’s malacia. The main causes for osteomalacia are given in Box fracture risk and it has not been possible to use bone den- 11. In rickets the changes are maximal where bone growth is occurring, so they are best seen at the knees, wrists and ankles. The zone of provisional calcifcation is defcient and the metaphyses are irregularly mineralized, widened and cupped (Fig. This results in an increased distance between the visible epiphysis and the calcifed portion of the metaphysis. In osteomalacia the characteristic features are loss of bone density, thinning of the trabeculae and cortex, and Looser’s (a) (b) zones (pseudofractures) (Fig. There is reduced bone density and bowing of the are thought to be insuffciency fractures. Many patients with primary hyperparathyroidism present with renal stones and only a small minority have radiological bone changes. Hyperparathyroidism The signs of hyperparathyroidism in the bones are: Excess parathyroid hormone secretion mobilizes calcium • A generalized loss of bone density, with loss of differentia- from the bones, resulting in a decrease in bone density. The trabecular pattern Hyperparathyroidism may be primary, from hyperplasia may have a fne lacework appearance.
50 mg hyzaar amex
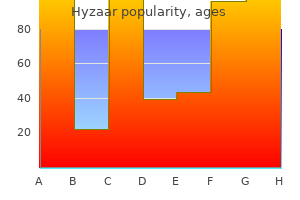
It is possible to estimate the right ventricular pressure in patients between 2 and 20 years of age if a pure R wave is present in lead V4R or V1 blood pressure medication vitamin k buy hyzaar american express. The height of the R wave in millimeters blood pressure varies greatly cheap hyzaar 12.5 mg without prescription, multiplied by 5 hypertension yahoo order hyzaar 12.5 mg with visa, approximates the right ventricular systolic pressure in millimeters of mercury (14). A superior axis, sometimes accompanied by a conduction abnormality of the left bundle, also has been described in some patients with pulmonary stenosis. There may be a correlation between these findings and Noonan syndrome, with its associated cardiomyopathy. This finding is present in 80% to 90% of cases, but it may be absent in infants, in patients with dysplastic pulmonary valve, and in cases of rubella syndrome. The right atrial segment may be prominent, more commonly in patients with associated P. The pulmonary vascularity is diminished as a result of right-to-left shunting at the atrial level. Heart size and pulmonary vascularity are usually normal in patients with mild to moderate stenosis. In the absence of right ventricular failure, even with severe obstruction, only mild cardio megaly is seen. When heart failure develops, marked cardiomegaly results due to right atrial and right ventricular enlargement, and pulmonary vascularity is decreased as a result of a reduction in pulmonary flow. Cardiomegaly is commonly present in infants with severe or critical pulmonary stenosis, and pulmonary vascularity is severely reduced because of the large atrial right-to-left shunt (Fig. Two-Dimensional Echocardiography The 2-D echocardiogram clearly demonstrates the typical features of the stenotic pulmonary valve from the standard and high parasternal short-axis and long-axis views as well as the subcostal sagittal views (Fig. Systolic motion is restricted, with inward curving of the tips of the leaflets, known as doming. Associated features, such as poststenotic dilation of the main and branch pulmonary arteries, also are easily recognized. Evidence of dynamic subpulmonary stenosis should be sought, but the severity may be impossible to estimate in the presence of more than mild valvar stenosis. The diagnosis of dysplastic pulmonary valve usually can be ascertained by echocardiography (Video 39. The leaflets appear thickened and immobile, without the characteristic doming seen in typical cases. The pulmonary valve annulus is hypoplastic, and supraannular narrowing of the proximal main pulmonary artery is often present. Doppler Evaluation The Doppler echocardiogram allows quantitative assessment of severity of pulmonary valve stenosis by estimating the pressure P. The simplified Bernoulli equation P = 4 V2 is used, where P is the peak instantaneous pressure gradient (mm Hg), across the obstructed pulmonary valve, and V2 is the peak flow velocity (m/s), distal to the obstructive orifice. If significant subpulmonary stenosis coexists, V1 (the peak flow velocity proximal to the obstruction) must be taken into account. The Doppler beam must be aligned parallel with the main pulmonary artery trunk or the direction of the flow jet as seen on color Doppler. Right ventricular pressure then can be estimated by adding the pressure gradient to the estimated right atrial pressure. Several studies have documented excellent correlation between the Doppler-derived gradient and that obtained by direct pressure measurement at catheterization (17,18). It should be recognized, however, that the Doppler- derived peak instantaneous pressure gradient exceeds the peak-to-peak pressure gradient measured at catheterization by a small amount. In pulmonary valve stenosis, this difference is clinically insignificant, and the two measurements are close enough to obviate the need for diagnostic catheterization in most patients until intervention becomes necessary. The development of color Doppler 2-D echocardiography has contributed to the diagnostic accuracy of pulmonary valve stenosis by demonstrating an abnormal flow pattern originating at the stenotic valve (see Fig. Normal flow is coded as red or blue, depending on whether it is directed toward or away from the transducer, respectively. High-velocity, turbulent flow through stenotic lesions appears as a mosaic jet with green, yellow, and other shades.
