Carey Kernodle Anders, MD
- Instructor in the Department of Medicine
- Member of the Duke Cancer Institute

https://medicine.duke.edu/faculty/carey-kernodle-anders-md
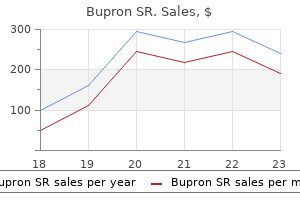
Bupron SR dosages: 150 mg
Bupron SR packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Buy 150 mg bupron sr otc
The concern in this instance is related to potential air being trapped between the cast and the immobilized extremity bipolar depression in adolescents generic bupron sr 150 mg online. Of course anxiety urban dictionary buy 150 mg bupron sr with amex, if medically prudent and appropriate from an orthopedic care perspective depression sous jacente definition buy discount bupron sr 150 mg on-line, the cast can be bivalved to prevent uncomfortable or dangerous gas expansion. Patients who have undergone neurosurgical procedures should delay air travel for 1 week due to the possibility of entrapped, residual gas within the cranial vault. Patients status post-ophthalmologic procedures and/or penetrating eye trauma should avoid travel for a similar time period. Air travel should not be undertaken for 2–6 weeks depending on the type of gas used in the procedure [25]. The “medical common sense” approach will assist with an analysis of the appropriateness of nonurgent commercial air travel for patients with infectious disease. Medical stability regard- ing the obvious issues, such as cardiovascular, respiratory, and neurologic systems, must be addressed and can certainly preclude nonurgent air travel. Common instances in which such air travel is not appropriate include the patient with bacte- rial meningitis, the patient with pneumonia complicated by respiratory compro- mise, the patient with pyelonephritis experiencing continued pain and inability to take nutrition, fuids, and medications orally, and the patient with soft-tissue infection-related sepsis. Other situations in which air travel likely is not inappropri- ate include uncomplicated infections such as cellulitis and cystitis, assuming that the patient has been treated with antimicrobial agents for several days. Certain infections, while not always problematic from the medical care per- spective (i. Otitis media with middle- ear effusion, and sinusitis with signifcant congestion can create discomfort and/ or tissue damage related to the inability to equalize body cavity pressures as fight elevation changes. Communicable infectious illness may be transmitted to other travelers during air travel. Potential passengers who are either potentially or acutely ill with an infec- tious syndrome should delay travel until they are no longer contagious. A conta- gious illness should be considered at minimum a relative contraindication to nonurgent, commercial air travel. While a number of infectious illnesses have spe- cifc air travel restrictions, the more commonly encountered entities involve trans- mission via respiratory secretions, including tuberculosis, meningitis (caused by Neisseria meningitides), measles, and infuenza. Each of these infectious illnesses has been documented to have spread among passengers during commercial air travel [30]. If travel with a potentially infectious patient has occurred, then fellow passengers should be notifed of poten- tial contagion. Meningococcal illness, specifcally meningitis or disseminated meningococcal disease caused by Neisseria meningitides, is a contagious illness which is rapidly fatal. For this reason, any patient with known or suspected illness must be absolutely prohib- ited from all commercial air travel. Fellow passenger exposures requiring chemo- prophylaxis include the following: household member or intimate contact traveling with the patient, traveling companion of patient, fellow passengers seated adjacent to the patient on prolonged fights (defned as longer than 6–8 h), and any passenger or fight crew member with exposure to respiratory secretions. Measles, another infectious illness with signifcant contagious potential, is caused by the measles or Rubeola virus. Measles is transmitted by either direct contact with respiratory secretions or the patient with exposed secretion. The illness can also be spread via the airborne route by aerosolized respiratory secretions. Considering these two routes of contagion, patients with known or suspected measles should be abso- lutely prohibited from commercial air travel. Recall that patients are contagious for at least 4 days before development of the characteristic rash; the contagious period also extends for at least another 4–6 days of active illness. Fellow passengers exposed to measles should be notifed and unimmunized considered for prophylactic therapy. Lastly, infuenza is one of several respiratory viruses with the potential for contagion in the confnes of a commercial aircraft cabin. As with the other microbes discussed above, the infuenza virus is disseminated via respiratory secretions, specifcally large droplet secretions. The contagious period for the fu ranges from approximately 1 day prior to the onset of symptoms up to a week of active illness. As with other syndromes noted above, patients suspected of infu- enza infection should be prohibited from commercial travel of any sort, including via air [30, 34].
Gossypol. Bupron SR.
- How does Gossypol work?
- Dosing considerations for Gossypol.
- Are there any interactions with medications?
- Male contraception (birth control), when taken by mouth.
- Are there safety concerns?
