Valerie A. Holmes RGN, BSc, PGCHET, PhD
- Lecturer in Health Sciences
- School of Nursing and Midwifery
- Queen's University Belfast
- Belfast, Northern Ireland, UK
V-gel dosages: 30 gm
V-gel packs: 1 tubes, 2 tubes, 3 tubes, 4 tubes, 5 tubes, 6 tubes, 7 tubes, 8 tubes, 9 tubes, 10 tubes

Buy 30 gm v-gel mastercard
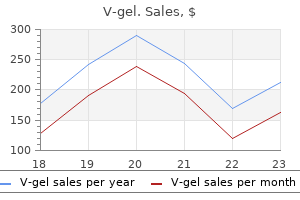
We conducted a sensitivity analysis excluding studies rated poor quality herbals books buy v-gel 30 gm online. Peer Review and Public Comment Original Drug Effectiveness Review Project reports are independently reviewed and commented upon by 3 to 5 peer reviewers vindhya herbals discount v-gel 30 gm buy. Peer reviewers are identified through a number of sources herbals for anxiety discount v-gel 30 gm line, including but not limited to professional society membership, acknowledged expertise in a particular field, prominent authorship in the published literature, or recommendation by Drug Effectiveness Review Project participating organizations. A list of individuals who have acted as peer reviewers of Drug Effectiveness Review Project reports is available on the Drug Effectiveness Review Project website. Peer reviewers have a maximum of 3 weeks for review and comment. They are asked to submit their comments in a standardized form in order to maintain consistent handling of comments across reports and to allow the Drug Effectiveness Review Project team to address all comments adequately. The Drug Effectiveness Review Project process allows for a 2-week public comment period prior to finalization of the report. Draft reports are posted on the Drug Effectiveness Review Project website and interested individuals or organizations can review the complete draft report and submit comments. Comments from peer reviewers and the public are entered into a spreadsheet and the disposition of each comment is tracked individually. RESULTS Overview Results of literature searches are shown in Figure 1. We retrieved 338 potentially relevant articles for review. Of these, 74 randomized controlled trials and 61 additional publications (other study designs) were included. Statins Page 16 of 128 Final Report Update 5 Drug Effectiveness Review Project Figure 1. Results of literature search a 11756 (3089 ): Total number of citations identified from searches and public comment 10965 (2751) excluded at title/abstract level 791 (338) articles retrieved for full- text evaluation 444 (203) articles excluded at full- text level: • 9 (8) foreign language • 94 (53) outcome not included • 18 (10) intervention not included • 37 (25) population not included • 148 (17) publication not included (letter, editorial, non-systematic review) • 138 (90) study design not included 347 (135) included studies: • 102(24) head-to-head trials • 29(25) active-control trials • 2(1) head-to-head and active-control trials • 92(24) placebo controlled trials • 80(38) observational studies • 21(8) systematic reviews b • 21(15) other a Numbers in parentheses are results of the literature search new to Update 5. Statins Page 17 of 128 Final Report Update 5 Drug Effectiveness Review Project Report Organization The results in this report are presented in two sections: one, results for adults, and two, results for children. How do statins and fixed-dose combination products containing a statin and another lipid-lowering drug compare in their ability to reduce low- density lipoprotein cholesterol? Summary of findings • For patients who required low-density lipoprotein cholesterol reductions of up to 35% to meet their goal, any of the statins were effective. Are there doses for each statin or fixed-dose combination product containing a statin and another lipid-lowering drug that produce similar percent reduction in low-density lipoprotein cholesterol? Statins 12, 13 We identified 88 randomized controlled trials and 2 meta-analyses comparing the low- density lipoprotein cholesterol-lowering ability of 2 or more statins in patients with baseline low- Statins Page 18 of 128 Final Report Update 5 Drug Effectiveness Review Project 14-29 30-78 density lipoprotein cholesterol less than 250 mg/dL or 6. In 51 of these trials, the percentage of patients reaching their National Cholesterol Education Program goal (or equivalent goal based on the country of origin of the study) was also evaluated. There were 40 double-blinded, 43 open-label, and 3 single-blinded studies, and dosing strategies varied between trials. Some studies titrated to a maximum recommended daily dose (titrate to target) while others compared fixed statin doses. One trial compared extended-release lovastatin 63 with the immediate-release form. One trial looked at the effects of switching to rosuvastatin 79 midway through the trial. Another study switched to pravastatin from simvastatin but was 80 given a poor quality rating, thus its data was not included in this report. The trials included men and women ages 18 and older who met low-density lipoprotein cholesterol criteria. Many of the trials had participants initially complete a placebo/dietary run-in phase before determining low-density lipoprotein eligibility. Most trials excluded patients with secondary hypercholesterolemia (uncontrolled diabetes, thyroid disease, or other endocrine condition), pregnant or lactating women, kidney or liver impairment, baseline creatine kinase elevation, triglycerides greater than or equal to 350 to 400 mg/dL, and those receiving drugs with the potential for drug interaction with statins. Most trials were of short duration (4 to 24 weeks) 81 although a few were significantly longer. In the majority of the trials the efficacy analyses were performed on a smaller number of patients than were randomized (that is, the trials did not use intention-to-treat statistics), although some trials used modified intention-to-treat analyses requiring that post-randomization data be available in order to include the results in the analysis.