Hyzaar 50 mg order visa
Subclinical Cushing’s syndrome is characterized by lack of specific symptoms and signs of Cushing’s syndrome how is pulse pressure used as a diagnostic tool purchase hyzaar master card, but with evidence of autonomous glucocor- ticoid secretion blood pressure chart vs age generic hyzaar 12.5 mg amex. However blood pressure 40 over 70 50 mg hyzaar buy, majority of these patients have obesity, hyperten- sion, and type 2 diabetes. Causes of weight gain in a patient with Cushing’s syndrome are increased appetite, enhanced adipogenesis, fluid retention, and decreased physical activity. Increased appetite is because of stimulatory effect of cortisol on feeding center through aug- mented adenosine monophosphate kinase activity, insulin resistance, decreased corticotrophin-releasing hormone, and increased neuropeptide Y. Enhanced adipo- genesis is attributed to cortisol-mediated diversion of primitive mesenchymal stem cells to adipocytes and increased activity of lipoprotein lipase and glycerol- 3-phosphate dehydrogenase. Fluid retention also contributes to weight gain and is due to action of excess cortisol on mineralocorticoid receptor (specificity spill- over). Decreased physical activity resulting from proximal muscle weakness or neuropsychiatric manifestations is also a cause of weight gain. Nearly 45% of patients with Cushing’s syndrome have central obesity as against 55% with generalized obesity. However, children with Cushing’s syn- drome usually have generalized obesity, probably due to lesser omental fat. Weight gain is a hallmark feature of Cushing’s syndrome; however, some patients may present with weight loss. The causes include adrenocortical carci- noma, ectopic Cushing’s syndrome, uncontrolled diabetes, concurrent infec- tions like tuberculosis, and endogenous depression. Headache in patients with Cushing’s syndrome can be due to adenoma per se, sinusitis, cor- tical vein thrombosis, benign intracranial hypertension, and glaucoma. Striae are one of the classical features of Cushing’s syndrome and are present in 60–70% of patients. Striae in Cushing’s syndrome are violaceous-purple, dehis- cent, >1 cm wide and are commonly present over abdomen, thighs, buttocks, arms, and inframammary region. Wide and purplish striae are due to venular dila- tation and thinned out dermis, which in turn occurs as a result of loss of perivas- cular collagen support and dermal collagen breakdown, respectively. Striae may be absent in patients with childhood Cushing’s syndrome, adrenocortical carci- noma, ectopic Cushing’s syndrome, and hypercortisolemia associated with androgen excess. Causes of striae in the absence of Cushing’s syndrome include rapid weight gain during puberty, pregnancy, and pseudo-Cushing’s states. Cutaneous manifestations of Cushing’s syndrome are bruise, striae, plethora, cutic- ular atrophy (“cigarette paper” appearance – Liddle’s sign), and fungal infections. Bruise, striae, and plethora are due to loss of dermal collagen, while cuticular atro- phy is a result of atrophy of stratum corneum. Rarely, purpura can be associated with Cushing’s syndrome due to qualitative abnormalities in platelet function. Proximal myopathy in patients with Cushing’s syndrome is due to decreased muscle protein synthesis, increased muscle protein catabolism, and myocyte apoptosis. Concurrent hypokale- mia, hypophosphatemia, hypomagnesemia, vitamin D deficiency, and hypogo- nadism further contribute to muscle weakness in patients with Cushing’s syndrome. Why do some patients with Cushing ’ s syndrome lack features of protein catabolism? The features of protein catabolism, also called as specific features, are present in 60–70% of patients with Cushing’s syndrome. However, these features may not be present in patients with mild Cushing’s syndrome, cyclical Cushing’s syndrome, childhood Cushing’s syndrome, and hypercortisolemia associated with androgen excess. Patients with adrenocortical carcinoma and ectopic Cushing’s syndrome may lack features of protein catabolism due to short lag time between onset of hypercortisolemia and diagnosis. Plethora is considered as a specific sign of Cushing‘s syndrome and is due to dermal collagen breakdown and increased erythropoiesis because of hypercortisolemia. Hyperprolactinemia seen in 20–30% of patients may also contribute to increased adrenal androgen production. Further, patients with Cushing’s syndrome may also have increased fine hair (vellus hair), especially on the forehead, back, and extremities due to a direct effect of cortisol on pilosebaceous units. What are the causes of menstrual irregularities in patients with Cushing ’ s syndrome? Menstrual irregularities are seen in 70–80% of women with Cushing’s syn- drome; the most common being oligomenorrhea followed by secondary amenorrhea. Hypertension is seen in 75% of patients with endogenous Cushing’s syndrome as against 20% in exogenous Cushing’s syndrome.