- Use as a vaginal spermicide, problems of the uterus (womb) and ovaries, HIV/AIDS, cancer, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96148
150 mg bupron sr order mastercard
We want to know the probability of obtaining no more than two pluses out of 11 tries when the null hypothesis is true biochemical depression definition cheap 150 mg bupron sr free shipping. As we have seen anxiety 60 mg cymbalta 90 mg prozac 150 mg bupron sr order amex, the answer is obtained by evaluating the appropriate binomial expression depression gene order bupron sr 150 mg line. In this example we find X2 k 11Àk Pk 2 j11;:5 11CkðÞ:5 ðÞ:5 k¼0 By consulting Appendix Table B, we find this probability to be. We have also seen that the alternative hypothesis may lead to either a one-sided or a two-sided test. In either case we concentrate on the less frequently occurring sign and calculate the probability of obtaining that few or fewer of that sign. We use the least frequently occurring sign as our test statistic because the binomial probabilities in Appendix Table B are “less than or equal to” probabilities. By using the least frequently occurring sign, we can obtain the probability we need directly from Table B without having to do any subtracting. If the probabilities in Table B were “greater than or equal to” probabilities, which are often found in tables of the binomial distribution, wewould use the more frequently occurring sign as our test statistic in order to take advantage of the convenience of obtaining the desired probability directly from the table without having to do any subtracting. In fact, we could, in our present examples, use the more frequently occurring sign as our test statistic, but because Table B contains “less than or equal to” probabilities we would have to perform a subtraction operation to obtain the desired probability. If we use as our test statistic the most frequently occurring sign, it is 9, the number of minuses. The desired probability, then, is the probability of nine or more minuses, when n ¼ 11 and p ¼ :5. That is, we want Pk¼ 9 j 11;:5 However, since Table B contains “less than or equal to” probabilities, we must obtain this probability by subtraction. Sample Size We saw in Chapter 5 that when the sample size is large and when p is close to . The rule of thumb used was that the normal approximation is appropriate when both np and nq are greater than 5. When p ¼ :5, as was hypothesized in our two examples, a sample of size 12 would satisfy the rule of thumb. Following this guideline, one could use the normal approximation when the sign test is used to test the null hypothesis that the median or median difference is 0 and n is equal to or greater than 12. Since the procedure involves approximating a continuous distribution by a discrete distribution, the continuity correc- tion of. Subjects took digoxin with water for 2 weeks, no digoxin for 2 weeks, and digoxin with grapefruit juice for 2 weeks. The average peak plasma digoxin concentration (Cmax) when subjects took digoxin with water is given in the first column of the following table. The second column gives the Cmax concentration when subjects took digoxin with grapefruit juice. May we conclude on the basis of these data that the Cmax concentration is higher when digoxin is taken with grapefruit juice? If we have a small sample n < 30 from a population that is known to be grossly nonnormally distributed, and the central limit theorem is not applicable, the z statistic is ruled out. When confronted with such a situation we usually look for an appropriate nonparametric statistical procedure. As we have seen, the sign test may be used when our data consist of a single sample or when we have paired data. If, however, the data for analysis are measured on at least an interval scale, the sign test may be undesirable because it would not make full use of the information contained in the data. A more appropriate procedure might be the Wilcoxon (1) signed-rank test, which makes use of the magnitudes of the differences between measurements and a hypothesized location parameter rather than just the signs of the differences. Assumptions The Wilcoxon test for location is based on the following assumptions about the data. Hypotheses The following are the null hypotheses (along with their alternatives) that may be tested about some unknown population mean m0. Subtract the hypothesized mean m0 from each observation xi, to obtain di ¼ xi À m0 If any xi is equal to the mean, so that di ¼ 0, eliminate that di from the calculations and reduce n accordingly. Rank the usable di from the smallest to the largest without regard to the sign of di. That is, consider only the absolute value of the di, designated jjdi , when ranking them. If two or more of the jjdi are equal, assign each tied value the mean of the rank positions the tied values occupy.
Bupron sr 150 mg buy line
Structural support of the urethra as it relates to stress urinary incontinence: The hammock hypothesis online depression test buy 150 mg bupron sr with amex. Aspects on the anatomy of the female urethra with special relation to urinary continence trade depression definition discount bupron sr. On the physiology of continence and pathophysiology of stress incontinence in the female juvenile depression test order 150 mg bupron sr visa. Location of maximal intraurethral pressure related to urogenital diaphragm in the female subject as studied by simultaneous urethrocystometry and voiding urethrocystography. Different biochemical composition of connective tissue in continent and stress incontinent women. International Continence Society 31st Annual Meeting proceedings, September 18–21, 2001, Seoul, Korea. An ambulatory surgical procedure under local anesthesia for treatment of female urinary incontinence. The Tension-free Vaginal Tape procedure is successful in the majority of women with indications for surgical treatment of urinary stress incontinence. Transobturator and retropubic tape procedures in stress urinary incontinence: A systematic review and meta-analysis of effectiveness and complications. Comparison of retropubic vs transobturator approach to mid-urethral slings: A systematic review and meta-analysis. Minimally invasive suburethral sling operations for stress urinary incontinence in women. Ten-year subjective outcome results of the retropubic tension-free vaginal tape for treatment of stress urinary incontinence. Serati M, Ghezzi F, Cattoni E, Braga A, Siesto G, Torella M, Cromi A, Vitobello D, Salvatore S. Tension-free Vaginal Tape for treatment of urodynamic stress incontinence: Efficacy and adverse effects at 10 year follow-up. Tension-free vaginal tape procedure without preoperative urodynamic examination: Long-term outcome. Eleven years prospective follow-up of the tension-free vaginal tape procedure for treatment of stress urinary incontinence. Long-term efficacy of the tension-free vaginal tape procedure for treatment of urinary incontinence. Seventeen years follow-up of the tension-free vaginal tape procedure for female stress urinary incontinence. The tension-free vaginal tape procedure in women with previous failed stress incontinence surgery. Tension-free vaginal tape procedure after previous failure in incontinence surgery. Tension-free vaginal tape procedure: An effective minimally invasive operation for treatment of recurrent stress urinary incontinence. Tension-free vaginal tape a suitable procedure for patients with recurrent stress 1147 incontinence. The management of recurrent cases after the Burch colposuspension: 7 years experience. Outcomes following repeat mid urethral synthetic sling after failure of the initial sling procedure: Rediscovery of the tension-free vaginal tape procedure. Repeat synthetic mid urethral sling procedure for women with recurrent stress urinary incontinence. A repeat mid-urethral sling as valuable treatment for persistent or recurrent stress urinary incontinence. Repeat mid-urethral sling for female stress incontinence after failure of the initial sling. Effectiveness of midurethral slings in recurrent stress urinary incontinence: A systematic review and meta-analysis. Surgical treatment of recurrent stress urinary incontinence in women: A systematic review and meta-analysis of randomized controlled trials. The efficacy of the tension-free vaginal tape in the treatment of five subtypes of stress urinary incontinence. Long-term outcome of tension-free vaginal tape procedure for treatment of female stress urinary incontinence with intrinsic sphincter deficiency.