30 gm v-gel amex
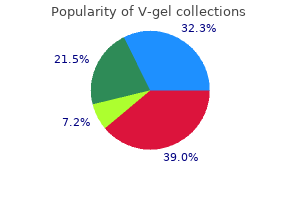
A Cancer and Leukemia Group B phoma Study Group (DSHNHL) sathuragiri herbals quality v-gel 30 gm. MYC gene rearrange- B-cell lymphoma with analysis of outcome by molecular subtype quantum herbals generic v-gel 30 gm with mastercard. Burkitt lymphoma pathogen- lymphoma with analysis of germinal center and post-germinal center esis and therapeutic targets from structural and functional genomics herbs chips buy v-gel once a day. Recurrent mutation of the subtypes of diffuse large B-cell lymphoma using gene expression in ID3 gene in Burkitt lymphoma identified by integrated genome, exome formalin-fixed paraffin-embedded tissue. PTEN loss defines a PI3K/AKT oncogenes by disruption of super-enhancers. PI3Kdelta inhibition by idelalisib in lymphomas: novel therapy of untreated Burkitt lymphoma (BL) and patients with relapsed indolent lymphoma. Tolani B, Gopalakrishnan R, Punj V, Matta H, Chaudhary PM. Rituximab plus cyclophos- Targeting Myc in KSHV-associated primary effusion lymphoma with phamide, doxorubicin, vincristine, and prednisolone in patients with BET bromodomain inhibitors. Inhibition of bromodo- comparison of dose intensification with 14-day versus 21-day cycles. Bhadury J, Nilsson LM, Veppil Muralidharan S, et al. BET and HDAC adult MYC-translocation-positive mature B-cell lymphomas other than inhibitors induce similar genes and biological effects and synergize to molecular Burkitt lymphoma. Phase II study of alisertib, MYC- or double-hit MYC/BCL2 translocations. Sheth A, Escobar-Alvarez S, Gardner J, Ran L, Heaney ML, Scheinberg lymphoma treated with rituximab. Inhibition of human mitochondrial peptide deformylase causes 391. MYC/BCL2 protein in newly diagnosed DLBCL is not associated with 41. SIRT4 protein suppresses tumor an inferior survival following EPOCH-R therapy [abstract]. Blood (ASH formation in genetic models of Myc-induced B cell lymphoma. Navitoclax, a targeted study of dose-modified CODOX-M/IVAC in patients with sporadic high-affinity inhibitor of BCL-2, in lymphoid malignancies: a phase 1 Burkitt lymphoma defined using cytogenetic and immunophenotypic dose-escalation study of safety, pharmacokinetics, pharmacodynamics, criteria (MRC/NCRI LY10 trial). ABT-199, a potent and rearrangements and IGH@BCL2/t(14;18)(q32;q21): an aggressive dis- selective BCL-2 inhibitor, achieves antitumor activity while sparing ease with heterogeneous histology, germinal center B-cell immunophe- platelets. Impact of induction regimen (GDC-0199) in patients with relapsed/refractory (R/R) non-Hodgkin and consolidative stem cell transplantation in patients with double hit lymphoma (NHL): Responses observed in diffuse large B-cell lym- lymphoma (DHL): a large multicenter retrospective analysis [abstract]. A small-molecule inhibitor of Anderson Cancer Center clinical experience. Margarete Fischer-Bosch Institute of Clinical Pharmacology, Stuttgart, Germany MYC, a member of the helix-loop-helix leucine zipper family of nuclear transcription factors, is a potent proto-oncogene primarily identified as the target of the t(8;14)(q24;q32) chromosome translocation in Burkitt lymphoma. Activation of the MYC gene in normal cells both results in enhanced cellular proliferation and up-regulation of pro-apoptotic pathways, reflecting the tight regulation of the molecule in the normal cellular system. In the process of transformation, these secondary inhibitory functions of the MYC molecule have to be overcome through secondary mutations of the MYC gene itself and/or by abrogating the inhibitory effects of physiological regulators and/or repressors of proliferation such as BCL2, BCL6, BLIMP1, or others. Most aggressive lymphomas, therefore, harbor additional oncogenic alterations that cooperate with MYC deregulation, with different alterations identified in human solid or hematological tumors. These alterations are likely to counteract the pro-apoptotic function of MYC. MYC gene alterations in diffuse large B-cell lymphomas and in B-cell lymphomas, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and Burkitt lymphoma are frequently associated with BCL2 or/and BCL6 translocations conferring a very aggressive behavior. This review summarizes inherent factors of the biology and function of MYC important in the process of transformation, especially taking account the interdependence of MYC on various cellular networks that have to be co-deregulated to achieve the full malignant phenotype. In addition, microRNAs pathways (miRs) have been found to assist in controlling its expression. MYC itself is activated by binding the histone acetyltransferases CBP/ p300 and TIP60/GCN5 or the transcription factor P-TEFb, among Introduction others. Transcriptional repression of MYC is mediated by interaction The expression of the proto-oncogene MYC is deregulated in a large with the transcription factor MIZ-1, which prevents recruitment of variety of cancers and, in these tumors, overexpression of MYC is the activating molecule p300 and enables binding of the gene- often associated with a poor prognosis. The MYC gene is located in silencing DNA-methyltransferase DNMT3a.