Nalleru (Cissus Quadrangularis). Hyzaar.
- Obesity and weight loss, diabetes, metabolic syndrome, and high cholesterol, bone fractures, osteoporosis, scurvy, cancer, upset stomach, hemorrhoids, stomach ulcer, menstrual discomfort, asthma, malaria, pain, and body building.
- How does Cissus Quadrangularis work?
- Dosing considerations for Cissus Quadrangularis.
- Are there safety concerns?
- What is Cissus Quadrangularis?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97110
Generic 50 mg hyzaar visa
A shunt can also important in avoiding a low diastolic pressure in the early result in scarring and distortion of the pulmonary arteries blood pressure stroke cheap hyzaar express, postoperative period with a risk of acute cardiac arrest as and if performed through a thoracotomy is likely to cause well as longer-term excessive volume loading of the single distortion of the lobar branches blood pressure medication effect on running discount 50 mg hyzaar. For the average-sized neonate weighing between 3 488 Comprehensive Surgical Management of Congenital Heart Disease arteria sa generic hyzaar 12.5 mg buy line, Second Edition L. The proximal anastomosis is placed to a longitudinal arteriotomy in the origin of the right subcla- vian artery, which is controlled with a side-biting clamp. After construction of the proximal anastomosis the shunt is threaded posterior to the left innominate vein. This will also serve to lengthen the shunt which also to the left or right side so that at a subsequent procedure a helps to reduce the volume loading of the ventricle as origi- patch of anterior pericardium can be harvested if necessary. However, a child presenting at a weight of 5 dissected free being careful to avoid injury to the right recur- or 6 kg is likely to be several months old. If there is a suff- rent laryngeal nerve which can be seen passing around the cient degree of cyanosis that a systemic to pulmonary arterial distal right subclavian artery. A side-biting clamp is applied shunt has to be inserted then it is probable that the child has across the origin of the right subclavian artery and the distal suffciently low pulmonary resistance by that age, for exam- innominate artery. A longitudinal arteriotomy is made either ple beyond 2–3 months, that a more appropriate management partially or completely on the right subclavian artery depend- strategy would be to proceed directly to a bidirectional Glenn ing on the size of the child. A The child should be positioned supine with as much exten- direct anastomosis is fashioned. It is not dard median sternotomy incision is performed with the skin essential to administer heparin during the clamping period as incision extending at least to the top of the sternal notch. Even though it is possible to perform a strict policy regarding heparin administration and often Three-Stage Management of Single Ventricle 489 administer 1 mg/kg before clamp application if the neonate’s right atrial line to maintain a systolic pressure of at least coagulation appears normal. This will help to maintain shunt fow and reduce Following completion of the anastomosis the shunt is con- the risk of platelet deposition, particularly at the proximal trolled with a bulldog clamp that is applied close to the anas- anastomosis. A side-biting clamp is tionally smaller than expected, that is the oxygen saturation applied to the right pulmonary artery with appropriate rota- is less than 75% and there is little change in blood pressure tion of the vessel so that an incision can be made on the supe- or heart rate at clamp release. The anastomosis is fashioned once again with ing of the anastomoses and the shunt itself is often helpful. Upon release of the clamps there should If heparin was not administered before clamp application it be a decrease in diastolic pressure and an increase in arterial can be given now, usually in a dose of 1 mg/kg. A chest tube, both anastomoses have been done as well as possible and usually a 15 Fr soft silicone four-channel drain (e. The sternotomy incision is closed tiny incision is made in the middle of the shunt. A 3 mm Fogarty embolectomy catheter is passed Shunt Complications: Excessive Pulmonary Blood Flow proximally and infated and withdrawn. There should be an Opening the clamp on a systemic to pulmonary arterial shunt abrupt increase in fow out of the incision in the shunt and an results in an acute increase in volume work for the single increase in oxygen saturation. Balloon dilation of platelet ration is high following clamp release, for example greater or fbrin accumulation is usually helpful. Sometimes it is than 85% and if a metabolic acidosis begins to build up, con- necessary to place a small stent to optimize shunt function. Cardiac catheterization may also diagnose an unanticipated Often the simplest way to do this is to ligate the ductus rather problem such as discontinuity of the pulmonary arteries that than waiting for the duct to close following prostaglandin has been missed by the echocardiographers. Ligation of the duct also avoids competitive consequence of ductal closure that has occurred after with- fow which probably increases the risk of shunt thrombosis. However, if the duct is not ligated and if the shunt does sub- sequently thrombose, there is a possibility of resuscitating Surgery for Inadequate Pulmonary Blood the child through administration of prostaglandin. Although Flow Caused by Obstructed Total Anomalous there is no clear answer to this conundrum it is our usual Pulmonary Venous Connection practice to ligate the ductus when it is clearly large or if there is an additional source of pulmonary blood fow, for example Neonates with heterotaxy may present with a profound degree the child with forward pulmonary outfow through a stenotic of cyanosis because of obstructed total anomalous pulmo- pulmonary outfow. We have children also tend to have branch pulmonary artery stenoses used various techniques including hemoclips and Gore-Tex at the origin of either the right or left pulmonary artery or suture. Probably a good general principle to bear in mind is even discontinuity of the right and left pulmonary arteries. In that a gentle taper should be achieved rather than an abrupt order to optimize pulmonary artery development and to min- diameter change. There is no question that narrowing the imize pulmonary vascular resistance it is important that the shunt by any technique will introduce an increased risk of total anomalous pulmonary connection be repaired shortly acute shunt thrombosis at a later time.