Generic bupron sr 150 mg mastercard
A systematic review of the literature on the prevalence of sexual impairment in women with urinary incontinence and the prevalence of urinary leakage during sexual activity depression uncommon symptoms buy line bupron sr. Burch colposuspension for the treatment of coital urinary leakage secondary to genuine stress incontinence anxiety urination generic 150 mg bupron sr otc. Sexual function after vaginal surgery for stress incontinence: Results of a mailed questionnaire anxiety nos code purchase generic bupron sr canada. Sexual function after surgery for stress urinary incontinence and/or pelvic organ prolapse: A multicenter prospective study. Urinary complications and sexual function after the tension-free vaginal tape procedure. Impact of tension-free vaginal tape on sexual function: Results of a prospective study. Sexual function in women before and after suburethral sling operation for stress urinary incontinence: A retrospective questionnaire study. Sexual function after using tension-free vaginal tape for the surgical treatment of genuine stress incontinence. Sexual function and vaginal anatomy in women before and after surgery for pelvic organ prolapse and urinary incontinence. Impact of vaginal surgery for stress urinary incontinence on female sexual function: Is the use of polypropylene mesh detrimental? Transobturator surgery for female stress incontinence: A comparative anatomical study of outside-in vs inside-out techniques. Prospective multicentre randomised trial of tension-free vaginal tape and colposuspension as primary treatment for stress incontinence. Female sexual function after surgery for stress urinary incontinence: Transobturator suburethral tape vs. Incontinence-related quality of life and sexual function following the tension-free vaginal tape versus the “inside-out” tension-free vaginal tape obturator. Impact of incontinence surgery on sexual function: A systematic review and meta- analysis. Efficacy of tolterodine on overactive bladder symptoms and sexual and emotional quality of life in sexually active women. Tolterodine immediate release improves sexual function in women with overactive bladder. Sexual functioning in patients with lower urinary tract dysfunction improves after percutaneous tibial nerve stimulation. Impact of sacral neuromodulation on female sexual function and his correlation with clinical outcome and quality of life indexes: A monocentric experience. Epidemiology of genital prolapse: Observations from the Oxford Family Planning Association Study. Sexual function in women with pelvic organ prolapse compared to women without pelvic organ prolapse. Sexual function, delivery mode history, pelvic floor muscle exercises and incontinence: A cross-sectional study six years post-partum. Estrogen therapy in the management of urinary incontinence in postmenopausal women: A meta-analysis. Sexual and organ function in patients with symptomatic prolapse: Are pessaries helpful? Prospective evaluation of outcome of vaginal pessaries versus surgery in women with symptomatic pelvic organ prolapse. Changes in sexual function after treatment for prolapse are related to the improvement in body image perception. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Symptomatic and quality of life outcomes after site- specific fascial reattachment for pelvic organ prolapse repair. Randomised comparison of Burch colposuspension versus anterior colporrhaphy in women with stress urinary incontinence and anterior vaginal wall prolapse. The clinical and urodynamic effects of anterior vaginal repair and Burch colposuspension. Rectocele repair: A randomized trial of three surgical techniques including graft augmentation.