Diseases
- Toni Fanconi syndrome
- GMS syndrome
- Upton Young syndrome
- Apert like polydactyly syndrome
- Sciatica
- Zellweger syndrome
Effective v-gel 30 gm
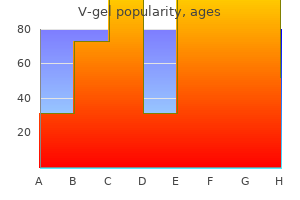
Pegylated interferons for hepatitis C Page 13 of 65 Final Report Drug Effectiveness Review Project Figure 1 herbals and supplements generic 30 gm v-gel free shipping. Results of literature search Step 1 829 titles and abstracts identified through searches Step 2 663 citations excluded (see report for criteria) Step 3 166 full-text articles retrieved for more detailed evaluation Step 4 74 articles excluded (see Appendix C) • 21 no original data (e herbs philipson buy genuine v-gel on-line. Two trials directly compared 50 herbs to lower cholesterol 30 gm v-gel order, 52 different doses of ribavirin as part of dual therapy with pegylated interferon. Two trials were 50, 63 included in more than one category. One head-to-head trial available as an abstract was excluded because it only reported 121 interim (8-week) results of a short-term (12 weeks) trial. We identified six other unpublished trials from pharmaceutical company dossiers that otherwise met inclusion criteria (Appendix D). These trials were not included in our primary analyses, but results were considered in sensitivity analyses in order to determine how they affected conclusions. A large (N=4913) trial compared weight-based to fixed, lower-dose ribavirin in patients on dual therapy with pegylated interferon 122 123-126 alfa-2b. The other five trials evaluated effects of different doses or duration of therapy 127 or compared effects of therapy in different racial groups. Overview of methodological quality of included trials Details of our quality assessment of included randomized controlled trials are shown in Evidence Table 3. Two of 41 included trials were rated good quality, 9 were rated poor, and the rest were fair (Table 4). Summary of quality assessment of included published trials Trial type Number of trials Good Fair Poor Head-to-head 2 0 1 1 Peg-IFN vs Non-peg 15 1 11 3 IFN Peg-IFN dual 5 0 4 1 therapy vs. Peg-IFN monotherapy Peg-IFN 19 1 14 4 dose/duration ranging Ribavirin dose 2 1 1 0 ranging Totals 43 3* 31* 9 *One trial included in more than one category Pegylated interferons for hepatitis C Page 15 of 65 Final Report Drug Effectiveness Review Project Key Question 1. What is the comparative effectiveness of regimens of peginterferon alfa-2a plus ribavirin versus peginterferon alfa-2b plus ribavirin for treatment of chronic hepatitis C virus infection? Summary of evidence We found insufficient evidence to determine if dual therapy with pegylated interferon alfa-2a is superior to dual therapy with pegylated interferon alfa-2b for achieving SVR or SBR. Head-to-head trials data were sparse (two trials), short-term (8 to 12 weeks), clinically diverse, and had methodological flaws. Indirect analysis of trials comparing dual therapy with pegylated interferon alfa-2a or alfa-2b to a common comparator (dual therapy with non-pegylated interferon) indicate no significant differences in rates of SVR, though interpretation of findings is limited by clinical diversity across trials and imprecise estimates of effects. Data on histologic outcomes and quality of life are sparse and there are no comparative data on other outcomes such as cirrhosis, hepatocellular cancer, liver transplant, or functional status. Effectiveness versus efficacy We considered all of the trials included in this report efficacy studies, as they generally applied numerous inclusion criteria, were conducted in specialty settings, used rigid dosing 128 regimens, and evaluated relatively short-term, intermediate outcomes (SVR and SBR rates). Systematic reviews We identified five systematic reviews (reported in six publications) on efficacy of dual 9, 13-15, 79, 80 therapy with pegylated interferon. All of the systematic reviews included the same 48 two published trials (one evaluating dual therapy with pegylated interferon alfa-2a and the 63 other pegylated interferon alfa-2b ). In both trials, dual therapy with pegylated interferon was compared to dual therapy with non-pegylated interferon or monotherapy with pegylated interferon. We excluded four of the systematic reviews because they did not assess comparative 9, 13-15, 79 efficacy of dual pegylated interferon regimens and are missing new, relevant trials. The fifth systematic review focused on efficacy of dual therapy with pegylated interferon in patients 79 with HCV genotype 4 infection and is reviewed for key question 3. Head-to-head trials Two head-to-head trials compared dual therapy with pegylated interferon alfa-2a versus 71, 72 pegylated interferon alfa-2b. Both were short-term (eight to twelve weeks) efficacy trials that only assessed end-of-treatment virologic responses. Results of the two trials cannot be directly compared or combined because of differences in study quality, patient populations, and interventions (Table 5). One trial (rated fair-quality), sponsored by the manufacturer of pegylated interferon alfa-2b, only included treatment-naïve patients infected with HCV genotype 1 and initially placed patients on four weeks of pegylated interferon monotherapy before 71 ribavirin was added for the last four weeks. The other trial, sponsored by the manufacturer of pegylated interferon alfa-2a, was rated poor quality (flaws include allocating consecutive patients to alternating therapy), did not restrict to genotype 1, initiated patients on dual therapy, and 72 included treatment-experienced patients (30% of enrolled population). In both trials, end-of- treatment virologic response was defined as >=2. Pegylated interferons for hepatitis C Page 16 of 65 Final Report Drug Effectiveness Review Project In the fair-quality trial, there was no significant difference (p=0.