Cheap hyzaar 12.5 mg free shipping
While Doppler gradients often provide accurate estimates of disease severity hypertension warning signs generic hyzaar 12.5 mg on-line, there are some instances in which Doppler findings may underestimate the degree of stenosis blood pressure average calculator purchase hyzaar 12.5 mg overnight delivery. Decreased cardiac output blood pressure standards 12.5 mg hyzaar mastercard, multiple levels of obstruction, or the presence of a “pop-off” (atrial or ventricular septal defect, patent ductus arteriosus, etc. Absent any of these scenarios, however, spectral Doppler can provide a highly accurate assessment of the severity of discrete left ventricular outflow tract obstruction. An apical long-axis view often provides optimal alignment for Doppler interrogation of the left ventricular outflow tract, while a high right parasternal view may also be useful in assessing the Doppler gradient (164). Doppler imaging will also provide accurate information on the presence and severity of aortic insufficiency. Doppler assessment of aortic valve stenosis, including valve area calculation using the continuity equation, is covered in detail in Chapter 13 and will not be discussed at length here. One key point to reiterate is the difference between the peak-to-peak gradients obtained by direct pressure measurement in the cardiac catheterization laboratory and the peak instantaneous pressure gradient obtained by spectral Doppler. As discussed in Chapter 13, these two measurements reflect different physiologic parameters, and the peak instantaneous gradient is generally P. While the mean Doppler-derived gradient may more closely approximate the peak-to-peak gradient than the peak instantaneous gradient does (167), the best estimate of the catheter-derived gradient is likely obtained by correcting the peak instantaneous gradient for the phenomenon of pressure recovery. Pressure recovery refers to an increase in fluid pressure that occurs after the immediate drop in pressure associated with passing through an area of discrete stenosis (168). Pressure recovery may be amplified in pediatric patients with small aortae, and a study of pediatric patients with simultaneous catheter and Doppler-based assessments of aortic valve gradients demonstrated that correcting peak instantaneous gradient for pressure recovery, using a previously validated formula, resulted in the best approximation of peak-to-peak gradient (169). The primary purpose in attempting to correlate Doppler estimates of gradient with peak-to-peak gradients obtained in the catheterization laboratory is to aid in clinical decision making, as the traditional indications for intervention have been based on catheter-derived numbers. In these guidelines, severe stenosis is defined by a peak velocity across the aortic valve of ≥4. In the setting of an artificially low gradient due to decreased cardiac output, an 2 2 2 aortic valve area ≤1. With time, noninvasive Doppler assessment of the degree of stenosis may increasingly replace catheter-based evaluation in clinical practice. Additional roles for echocardiography in the assessment of aortic stenosis include the evaluation of left ventricular systolic and diastolic function (discussed in detail in Chapter 13). The degree to which a left ventricle is able to accommodate increased afterload without undergoing pathologic remodeling is highly variable, and the sensitivity of echocardiography, particularly using newer strain-based assessments, in identifying subtle systolic and diastolic dysfunction is crucial in optimal clinical decision making (172,173,174). Given the high incidence of additional cardiac anomalies in patients with left ventricular outflow tract obstruction, a complete and careful anatomic survey is essential. In infants with critical aortic stenosis in whom a decision regarding a one versus two ventricle repair must be made, accurate measurements of all left heart structures, as well as detailed assessment of the mitral valve and its apparatus, is crucial. Three-dimensional transthoracic echocardiography may provide useful anatomic information when used in conjunction with standard two-dimensional echo and is particularly useful in delineating the mechanism of complex subaortic obstruction (163). Late gadolinium enhancement as a marker for fibrosis is an independent predictor of mortality in adults with aortic stenosis (176), although the same prognostic value has not yet been shown in children. The primary role for exercise testing in the contemporary evaluation of aortic stenosis is in the risk stratification of asymptomatic patients with severe disease. The same guidelines recommend avoiding exercise testing in any symptomatic patient. Patients who develop symptoms with exercise are considered symptomatic, despite the lack of symptoms at baseline, and aortic valve intervention is recommended. Cardiac Catheterization Although cardiac catheterization is still considered the gold standard to measure pressure gradients and determine the need for intervention, it has largely been replaced by echocardiography and other noninvasive imaging modalities as a diagnostic tool for aortic stenosis. More typically, cardiac catheterization is undertaken as a therapeutic tool for patients with valvar aortic stenosis (see “Therapeutic Cardiac Catheterization” below). That said, cardiac catheterization continues to have an important role in the diagnosis of aortic stenosis by providing hemodynamic assessment of disease severity and defining the anatomic substrate for obstruction. This can be especially useful when echocardiographic images are inadequate or result in conflicting data. When performing a cardiac catheterization for the diagnosis of aortic stenosis or assessment of disease severity, it is generally optimal to perform the procedure using light conscious sedation to mimic resting hemodynamic conditions as closely as possible. General anesthesia can alter systemic vascular resistance, which can impact measured pressure gradients.