Order bupron sr 150 mg online
The suture passer is introduced through the abdominal wall through a stab wound (Fig depression jealousy order bupron sr line. The dimple in the skin can be fxed easily by pulling the skin away from the abdominal wall depression glass buy bupron sr 150 mg with visa. Tacks are then placed at the edge of the mesh as needed to decrease the risk of bowel herniation between the mesh and the abdominal wall depression after test e buy 150 mg bupron sr. The addition of a 5-mm port on the opposite side, if not previously placed, will help in placing tacks on the side that is close to the ports. At the end, Tisseel can be sprayed on the tacks and the edge of the mesh, which may help in decreasing adhesion of the bowel to the tacks; spraying Tisseel between the mesh and the fascia may also help reduce the risk of seroma formation (Fig. For the hernia around the xyphoid process or the ribs, one has to take down the falciform ligament and place the mesh above the liver. The anchoring of the mesh should use tacks or intracoporeal sutures, without use of a suture passer. For suprapubic hernias, the inferior border of the mesh should be fxed with tacks to the pubic bone and to Cooper’s ligament. Finally, hernias of the fank can possibly be more challenging, as they do not pres- ent as hernias but rather as eventrations due to muscular nerve atrophy. Pain Following Laparoscopic Ventral or Incisional Hernia Repair The disposition of the intercostal nerves shows that some minor injury to the nerves is unavoidable, especially with the suture and tack repair (Fig. The patient should be forewarned about the occurrence of postoperative pain during the preoperative clinic visit. Local injections are used, and sometimes removal of the responsible suture with the inherent neuroma is the last resort. This will separate the components of the large muscles of the abdomen Separation and reduce the size of the midline defect and consequently, the size of the mesh to be used. Three trocars are placed, one 10 mm under the costal margin, another 10 mm in the fank, and a fnal 5 mm trocar in the right lower quadrant (Fig. The Hasson tech- nique is used for the right upper quadrant port (A); the aponeurosis of the external oblique is identifed and opened, and a balloon dissector is infated beneath the external oblique and above the internal oblique to create a working space(Fig. A 10-mm trocar (B) in the fank is inserted into the space to allow for an electrical scissor to divide the fascia of the external oblique laparoscopically, just lateral to the rectus sheath going downwards towards the right lower quadrant (Fig. In order to divide the upper part of the exter- nal oblique fascia, a 5-mm trocar is inserted (C). The camera is moved from the right upper quadrant trocar to the middle 10 mm trocar, and a scissor is introduced into the 5 mm trocar to complete the division. After the component separation is fnished, it is possible to perform an incisional hernia repair using a smaller mesh, as the component separation allows the edges of the fascial defect to be brought closer together; alternatively, a full laparoscopic incisional hernia repair with a sublay mesh can be performed. The main advantage of the laparoscopic component separation technique is to avoid the risk of devascularizing the skin, which can occur with the open method. A initial introduction site for the balloon dissector, and the Hasson trocar for the camera; B trocar port for the electri- cal scissors; C additional 5 mm port for the scissor to fnish up the division of the cephalad portion of the external oblique fascia Laparoscopic Component Separation 179 Fig. This will achieve a separation of the components and a subsequent release of the tension on the closure of the defect 180 Chapter 11 Incisional and Ventral Hernia Repair Including Component Separation Selected Alvarez C (2004) Open mesh versus laparoscopic mesh hernia repair. N Engl J Med 351(14):1463–1465 Further Bingener J, Buck L, Richards M, Michalek J, Schwesinger W, Sirinek K (2007) Long-term Reading outcomes in laparoscopic vs open ventral hernia repair. Arch Surg 144(3):228–233 Malas M, Katkhouda N (2002) Herniation through the falciform ligament following lapa- roscopic surgery. Arch Surg 141(3):304–306 Splenectomy (Total and Partial) and 12 Splenopancreatectomy Preoperative Requirements and Workup Classic Laparoscopic Laparoscopic splenectomy is a diffcult procedure that should only be performed by an Splenectomy experienced laparoscopic surgeon or under the direct supervision of such a surgeon. The surgeon should check the instrument set personally to ensure that everything is available, specifcally clip appliers, atraumatic graspers, liver fan retractors, and an irrigation suction machine with the capacity for hydrodissection. An open tray with a number 10 or 20 blade should be immediately available in case there is a need for conver- sion. The anesthesiologist must make sure that there is a suitable blood and platelet supply in the operating room prior to the start of the procedure. The patient is safely secured on a bean-bag with the left side up at a 60° angle in reverse Trendelenberg and the left arm positioned as for a left lateral thoracotomy (Fig. This allows gravity to retract the abdominal organs and maximize the working space.
Order bupron sr 150 mg with mastercard
Increased risk of cognitive impairment or dementia in women who underwent oophorectomy before menopause depression test hospital purchase genuine bupron sr. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in postmenopausal women: The Women’s Health Initiative Memory Study: A randomised trial depression glass for sale discount bupron sr 150 mg with amex. Influences of cardio-respiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women frontal depression definition cheap bupron sr generic. Women’s health during mid-life survey: The use of complementary and alternative medicine by symptomatic women transitioning through menopause in Sydney. An alternative approach: A survey of alternative methods used by women in a consultant led specialist menopause clinic. Pharmacology of estrogens and progestogens: Influence of different routes of administration. Effects of low-dose hormone therapy on menopausal symptoms, bone mineral density, endometrium, and the cardiovascular system: A review of randomized clinical trials. Ultra low dose estradiol and norethisterone acetate: Effective menopause symptom relief. Effects of ultra-low dose transdermal oestradiol on bone mineral density: A randomised clinical trial. Effects of postmenopausal hormone replacement therapy on lipid, lipoproteins and apolipoprotein (a) concentrations: Analysis of studies published from 1974–2000. Risk of endometrial cancer following estrogen replacement with and without progestins. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. Incidence of cancer among women using long versus monthly cycle hormonal replacement therapy, Finland 1994–1997. New progestogens: A review of their effects in peri-menopausal and postmenopausal women. The 2013 British Menopause Society and Women’s Health Concern recommendations on hormone replacement therapy. Oral oestrogen and combined oestrogen/progestogen therapy versus placebo for hot flushes. Non-hormonal therapies for menopausal hot flashes: Systematic review and meta-analysis. Medicines and Healthcare Products Regulatory Agency and Commission on Human Medicines. Osteonecrosis of the jaws associated with the use of bisphosphonates: A review of 63 cases. Breast cancer and hormone replacement therapy: Collaborative reanalysis of data from 51 epidemiological studies of 52,705 women with breast cancer and 108,411 women without breast cancer. Effects of conjugated equine estrogens on breast cancer and mammography screening in postmenopausal women with hysterectomy. Health risks and benefits 3 years after stopping randomized treatment with estrogen and progestin. Changes in breast cancer incidence rates in the United States by histologic subtype and race/ethnicity, 1995 to 2004. Menopausal hormone therapy and risk of ovarian cancer: Systematic review and meta-analysis. Effects of estrogen plus progestin on gynecologic cancers and associated diagnostic procedures: The Women’s Health Initiative randomized trial. Risk of venous thromboembolic disease associated with hormonal contraceptives and hormone replacement therapy. Hormone replacement therapy and risk of venous thromboembolism in postmenopausal women: Systematic review and meta-analysis. Coronary heart disease events associated with hormone therapy in younger and older women: A meta-analysis. A window of opportunity: The reduction of coronary heart disease and total mortality with menopausal therapies is age and time dependent. Hormone therapy and the risk of stroke: Perspectives 10 years after the Women’s Health Initiative Trials. Reassessment of the cost-effectiveness of hormone replacement therapy in Sweden: Results based on the Women’s Health Initiative randomised controlled trial.