V-gel 30 gm with amex
Data Sources We searched Ovid MEDLINE quality herbals products pvt ltd order v-gel 30 gm online, the Cochrane Database of Systematic Reviews herbs and uses generic 30 gm v-gel amex, and the Cochrane Central Register of Controlled Trials and Database of Abstracts of Reviews of Effects through January 2011 herbals on deck review cheap v-gel 30 gm without a prescription. We also hand searched reference lists, US Food and Drug Administration medical and statistical reviews, and dossiers submitted by pharmaceutical companies. Review Methods Study selection, data abstraction, validity assessment, grading the strength of the evidence, and data synthesis were all carried out according to standard Drug Effectiveness Review Project review methods. Results and Conclusions High-strength evidence indicated that in coronary revascularization, prasugrel reduces target- vessel revascularization more than clopidogrel at 15 months, while moderate-strength evidence indicated that there was more major bleeding with prasugrel. Evidence was moderate strength that the use of clopidogrel for 6 months after coronary revascularization resulted in lower risk of revascularization compared with 1 month, with no increase in bleeding (moderate strength). The benefit lessened after 8 and 12 months and bleeding risk gradually increased (moderate to low strength). In patients with acute coronary syndrome who are managed medically, there was moderate-strength evidence of no significant difference in reduction of mortality out to at least 12 months, significantly fewer myocardial infarctions, and increased major bleeding between clopidogrel plus aspirin compared with aspirin alone. Following stroke or transient ischemic attack, high-strength evidence indicated that extended-release dipyridamole plus aspirin did not meet criteria for being noninferior to clopidogrel for the primary outcome of recurrent stroke and had higher risks of major bleeding and withdrawals due to adverse events. Evidence was insufficient to draw strong conclusions about the benefit-risk ratio of using a proton pump inhibitor for any patients taking clopidogrel. Newer antiplatelet agents 3 of 98 Final Update 2 Report Drug Effectiveness Review Project TABLE OF CONTENTS INTRODUCTION.......................................................................................................................... For adults with acute coronary syndromes or coronary revascularization via stenting or bypass grafting, prior ischemic stroke or transient ischemic attack, or symptomatic peripheral vascular disease do antiplatelet agents differ in effectiveness?............................................................................ For adults with acute coronary syndromes or coronary revascularization via stenting or bypass grafting, prior ischemic stroke or transient ischemic attack, or symptomatic peripheral vascular disease do antiplatelet agents differ in harms?....................................................................................... For adults with acute coronary syndromes or coronary revascularization via stenting or bypass grafting, prior ischemic stroke or transient ischemic attack, or symptomatic peripheral vascular disease do antiplatelet agents differ in effectiveness and harms based on duration of therapy? Are there subgroups of patients based on demographics (age, racial groups, gender), socioeconomic status, other medications (drug-drug interactions), comorbidities (drug-disease interactions), or pregnancy for which one antiplatelet agent is more effective or associated with fewer harms? Definitions of the grades of overall strength of evidence........................................................... Pooled relative risks of major outcomes for the comparison of each newer antiplatelet agent with aspirin alone following stroke or transient ischemic attack............................................................... Detailed outcome data from pooled analysis of dual antiplatelet therapy length postpercutaneous coronary intervention.................................................................................................. Clopidogrel plus aspirin compared with aspirin alone: Pooled relative risks (95% confidence intervals) for outcomes from CREDO, CURE, and CHARISMA.............................................................. Stroke or vascular event rates in ESPS-2: extended-release dipyridamole/aspirin or aspirin monotherapy............................................................................................................................................. Gastrointestinal outcomes with concomitant proton pump inhibitor use in observational studies of high-risk patients.................................................................................................................................. Nonfatal and fatal bleeding events in Sorensen 2009................................................................ Revascularization risk at 6 months, 8 months, and 12 months................................................ Major bleeding risk at 6 months, 8 months, and 12 months..................................................... Results of literature search from Original Report and Update 1.......................................... Newer antiplatelet agents 6 of 98 Final Update 2 Report Drug Effectiveness Review Project Acknowledgments We thank Leah Williams, our publications editor, for putting this report into its present form for you to read. Suggested Citation Ketchum K, Peterson K, Thakurta S, Low A, McDonagh M. Prepared by the Oregon Evidence-based Practice Center for the Drug Effectiveness Review Project. Dailey, PharmD Peter Glassman, MBBS, MSc Marika Suttorp, MS Susan Chen, BA Southern California Evidence-based Practice Center, RAND Original Report authors Janet H. Dailey, PharmD Peter Glassman, MBBS, MSc Marika Suttorp, MS Cony Rolón, BA Southern California Evidence-based Practice Center, RAND Funding The Drug Effectiveness Review Project, composed of 12 organizations including 11 state Medicaid agencies, and the Canadian Agency for Drugs and Technology in Health commissioned and funded for this report. These organizations selected the topic of the report and had input into its Key Questions.
Buy 30 gm v-gel fast delivery
Therapeutics) all testing liver-directed adeno-associated viral (AAV) vectors encoding FIX for the treatment of hemophilia B herbs that heal v-gel 30 gm order free shipping. Of these Origins and limitations of FVIII and FIX biosynthesis trials herbalstarcandlescom generic 30 gm v-gel overnight delivery, only initial results from the St herbs nyc cake 30 gm v-gel buy. However, a prerequisite of this approach is the which is the 5-fold more prevalent form of the disease. Most endogenous expression of the deficient protein by the donor cells. It recently, in June 2014, Bayer HealthCare agreed to a collaboration has been known for decades that orthotopic liver transplantation with Dimension Therapeutics to commercialize another indepen- cures hemophilia in dogs and humans. This is not unexpected given dent AAV gene therapy product for hemophilia A. As these that vitamin K–dependent coagulation factors such as FIX require activities clearly indicate, gene therapy of hemophilia is being the activities of 2 proteins highly expressed in hepatocytes, gamma- aggressively pursued and multiple commercial entities have active glutamyl carboxylase and vitamin K epoxide reductase. However, preclinical and clinical hemophilia gene therapy pipeline programs several paradoxical observations surrounding FVIII biology made (Table 1). First, it was known that FVIII levels increase during fulminant hepatic failure, whereas Stem cells as therapeutics the levels of all other coagulation factors decrease. Second, it was One anticipated shortcoming of AAV-based gene therapy ap- observed clinically that FVIII levels did not decrease in the recipient proaches is limited therapeutic duration due to the turnover of the of a liver from a donor with mild hemophilia. In contrast, targeting stem cells has been widely speculated that both hepatic and extrahepatic for genetic modification and delivery of FVIII or FIX theoretically sources of FVIII exist, a role likely held by endothelial cells of both presents as the most durable approach. In the simplest sense, stem the liver sinusoids and elsewhere. However, it was not until early cells can be defined as undifferentiated cells that possess 2 key 2014 that endothelial cells clearly were identified as the primary properties, self-renewal and potency (ie, cellular differentiation endogenous source of FVIII by the Montgomery and Ginsburg potential). From a clinical perspective, these properties endow stem laboratories using distinct murine genetic engineering approaches cells with the ability to not only treat, but also to cure a multitude of involving cell type–specific F8 and Lman1 gene conditional knock- human diseases, which can include hemophilia. The first are the pluripotent stem cell (PSC) types that are endothelial cell and hepatocytes. They observed that endothelial naturally present during development. These include embryonic cells, but not hepatocytes, contained measurable levels of FVIII stem cells (ESCs) derived from the inner cell mass of a blastocyst, coagulant activity. Without clinical organs, which include BM-derived hematopoietic stem cells (HSCs) evidence of nonendothelial FVIII biosynthesis and nonhepatocyte and mesenchymal stem cells (MSCs). Currently, our understanding FIX biosynthesis and with no existing source/transplantation proto- of the clinical translatability of ESCs, EGCs, and iPSCs remains the cols for endothelial or hepatocyte stem cells, allogeneic transplanta- least mature