Hyzaar 12.5 mg buy without prescription
In addition high blood pressure medication and zinc order hyzaar overnight delivery, children with normal age of onset of puberty cardiac arrhythmia 4279 hyzaar 12.5 mg purchase with visa, but without progression of pubertal events over a period of 2 years (arrested puberty) blood pressure medication cause erectile dysfunction hyzaar 50 mg purchase fast delivery, or those with signifcant delay in the progression of pubertal events (>5 years between thelarche and menarche in girls or >5 years between onset of testicular enlargement and complete genital development in boys) are also considered to have delayed puberty. The age of onset of puberty in a population is normally distributed (bell-shaped curve with a Gaussian distribution). In the studies by Tanner and Marshall, it was shown that the mean age of onset of puberty was 10. It has been shown that a critical body weight/body fat is essential for the onset of puberty. This is evidenced by the presence of delayed/absent puberty in girls with low body fat and early puberty in obese girls. The key role of leptin in the induction of puberty is evidenced by the occurrence of isolated hypogonadotropic hypogonadism in individuals with congenital leptin defciency and initiation of puberty in these individuals with recombinant leptin therapy. Despite these evidences, leptin is considered to have a permissive role, rather than a primary role as evidenced by timely onset of puberty in patients with congenital generalized lipodystrophy, who are def- cient in leptin. In boys, gonadotropins and testosterone peak at 3 months and decline by 6–9 months of age. Serum estradiol levels widely fuctuate during mini-puberty in girls, whereas serum testosterone is stable in boys. The wide fuctuation in serum estradiol during mini-puberty is possibly due to cyclical maturation of ovarian follicles (Fig. The postnatal surge of gonadotropins and testosterone leads to growth and prolifera- tion of Leydig cells, Sertoli cells, and germ cells, thereby resulting in increase in testicular volume (by approximately 1 ml) and penile size and also contribut- ing to postnatal testicular descent. Further, mini-puberty also helps in priming of pilosebaceous units and development of male psyche. Mini-puberty is absent in children with congenital hypogonadotropic hypogo- nadism and complete androgen insensitivity syndrome; however, it is present in children with partial androgen insensitivity syndrome. Negative feedback between most of the target glands and hypothalamic–pitu- itary axis is usually established by 2–3 years of age. Hypogonadism refers to a clinical syndrome characterized by impaired gonadal function resulting in decreased gonadal steroidogenesis and/or gametogenesis. However, in clinical practice, those with isolated germ cell dysfunction but with normal gonadal steroidogenesis are not considered as having hypogonadism. Similarly, a well-feminized female with normal circulating levels of estradiol, but with chronic anovulation (e. Disorders caused by abnormalities of hypothalamus and pituitary gland are termed as hypogonadotropic hypogonad- ism, whereas those with a primary defect at the level of gonads are termed as hypergonadotropic hypogonadism (primary gonadal failure). The prevalence of various causes of delayed puberty is summarized in the table given below. The causes of permanent hypo- gonadotropic hypogonadism include congenital isolated hypogonadotropic hypogonadism, congenital multiple pituitary hormone defciency, and tumors/ cysts in sellar–suprasellar region. Turner syndrome, Klinefelter syndrome, and post-chemotherapy/gonadal irradiation are the common causes of hypergonad- otropic hypogonadism (Fig. Any patient with adult-onset hypogonadotropic hypogonadism should be investi- gated for sellar–suprasellar pathology like tumor and infltrative disorders. In addition, functional hypogonadotropic hypogonadism can be associated with any chronic systemic illness. Approximately 30% of individuals with congenital isolated hypogonadotropic hypogonadism have identifed genetic mutation as a cause of hypogonadism, while the rest are idiopathic. How to suspect congenital isolated hypogonadotropic hypogonadism during early childhood? What are the clinical clues to differentiate between prepubertal and postpuber- tal onset of hypogonadism in an adult male? The presence of micropenis, cryptorchidism/small testicular volume (testicular volume <4 ml), scant pubic and axillary hair, eunuchoidal habitus (due to delayed epiphyseal closure), and high-pitched voice suggests the prepubertal onset of hypogonadism. Postpubertal onset of hypogonadism is suggested by the presence of normal body proportions, normal- or small-sized testes with soft consistency, regression of pubic and axillary hair, and reduced shaving frequency (Fig. Kallmann syndrome is characterized by the coexistence of anosmia/hyposmia in a patient with congenital isolated hypogonadotropic hypogonadism. These genes might be playing a minor role in the development and migration of olfactory neurons (Fig.