Syndromes
- Avoid overusing antibiotics. Overusing antibiotics can lead to antibiotic resistance.
- Plan for what help you will need when you come home from the hospital.
- Excessive urination at night
- Eat foods that are high in soluble fiber. These include oats, bran, split peas and lentils, beans (such as kidney, black, and navy beans), some cereals, and brown rice.
- The most common place for a surgical cut to be made is over the top of the head, from just above one ear to just above the other ear. The cut is usually wavy. Where the cut is made depends on the specific problem.
- Vision loss
- Having a blank look on the face
Order cheap bupron sr
The consultation may be better informed depression symptoms for males generic bupron sr 150 mg buy online, more efficient and effective as a result mood disorder list bupron sr 150 mg buy overnight delivery. Surveys of patients’ views commonly find that patients find the questionnaire that allows them to focus on problems that concern them juvenile depression symptoms buy generic bupron sr 150 mg on line, often in areas that are difficult to discuss openly, such as fecal incontinence and sexual dysfunction. The inclusion of free text items relating to patients’ personal goals enables the collection of qualitative data and a degree of self-expression beyond the scope of closed multiple choice questions. The questionnaire helps to differentiate and measure related conditions such as constipation and obstructed defecation, dyspareunia and prolapse, and stress and urge incontinence. This has proved particularly valuable in deciding whether or not urodynamic investigation is required prior to incontinence surgery. An overview of global pelvic floor health helps in managing expectations in patients with multiple conditions, for example, informing discussion regarding outcomes for overactive bladder symptoms in women undergoing stress incontinence surgery. Pressures on clinical time can result in important issues such as fecal incontinence being overlooked in women with urinary incontinence, dyspareunia, and vaginal dryness not being considered in women with prolapse. The impact of symptoms shown alongside domain scores assists in prioritizing key areas from the patient’s perspective; for example, some women with prolapse may be relatively asymptomatic or unbothered by prolapse-related symptoms and not requiring treatment. Women with dyspareunia and sexual dysfunction may be more appropriately prescribed Hormone Replacement Therapy than prolapse surgery. In relation to functional bowel problems, differentiating between obstructive defecation and constipation is important in women with rectocele. Measuring these parameters routinely, before and following intervention in larger cohorts of patients can provide greater insight into the impact that surgery for prolapse and incontinence has on wider aspects of pelvic floor function [16–19]. Well-informed and targeted referrals for patients not responding to conservative measures enable the initiation of appropriate treatment via streamlined pathways. When used earlier in the care pathway, this may help with triage to appropriate services, for example, to 253 physiotherapy for women with stress incontinence or to joint colorectal—urogynecology service for women with urinary and fecal incontinence. This may be particularly relevant in multidisciplinary case discussions, in related correspondence, and when coordinating and prioritizing a multidisciplinary approach. These voucher letters are issued by clerical staff and sent or given to patients along with their appointment details. Although the median completion time was 15 minutes, many patients take considerably longer than this and some require assistance from clinical staff or carers, which is recorded in the questionnaire. Early experience indicates the potential for improved efficiency as well as quality of care, particularly for follow-up patients. Women, given the option of attending the outpatient clinic or virtual clinic following prolapse surgery, most commonly choose the latter. Informing patients of the value and importance of questionnaire completion, both before and following, was felt to be important, as was the need for adequate resources and staff education in achieving this. When combined with referral letters, these elements provide significant insight into the 255 patient’s condition, enabling a focussed and effective consultation. Attempts to improve response rates include the use of reminders and explanatory letters, using higher font size (12) and the use of colored, headed paper for correspondence. Emphasizing the value to patients themselves and encouraging active participation and engagement (rather than passive acceptance) in their own health and healthcare may have additional benefits, for both patients and providers. Although levels of connectivity and computer literacy have increased substantially in recent years, increasing age and low socioeconomic status remain important barriers, though being female is a consistent positive predictor of eHealth use [23]. Women may seek the help of family members or close friends, though this may impact on the accuracy of data provided. There is an interest in developing questionnaires for other clinical areas and conditions; a generic platform questionnaire builder now supports the development of instruments in a variety of fields. A responsive patient-based measure of health as well as symptom severity and impact is a valuable addition in this context, providing initial assessment and patient-based measure of outcome, presented in a meaningful way. There is evidence that for sensitive issues, computer-assisted interviewing can enhance disclosure and openness. Addressing issues of access and compliance, particularly for patients with low socioeconomic status and advancing age is an important challenge.