because their safety, manufacturing, and efficacy have tion does not appear to be a viable near-term option. Therefore, in yet to be rigorously established and significant scientific challenges the near future, stem cell–based therapy strategies for hemophilia A remain. However, despite these deficiencies, several clinical trials and B likely will remain dependent on gene transfer technology. Following up on these findings, limiting and the primary determinants of this limitation are believed Oshimura et al genetically modified iPSCs derived from embryonic to be specific amino acid sequences within the molecule itself. For example, it was shown by Kaufman et al that h-FVIII mRNA expression was detected in the resulting cells. Nathwani et al combined a similar approach with codon optimiza- MSCs are an ideal cellular vehicle for the delivery of nucleic tion and demonstrated significant improvement in FVIII production acid–based therapeutics due to their ease of harvest, robust cell from liver-directed AAV gene transfer systems. How- differential occurs through reduced engagement of the unfolded ever, because MSCs have not been demonstrated in vivo to protein response pathway,10 and have used this information to regenerate or maintain a tissue compartment and thus do not meet generate humanized, human/porcine (HP) high-expression FVIII the strict definition of a stem cell, they also can be termed constructs that retain this biosynthetic advantage. Currently, MSCs are the subject of 500 strategy is being pursued in gene therapy applications for hemo- clinical trials for a wide array of medical conditions including, but philia B through the use of a naturally occurring human FIX variant not limited to , osteogenesis imperfecta, Crohn’s disease and ulcer- termed FIX-Padua (R338L) that exhibits greater specific procoagu- ative colitis, multiple sclerosis, diabetes, liver cirrhosis, and knee lant activity than wild-type human FIX. Inclusion of this modified cartilage injury, which as suggested by Ebihara et al, may be applicable to hemophilic joint arthropathy. However, the safety and transfer appears to be a necessary component for the clinical efficacy of these molecules remain to be tested and proven in utilization of MSCs toward correction of bleeding in hemophilia. Several groups of investigators are pursuing this approach and, of these, one particularly promising but preliminary study was con- ducted in an ovine model of hemophilia A. Genetically modified MSCs were trans- ongoing clinical trials of hESC-derived products and all except 1 planted into the peritoneal cavity of 2 affected hemophilia A target macular degeneration (acute wet age-related, Stargard’s, and recipients, the first of which already harbored a low-titer inhibitor against h-FVIIII and received a dose of 3 107 cells.
Syndromes
- Inability to relax
- Breathing tube
- Nuclear ventriculography (MUGA or RNV)
- Primary amyloidosis
- Severe pain or burning in the nose, eyes, ears, lips, or tongue
- Blood cortisol level
- Refusal to sit up, stand, or walk (younger child)
- The presence of other health problems in the baby
- Always ask for the small serving size.
Buy discount v-gel 30 gm line
The first trial randomized 60 participants meeting DSM-IV criteria for social anxiety disorder for at least 6 months to 14 weeks of fluoxetine (20-60 mg/d) or placebo herbs mopar buy generic v-gel 30 gm. Loss to follow-up was 20 percent with a higher rate in the placebo control group than the active fluoxetine group (23% compared with 16% herbs parts buy v-gel 30 gm low cost, respectively) herbals outperform antibiotics in treatment of lyme disease generic v-gel 30 gm with amex. Significant improvements in LSAS scores were reported for fluoxetine and placebo, with no statistically significant differences between groups (P=0. Secondary efficacy measures included the BSPS, FQ, HAM-A, HAM-D, Global Assessment of Functioning (GAF), and SF-36. Overall, no statistically significant differences were reported on secondary efficacy measures. Compared to placebo, fluoxetine-treated patients had a significant increase in the bodily pain subscale of the SF-36 (P=0. Significantly more fluoxetine-treated patients had asthenia than placebo-treated patients (P<0. However, we included only two arms—the fluoxetine arm and the placebo arm. Primary efficacy measures were the CGI-I, CGI-S and BSPS. CGI-I response rates were significantly higher in fluoxetine treated patients (51% compared with 32%). Fluoxetine-treated patients also showed a significantly greater improvement in CGI-S score from baseline (P<0. Second-generation antidepressants 68 of 190 Final Update 5 Report Drug Effectiveness Review Project 5. Other second-generation antidepressants compared with placebo Mirtazapine compared with placebo 218 One fair 10-week trial compared mirtazapine to placebo in 114 women with social phobia. The primary outcome measure was the change in SPIN score; LSAS and SF-36 scores also were assessed. After 10 weeks, mirtazapine-treated patients were significantly more improved than placebo-treated patients on the SPIN (difference in change = -8. Statistically significant differences were not noted in physical functioning (P=0. Nefazodone compared with placebo One fair trial compared nefazodone to placebo in adults meeting the DSM-IV criteria for general 219 social phobia for at least 1 year. The primary outcome measures were percentage of CGI-I responders (1 or 2) at endpoint and the mean change from baseline in LSAS total score. Secondary efficacy measures included CGI-S, Social Phobia Inventory, SPS, and Social Interaction Anxiety Scale. More nefazodone- than placebo-treated patients were CGI-I responders, but the difference was not significant (31. With the exception of the Social Phobia scale, there were no significant differences between groups in measures of social phobia. Nefazodone-treated patients had significantly higher incidences of some adverse events: dizziness (P<0. Summary of the evidence Three head-to-head trials compared one second-generation antidepressant to another for the treatment of social anxiety disorder. These trials suggest no differences in efficacy for escitalopram compared with paroxetine and venlafaxine ER compared with paroxetine. These findings were confirmed in a network meta-analysis that did not find any significant differences in any of the possible comparisons between venlafaxine ER, escitalopram, fluvoxamine, paroxetine, or sertraline. Additionally, indirect evidence from a meta-analysis of placebo- controlled trials provides evidence that there is no difference in efficacy between fluvoxamine, paroxetine, and sertraline. Effectiveness We did not identify any study with a high degree of generalizability. Efficacy One comparative trial provides fair evidence of comparable efficacy between escitalopram and 209 paroxetine for the treatment of social anxiety disorder. Two comparative trials provide fair 208, 210 evidence of comparable efficacy between venlafaxine ER and paroxetine. One meta- analysis of placebo-controlled studies provides fair evidence of comparable efficacies of 211 fluvoxamine, paroxetine, and sertraline for the treatment of social anxiety disorder. Second-generation antidepressants 69 of 190 Final Update 5 Report Drug Effectiveness Review Project One network meta-analysis of head-to-head trials and placebo-controlled studies provides fair evidence of comparable efficacy between escitalopram, fluvoxamine, paroxetine, sertraline 212 213 and venlafaxine ER.
Order v-gel 30 gm amex
Comparisons between oral and topical drugs • No significant differences were found between diclofenac 1 herbs life is feudal order v-gel 30 gm with visa. Nonsteroidal antiinflammatory drugs (NSAIDs) 18 of 72 Final Report Update 4 Drug Effectiveness Review Project Detailed Assessment Effectiveness Some trials evaluated longer-term (>6-12 months) and real-life (symptoms himalaya herbals 52 v-gel 30 gm purchase free shipping, clinical ulcers zordan herbals buy cheap v-gel, functional status, myocardial infarctions, pain relief) outcomes, but none were conducted in primary care or office-based settings or used broad enrollment criteria. Efficacy: Comparisons between oral drugs Celecoxib compared with nonselective NSAIDs 22-30 Eleven of 12 randomized controlled trials of arthritis patients found no significant difference in efficacy between celecoxib and an NSAID. The single study finding a difference was a randomized controlled trial of 249 randomized patients with severe osteoarthritis of the hip requiring joint replacement surgery. A significantly greater reduction in pain on walking was found for diclofenac 50 mg 3 times daily compared with celecoxib 200 mg once daily, as measured using an 100 mm visual analog scale, both in the primary 6-week assessment (difference, 12. However, insufficient information was provided to determine if an adequate method was used to conceal the allocation sequence or whether the approach produced treatment groups that were comparable at baseline in terms of important prognostic factors. Baseline characteristics were only provided for the evaluable population (N=141), which only accounted for 60% of the modified intention-to-treat population (N=235). Consequently, this randomized controlled trial was rated poor quality and its results should be interpreted with caution. The Agency for Healthcare Research and Quality Effective Health Care Program 31 Comparative Effectiveness Review found no clear differences in efficacy between celecoxib 22, 24, 26, 29 32, 33 and nonselective NSAIDs based on results from published trials and meta-analyses of published and unpublished trials. Celecoxib and nonselective NSAIDs were associated with similar pain reduction effects (Western Ontario and McMaster Universities Osteoarthritis Index, visual analogue scale, Patient Global Assessment) in published trials of patients with 22, 24, 26, 29 34, 35 36-38 29, osteoarthritis, soft tissue pain, ankylosing spondylitis, or rheumatoid arthritis. Celecoxib 200-400 mg was associated with slightly higher rate of withdrawals than other NSAIDs due to lack of efficacy (relative risk, 1. This estimate of comparative efficacy may be the most precise available, but the validity of the findings cannot be verified as the data used in this analysis is not fully available to the 33 public. On the other hand, ibuprofen 2400 