Cheap 50 mg hyzaar mastercard
Close followup is warranted blood pressure 3020 order generic hyzaar online, and annual echo may be helpful (109) but should be individualized to the patient blood pressure exercise program discount hyzaar 50 mg free shipping. Intense blood pressure medication nerve damage cheap hyzaar 50 mg overnight delivery, repetitive isometric activities may enhance aortic stiffness (110) and dilation (111); however, in the absence of aortic root dilation, isometric activities are currently acceptable (112). Exercise restrictions are implemented for regurgitant and/or stenotic aortic valves, and the degree of restriction is commensurate with the degree of the hemodynamic abnormality (112). Mild aortic dilation does not typically indicate exercise restrictions; however, frequent (annual) assessment is required in athletes, with attention to both the absolute dimension and rate of change. In younger preadolescent ages, the aortic root size should be indexed to the appropriate body mass Z-score. Patients with isolated bicuspid aortic valve without important stenosis or regurgitation and no more than mild aortic dilation (<40 mm) may participate in all competitive sports. Patients with moderate (<45 mm) aortic dilation that is stable (not rapidly progressive) may participate in low static/low-to-moderate dynamic competitive sports without risk of bodily collision. Patients with progressive (>5 mm per year) or severe aortic dilation (>45 mm) are permitted to engage in low static/low dynamic exercise only. Histologic abnormalities involving the elastic media at the site of the coarctation are integral to this lesion. Older unoperated patients are also at risk for the development of and rupture of intracranial aneurysms. Exercise capacity is reduced in these patients despite the adequacy of the repair (114,115). Chronically elevated systolic blood pressure may play a role in cardiovascular morbidity and mortality. Even in those patients who are normotensive at rest, a hypertensive response to exercise may be associated with left ventricular hypertrophy and abnormal vascular function (116,117,118). Endothelial dysfunction, reduced vessel elasticity, and enhanced baroreceptors may all play a role in the development of chronic systolic hypertension and the commonly found systolic hypertensive rise to graded dynamic or isometric exercise (119,120,121). Previous information regarding cardiac catheterizations is also important, particularly in patients who have had balloon dilation of native coarctation or dilation of recurrent/residual coarctation. The presence of an upper-to- lower extremity blood pressure gradient should alert the physician to the presence of a possible residual coarctation. Maximal exercise testing is useful to assess the blood pressure response to exercise in these patients. This may be related to residual abnormal vascular reactivity that may be seen in these patients as stated above. Leisure Activities and Activities of Daily Living Many studies have examined exercise performance in patients with repaired coarctation of the aorta but longitudinal data regarding the risk of intense exercise participation and training are sparse. Those patients with hypertension in the absence of residual coarctation should follow the recommendations listed later in this chapter for systemic hypertension. Patients with a bicuspid aortic valve should follow the recommendations for bicuspid valves in Table 10. Competitive Sports Patients with isolated coarctation of mild degree (<20 mm Hg systolic blood pressure gradient) may participate in all sports; however, activities that have a maximally strenuous isometric component should probably be discouraged. Patients with residual obstruction should be referred for either catheter-based or surgical intervention prior to participating in competitive sports (82). Resting or exercise-induced hypertension in the absence of a residual gradient should be treated as discussed in the section on systemic hypertension. As with recreational activities, competitive sports in patients with repaired coarctation and bicuspid aortic valve should defer to the section on bicuspid aortic valve. The degree of obstruction is variable, but is typically mild and may regress spontaneously. More advanced obstruction results in right ventricular hypertrophy and/or strain, and if left untreated, can result in exercise intolerance (122), and/or atrial arrhythmias secondary to right atrial dilation. Most patients with advanced obstruction benefit from intervention, typically balloon valvuloplasty. Freedom from reintervention and exercise capacity have been reported to be quite favorable; however, the long-term impact of chronic pulmonary regurgitation as a result of the intervention remains to be seen (123,124). Moderate (30 to 50 mm Hg peak gradient) stenosis may be well tolerated in children and adolescents and rarely effects performance. However, decreased exercise capacity may be seen in young and middle age adults even in the presence of preserved right ventricular systolic function.