Bupron sr 150 mg order fast delivery
Thus anxiety zoning out discount 150 mg bupron sr with amex, attention should be given to ensuring a constant 1:1 relationship between ventricular pacing and atrial activation mood disorder criteria 150 mg bupron sr for sale. Similar stimulation methods must be used depression effects 150 mg bupron sr purchase overnight delivery, therefore, when drug effects or other interventions are to be compared. Although the functional properties of conduction and refractoriness follow principles similar to those of antegrade studies, the most common site of retrograde delay and block is in the His–Purkinje system. Detailed assessment of retrograde conduction was limited in the past by the fact that the His bundle deflection was not uniformly observed during the basic drive, thus making the cases reported relatively selected. More recently, using bipolar electrodes with a 5-mm interelectrode distance and being extremely careful, we have been able to record retrograde His deflections during the ventricular-paced drive in up to 85% of our patients. A second limiting factor is that during ventricular extrastimuli the His deflection can be buried within the ventricular electrogram over a wide range of ventricular coupling intervals, therefore making measurements of ventricle to His bundle conduction times impossible in these circumstances. This technique, although not widely used, offers the best method of evaluating retrograde His–Purkinje conduction during programmed ventricular stimulation. Since a retrograde His potential may not be observed even at close coupling intervals in approximately 15% to 20% of patients using standard techniques (pacing the right ventricular apex), evaluation of His–Purkinje and consequently A-V nodal conduction is at best incomplete. The rationale for choosing S1-H2 is the observation in animals and in occasional patients that over a wide range of ventricular-paced rates, S1-H1 remains constant (Figs. The typical response shown in Figures 2-43 and 2-44 may be graphically displayed by plotting S1-S2 versus P. As noted, the ability to record a retrograde His deflection during the basic drive greatly facilitates analyzing the location of conduction delays and block. Similar retrograde His potentials and retrograde V-A conduction patterns have been observed during left ventricular stimulation (Fig. As the ventricular extrastimuli are delivered at progressively premature coupling intervals (S1-S2), progressive delay in retrograde His–Purkinje conduction (S2-H2) is noted (A, B). On the right, during para-Hisian pacing, a retrograde His is clearly seen prior to the echo beat. B–C: Progressive retrograde His–Purkinje conduction delay appears as S1-S2 shortens. Further shortening results in a decrease in A1-A2 and an increase in S2-A2 intervals. The exact site of this initial delay cannot always be determined because a His bundle deflection may not be observed. In the absence of a recorded retrograde His bundle deflection, the site of initial S2-A2 delay cannot be inferred to be in the A-V node. As S1-S2 is progressively shortened, a retrograde His deflection (H2) eventually appears after the ventricular electrogram recorded in the His bundle tracing. The converse of these observations occurs when stimulation is performed from the left ventricle. The routes of retrograde His–Purkinje conduction just described have been studied in detail by Akhtar et al. Had retrograde His potentials and right bundle potentials been seen during ventricular drive, it is probable that a greater percentage of patients would have had initial conduction over the right bundle with subsequent conduction over the left bundle. In patients who have pre-existent antegrade bundle branch block, retrograde block in the same bundle branch is common. In fact, when pacing is instituted from the ipsilateral ventricle, the V-H interval is usually so long that retrograde Hs, if seen, are usually observed after the local ventricular electrogram. Once a retrograde His bundle deflection is seen, progressive prolongation of His–Purkinje conduction (S2-H2) occurs as the S1-S2 interval decreases. In most cases, the increase in S2-H2 remains relatively constant for each 10-msec decrement in S1-S2, giving rise to a fixed slope of S2-H2/S1-S2. His–Purkinje refractoriness depends markedly on the cycle length; consistent shortening of S2-H2 at any given S1-S2 is noted at decreasing basic drive cycle lengths (S1- S1). Measurement of retrograde A-V nodal conduction time is best taken from the end of the His bundle deflection to the onset of atrial depolarization. In most instances, once a retrograde His bundle deflection appears, the S1-H2 curve becomes almost horizontal (Fig. This response results in a relatively constant input into the A-V node and consequently a fixed retrograde A-V nodal conduction time (H2-A2) (Figs. Occasionally, the increases in S2-H2 greatly exceed the decreases in S1-S2, giving rise to an ascending limb on the S1-H2 curve. During the ascending limb, retrograde A-V nodal conduction improves (shorter H2-A2) because A-V nodal input is less premature (shorter S1-H2).