Sinikar, 30 years: Of course, some of these genes may not be real, perhaps being incorrectly assigned as genes, but many will need to have their function assigned by other mechanisms. However, the pres- ence of distant metastasis is the only definitive evidence of malignant prolacti- noma. In normal postnatal development, many values normalize by 6 months of age, although changes can still be seen throughout childhood (3,4).
Rocko, 42 years: The lower right hand image shows the component of the mitral valve which inserts into the right ventricle (black arrow). Strategies: Epidemiology of Prevention Prevention is motivated by incentives and driven by evidence. Multiple capillaries originating from the peritruncal capillary ring then grow toward the aortic wall and penetrate it (Fig.
Miguel, 35 years: These include short oblique incision is made low in the right atrial free the kinking effect noted above. Lactotropes and somatotropes share a common origin dur- ing pituitary ontogenesis and this explains the development of stem cell ade- noma and mammosomatotropinoma. At the same time, there are also common themes in pathophysiology, presentation, and evaluation shared between entities.
Folleck, 37 years: There is scarring of the parenchyma of the upper half of the kidney indicating that the diagnosis is chronic pyelonephritis. Correction of atrioventricular septal defect: results influenced by Down syndrome? B: By the end of the first month of gestation, the common pulmonary vein establishes a connection between the pulmonary venous plexus and the sinoatrial portion of the heart.
Falk, 48 years: Approximately 50% of patients are covered by commer- Once again, this argues for the advantages of the higher vol- cial insurance companies, which, like the government payors, ume program, which allows this level of subspecialization. In small infants, because of the increased risk of femoral artery injury from the introduction of the dilating balloon catheters into the vessels, several other approaches to aortic valve dilation have been described. Prolonged application may cause gram-positive microorganisms to appear gram nega- tive, while short application may cause gram-negative microorganisms to appear gram positive.
Chris, 24 years: Radiotherapy can be delivered as conventional fractionated therapy or stereo- tactic radiosurgery. These blood pressures represent values measured in the sitting position using auscultation. A bicuspid aortic valve occurs in up to 80% of patients with a coarctation, and the valve may be stenotic or the annulus hypoplastic.
Mason, 22 years: Although the myo- tatic refexes and resistance to passive movements in her right limbs were slightly reduced, neither paralysis nor sensory disturbances were found in these limbs or in any other part of her body. This should be obtained between 15 and 60 minutes after com- pletion of the transfusion. The development of the connecting channels is followed by partial involution of the left side of the paired veins.
Jens, 28 years: Guidance for industry: patient-reported outcome measures: use in medical product development to support labeling claims: draft guidance. Missense mutations may result in either simple virilizing forms of disease or in non-classical form based on the particular mutations. Anterograde axonal transport, that is, movement from the cell body to the terminals, is of two main types: (1) fast transport of membranous organelles and synaptic vesicles or their precursors, and (2) slow transport of cytoskeletal materials.
Hamid, 64 years: Typically, other surgical teams are time from the moment of donor recovery to recipient implan- present on site to participate in the multiorgan recovery pro- tation. Health has been defined by the World Health Organization as “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity” (16). Genetic factors have a signifcant contribution to the fnal adult height of an individual.
Anog, 34 years: The pH of neutrality of blood retains during Cardiopulmonary Bypass its usual alkalinity relative to intracellular pH so that there Ectothermic (“cold-blooded”) animals and hibernating mam- is a constant hydrogen ion concentration gradient between mals have provided an opportunity for study of the alternative the intracellular and extracellular environments both at nor- methods whereby different species adjust their physiology mothermia and hypothermia. Overall, enterococcal endocarditis occurs much less frequently in children than in adults. Aleutian Island Earthquake, 1946 Stage 1 of the Disaster You are the governor of Hawaii, an island territory in the United States.
Marcus, 52 years: Bicuspid Aortic Valves Bicuspid or bicommissural aortic valves are the most common type of congenital heart malformation, estimated to occur in 0. As far as the limbs are concerned, the corticospinal tracts are usually considered to be completely crossed. Referred pain is the phenomenon in which pain is localized in a part of the body remote from its source.
Bradley, 29 years: However, at least two tests are required to establish the presence of hypercortisolemia in a patient with suspected Cushing’s syndrome to increase sensitivity of the screening tests. Diffusion-weighted imaging is the most sensi- raised intracranial pressure, focal neurological signs or tive method for the early detection of an infarct and will change in conscious level. Approximately 90% of patients with Cushing’s disease have microadenoma, while macroadenoma contributes to the rest.
Hatlod, 56 years: Matrix deposition during this period establishes a functionally competent ventricle, which provides structural stability necessary for transitioning from fetal to postnatal life (9). Quantitative real-time three-dimensional echocardiography provides new insight into the mechanisms of mitral valve regurgitation post-repair of atrioventricular septal defect. Strain rate is the speed at which the deformation occurs and is expressed as %/second.
Rufus, 31 years: The papillary muscles develop from compacting columns in the trabecular layer of the ventricular muscle. Abdominal radiography may dem- To enhance fuid excretion if oliguria persists, “mini- onstrate distention or an abnormal gas pattern, pneumatosis, volume dialysis” may be effective using 10 mL/kg of 1. However, even though one typically presumes muscle contraction leads to shortening, this occurs only with concentric contraction.
Jaffar, 38 years: The daily goals communication sheet: a simple and novel tool for improved communication and care. Chromosome abnormalities can be classified according to an increase or decrease in whole chromosome number (aneuploidy), an increase or decrease of part of a chromosome (duplication or deletion, partial trisomy, or partial monosomy), or a more complex rearrangement. These occlusion bodies consist primarily of a single protein, polyhedrin, which surrounds the viral particles and protects them from harsh environments.
Kamak, 58 years: With a conservative dilation of the aortic valve, the gradient should be reduced to a gradient equal to or less than 35 mm Hg. Significant ventricular hypertrophy substantially increases operative risk for Fontan operation because of associated ventricular diastolic abnormalities and elevated left ventricular end-diastolic pressure. Tumors thought to be suitable were structures within the anterior skull base are the anterior and tumors with a localized intracranial extension.
Cronos, 62 years: Tumoral calcinosis is a rare autosomal recessive metabolic disorder characterized by periarticular and surrounding soft tissue calcification. Eplerenone for early cardiomyopathy in Duchenne muscular dystrophy: a randomised, double-blind, placebo-controlled trial. The intracranial extracerebral vessels are con- tained within the subarachnoid space (Fig.
Murak, 50 years: Faeces cause a flling defect which can be very dif- fcult to distinguish from a polyp or tumour (Fig. In the presence of a balloon of the coronary arteries this height differential will usually atrial septal defect the single atrial cannula also functions as result in the bottom of the “U” being at the level of the tops a left atrial vent and drains left heart return which can oth- of the commissures of the neoaortic valve. Careful consideration must be given to cases on an individual basis prior to committing to long-term support as our surgical and postoperative management experience with these patients and devices is still in its infancy.
10 of 10 - Review by X. Kalesch
Votes: 233 votes
Total customer reviews: 233
References
- Badesch DB, Abman SH, Simonneau G, et al: Medical therapy for pulmonary arterial hypertension: updated ACCP evidence-based clinical practice guidelines, Chest 131(6): 1917-1928, 2007.
- Kannangai R, Wang J, Liu QZ, et al. Survivin overexpression in hepatocellular carcinoma is associated with p53 dysregulation. Int J Gastrointest Cancer. 2005;35:53-60.
- Boyce WH, King JS Jr: Crystal-matrix interrelations in calculi, J Urol 81:351, 1959.
- Georghiou GP, Boikov O, Vidne BA, Saute M. Primary pulmonary amyloidosis due to low-grade B cell lymphoma. Asian Cardiovasc Thorac Ann 2007;15:69-71.
- Scherer LA, Battistella FD, Owings JT, et al. Video-assisted thoracic surgery in the treatment of posttraumatic empyema. Arch Surg. 1998;133(6):637-642.
- Hamer AW, et al. Failure of episodic high-dose oral verapamil therapy to convert supraventricular tachycardia: a study of plasma verapamil levels and gastric motility. Am Heart J 1987;114:334-342.
- Masetti R, Pirulli PG, Magno S, et al. Oncoplastic techniques in the conservative surgical treatment of breast cancer. Breast Cancer. 2000;7(4):276-280.
- Grocott HP, Mathew JP, Carver EH, et al: A randomized controlled trial of the Arctic Sun temperature management system versus conventional methods for preventing hypothermia during off-pump cardiac surgery, Anesth Analg 98:298, 2004.