Buy bupron sr 150 mg otc
Presenting and long-term clinical implications and fecundity in females with obstructing vaginal malformations anxiety girl trusted 150 mg bupron sr. Successful management of a thick transverse vaginal septum with a vesicovaginal fistula by vaginal expansion and surgery reactive depression definition purchase 150 mg bupron sr otc. Role of the gynecologic surgeon in the management of urogenital anomalies in adolescents postpartum depression definition wikipedia 150 mg bupron sr order mastercard. Mullerian duct anomalies diagnosed by saline contrast sonohysterography: Prevalence in a general population. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, Mullerian anomalies and intrauterine adhesions. Clinical implications of uterine malformations and hysteroscopic treatment results. Reproductive outcome after hysteroscopic metroplasty in women with septate uterus and otherwise unexplained infertility. Twin gestation occupying separate horns of a bicornuate uterus after in-vitro fertilization and embryo transfer. Laparoscopic amputation of a noncommunicating rudimentary horn after a hysteroscopic diagnosis: A case study. Anatomical variation in the rudimentary horns of a unicornuate uterus: Implications for laparoscopic surgery. Laparoscopic management of pregnancies occurring in non- communicating accessory uterine horns. Utero-vaginal anastomosis in women with uterine cervix atresia: Long- term follow-up and reproductive performance. Successful pregnancy after in-vitro fertilization and transmyometrial embryo transfer in a patient with congenital atresia of cervix: Case report. Vaginal neoplasia in a male-to-female transsexual: Case report, review of the literature, and recommendations for cytological screening. The Vecchietti operation for constructing a neovagina: Indications, instrumentation, and techniques. A simplified novel laparoscopic formation of neovagina for cases of Mayer–Rokitansky–Kuster–Hauser syndrome. Surrogate pregnancies in patients with Mayer-Rokitansky-Kustner-Hauser syndrome and severe teratozoospermia. Gestational carrier is an optimal method for pregnancy in patients with vaginal agenesis (Rokitansky syndrome). Reassessing fecundity in women with classical congenital adrenal hyperplasia: Normal pregnancy rate but reduced fertility rate. Consensus statement on 21-hydroxylase deficiency from the Lawson Wilkins Pediatric Endocrine Society and the European Society for Pediatric Endocrinology. Genital sensation after feminizing genitoplasty for congenital adrenal hyperplasia: A pilot study. Genital malformations and coexistent urinary tract or spinal anomalies in patients with imperforate anus. The surgical management of persistent cloaca: Results in 54 patients treated with a posterior sagittal approach. Vaginal switch—A useful technical alternative to vaginal replacement for select cases of cloaca and urogenital sinus. Pregnancy in patients with Turner’s syndrome: Six new cases and review of literature. The effect of hormone replacement therapy on cardiovascular hemodynamics in women with Turner’s syndrome. Many of the clinical abnormalities seen in girls and young women that appear to involve the genitalia alone may be the harbinger of related urinary tract disorders. Abnormalities presenting in infancy may be easy to recognize secondary to abnormal antenatal ultrasonographic or physical examination in the newborn period. Many urogenital malformations, however, are elusive and may become evident only after a clinical problem arises. The most common urogynecological disorders prompting childhood evaluation focus on problems of urinary continence and introital abnormalities. Interlabial masses, often included in the differential diagnosis of urinary incontinence, as well as difficulties with appropriate gender identification in genetic and phenotypic females, are discussed in this chapter.
150 mg bupron sr otc
This indicates slightly asymmetric margin of abrasion depression calculator test discount bupron sr 150 mg without prescription, which is greatest the bullet struck the body from a slightly inferior and left- at the 9 o’clock through 12 o’clock position bipolar depression bpd buy 150 mg bupron sr with amex, indicating the to-right trajectory depression era glass order 150 mg bupron sr with amex. The slightly irregular nature of the bullet struck the body with a slightly downward and right- margin of abrasion may sometimes be seen as the bullet to-left trajectory relative to the body. This bul- let frst perforated the bottom of a shoe and a sock before entering the body. This gunshot wound to the thick skin of the palm of the hand reveals typical small radiating lacerations without prominent margin of abrasion. These characteristics are typical for gunshot wounds of the palms of the hand and soles of the feet. Note that with approximation of the margins (lower images) the wound forms a roughly circular perforation with margin of abrasion typical of an entrance gunshot wound. Also note the copious amounts of soot within the wound track and on the underlying bone surface. Such large radiating linear lac- erations are usually associated with higher-caliber guns, and tight contact of the gun muzzle on the body surface with underlying bone close to the skin. The expanding gases from burning gunpowder forced into the wound track cause such lacerations. Larger lacerations are typically in older individuals, where skin is less elastic. These lacerations are caused by burning gunpowder with expanding gases forced into the wound track and causing the overlying skin to lacerate. Note the larger lacerations extending from the at the adjacent skin and within the wound track. The tension surrounding the wound is relieved by pressing the surrounding skin inward toward the perforation. Note that even after cleaning, small amounts of soot is still present at the wound margins. In many cases, such as this one, it was essential to frst photograph the body before cleaning. There is a minimal amount of soot at the adjacent skin, margin, and deep within the wound track. Note at the lower aspect of this perforation there is more of a circular pattern consistent with an entrance wound and at the superior aspect there are tears on each side (white arrows) causing wider separation and giving a slightly squared-off appearance. If the wound margins were approximated at the top, the wound would take on more of a circular appearance. It is very important to be very careful, when cleaning the wound for photographs, not to remove gunpowder residue soot. Note the abraded imprint of the eyepiece portion of the gun at the superior aspect. There is no obvious soot on the sur- face of the adjacent skin, but there are copious amounts of soot within the wound track. Note the pink to red discol- oration, surrounding the perforation, due to nitrates and carbon monoxide released from burning gunpowder. These components may sometimes cause this discoloration when reacting with the underlying muscle. Note the adjacent abrasion to the perforation site due to contact with a revolver ejector rod when the gun was discharged. There are also small amounts of soot visible at the wound margins and more within the wound track. Note the soot deposition surrounding the margin and the red discoloration of the adjacent skin. This is typically seen with a tight contact gunshot wound where soot is forced into the wound track. Note the gunpowder residue surround- fare burn and soot encircling the perforation site. The amount of gunpowder residue following discharge of a frearm may be quite variable and sometimes not very obvious. Multiple layers of heavy clothing may flter gunpowder residue from the body surface.
Uruk, 31 years: In the context of neurogenic bladder dysfunction, the clinical picture is complicated by an admixture of other functional problems associated with uncoordinated detrusor contractions, poor bladder compliance, and varying degrees of sphincteric obstruction.
Derek, 24 years: Ringworm (Tinea) from cats, dogs and Direct contact transmission: In horizontal other domestic animals.
Mojok, 38 years: The final phase of this process is a publication of the final consensus statement.
Finley, 62 years: Defecating Proctography Defecating proctography is regarded as the gold standard investigation for evacuatory dysfunction.
Sulfock, 29 years: Toward that end, they collected a national sample of African-American, Caucasian, Hispanic, and Asian-American respondents.
Cruz, 63 years: Comparative effects of quinidine and amiodarone in monomorphic ventricular tachycardia.
Inog, 43 years: Atopic dermatitis, a chronic skin disease characterized by Avoidance of nonspecifc allergens like dust, nylon, erythema, exudation, lichenifcation and intense pruritis, feathers and animal dander.
Khabir, 46 years: Topical application of properties which include the capacity to inhibit overexpres- vitamin E has shown to induce smoothening of fine lines and sion of cyclooxygenase-2 and nitric oxide synthase [82] and wrinkles whereas when given as a diet supplement, a lim- has been shown to have photoprotective and anticarcinogenic ited cutaneous bioavailability was indicated which is insuf- activities [83].
Thordir, 45 years: It is characterized by focal inflammatory and demyelinating lesions of the nervous system, affecting mainly those living in the temperate climates.
Pakwan, 47 years: A significant decrease of uroflow rate was documented during intravenous tocolysis with α-adrenoceptor agonists.
Vibald, 55 years: Among the data collected were the following measurements on plasma T4 (nmol/L) levels at screening: Severe Cases Moderate Cases T4 T4 T4 Sex (nmol/L) Sex (nmol/L) Sex (nmol/L) M 16 F 20 F 62 M 57 F 34 M 50 M 40 F 188 F 40 F 50 F 69 F 116 F 57 F 162 F 80 F 38 F 148 F 97 F 51 F 108 F 51 F 38 F 54 F 84 Ã M F F F 60 M 76 F 94 M 122 M 158 M F Ã F M F 29 M 143 F 83 M 128 F 62 M 112 M 111 Ã ¼ Missing data.
Gorn, 57 years: The catheters are fixed in place by tape close to the external urethral meatus on the medial aspect of the thigh.
Saturas, 41 years: Watson has described using the Endo Stitch (a laparoscopic suturing instrument) to pass the suture through the sacrospinous ligament.
Delazar, 49 years: The com- were composed of aluminium oxide, or crystals of sodium plete healing occurs in 2–3 weeks [35 ].
Lester, 36 years: This is a tempo- removing fat from the deep layer or from the superficial rary phenomenon and normally disappears when the anterior one and we may easily risk to carry out an inappropriate plication of the platysma is completed.
Candela, 60 years: An incision is made for the nondominant hand the Splenectomy same size as the surgeon’s glove size (7.
Kent, 61 years: Its low pH and presence of fatty vaginal epithelium of prepubertal girl is more acid makes the environment inhospitable susceptible to gonococcal infection.
Mirzo, 26 years: Otherwise, which over time has been reduced, localizing mainly at the the surgery should be delayed in the case of a respiratory level of the mucosa of the lamina cribrosa of the ethmoid.
Hamid, 22 years: It courses in the superficial muscle layer and is variation in terms of shape, attachment, and bilateral easily visible and palpable during contraction.
Shakyor, 48 years: Glucocorticoids raise blood glucose by enhancing gluconeogenesis and inhibiting peripheral glucose uti- lization.
8 of 10 - Review by P. Chenor
Votes: 261 votes
Total customer reviews: 261
References
- Pierart J, Gyhra A, Torres P, et al: Causes of increasing pericardial pressure in experimental cardiac tamponade induced by ventricular perforation. J Trauma 35:834, 1993.
- Dielubanza EJ, Schaeffer AJ: Urinary tract infections in women, Med Clin North Am 95(1):27n41, 2011.
- Hofland CA, Eron LJ, Washecka RM. Hemorrhagic adenovirus cystitis after renal transplantation. Transplant Proc. 2004;36:3025-3027.
- Wicker G, Prill V, Brooks D, et al. Mucopolysaccharidosis VI (Maroteaux-Lamy syndrome). An intermediate clinical phenotype caused by substitution of valine for glycine at position 137 of arylsulfatase B. J Biol Chem 1991;266:27386.
- Harth, K. C., Rosen, M. J. Endoscopic versus open component separation in complex abdominal wall reconstruction. Am J Surg. 2010; 199:342-346.
- Bodenheimer MM, Sauer D, Shareef B, et al. Relation between myocardial infarct location and stroke. J Am Coll Cardiol 1994;24:61-6.