mg/day and diclofenac 150 mg/day were associated with higher rates of withdrawal due to lack of efficacy than celecoxib 800 mg/day after 52 weeks (14. Nonsteroidal antiinflammatory drugs (NSAIDs) 19 of 72 Final Report Update 4 Drug Effectiveness Review Project Partially selective NSAIDs compared with nonselective NSAIDs Partially selective NSAIDs (meloxicam, nabumetone, and etodolac) were associated with similar pain reduction effects relative to nonselective NSAIDs in short-term randomized controlled trials. In 2 of the trials, however, patients taking nonselective NSAIDs were significantly less likely to withdraw due to lack of efficacy 44, 49 than patients taking meloxicam. A systematic review of 3 short-term randomized controlled trials of nabumetone for soft tissue pain found no difference in efficacy when compared with 50 ibuprofen or naproxen. However, based on physician assessment, the same systematic review also found placebo to be as efficacious as nabumetone in reducing pain at 7 days. Etodolac and nonselective NSAIDs were generally associated with similar rates of withdrawals due to 51 52 efficacy or improvements in pain in short-term randomized controlled trials of patients with osteoarthritis of the knee and/or hip. A sustained-release form of etodolac was also associated with similar rates of pain reduction relative to diclofenac in a small trial (N=64) of patients with 53 osteoarthritis of the knee. Comparisons among nonselective NSAIDs Several recent good-quality systematic reviews by the Cochrane Collaboration found no clear 51 differences among nonselective NSAIDs in efficacy for treating osteoarthritis of the knee, 54 55 hip, or low-back pain. Results from 3 fair-quality randomized controlled trials published subsequent to the Cochrane reviews also consistently found no significant differences in efficacy 56-58 among nonselective NSAIDs when used in patients with osteoarthritis. Limited evidence from 2 trials found no difference in efficacy when salsalate 3 g daily 59 60 was compared with indomethacin 75 mg daily or diclofenac 75 mg daily. No studies comparing salsalate to other NSAIDs were identified, and salsalate was not included in any of the systematic reviews included in this report. Tenoxicam 20 mg and 40 mg, diclofenac, and indomethacin were associated with similar 61 effects on pain in a good-quality systematic review of 18 randomized controlled trials. Tenoxicam was also associated with slightly greater improvements in pain management outcomes than piroxicam according to physician global assessment (odds ratio, 1. An older (1985) review of tiaprofenic acid 600 mg found no difference in efficacy when compared with aspirin 3600 mg, diclofenac 150 mg, ibuprofen 1200 mg, indomethacin 75-105 62 mg, naproxen 500 mg, piroxicam 20 mg, or sulindac 300 mg. A more recent randomized controlled trial confirmed the short-term comparative efficacy of tiaprofenic acid 600 mg and 63 indomethacin 75 mg (at 4 wks, 43% and 45% of patients showed improvement respectively). However, the same study found both drugs less efficacious in the long term (at 1 year, 39% for tiaprofenic acid and 36% for indomethacin). Efficacy: Comparisons between topical drugs We found no head-to-head trials that directly compared the effectiveness or efficacy of different topical drugs. Therefore, we considered indirect comparison of topical drugs based on 3 64-66 randomized vehicle-controlled trials of diclofenac 1. All trials 64-66, 68 67 enrolled patients with osteoarthritis of the knee or hand and ranged in duration from 4 65 66, 68 weeks to 12 weeks. Nonsteroidal antiinflammatory drugs (NSAIDs) 20 of 72 Final Report Update 4 Drug Effectiveness Review Project Among the trials of diclofenac 1.
30 gm v-gel buy with visa
In addition herbals nature cheap v-gel 30 gm overnight delivery, very few studies reported measures of dispersion (standard deviation or standard error) herbals dario bottineau 30 gm v-gel mastercard. We therefore used a qualitative approach to synthesis of these data verdure herbals generic v-gel 30 gm buy online. Comparison with Cochrane meta-analysis The results of this review and meta-analysis are consistent with a Cochrane review and meta-analysis of oral estrogens and menopausal hot flashes that includes trials published prior to Hormone therapy Page 35 of 110 Final Report Update 3 Drug Effectiveness Review Project 8 2000. The Cochrane review included double-blind, randomized, placebo-controlled trials of all forms of oral estrogen, alone or with progestin/progesterone, for at least 3 month’s duration. The meta-analysis reported weekly hot flash frequency and symptom severity. References were checked against the results of the OHP search. The OHP review differs from the Cochrane review because OHP defined a narrower range of oral agents, included transdermal forms, captured studies published after 2000, and included head-to-head comparisons. The Cochrane meta-analysis indicated a significant reduction in the weekly hot flash frequency for estrogen compared to placebo with a pooled weighted mean difference of –17. Severity of symptoms was also significantly reduced compared to placebo (odds ratio=0. Differences between types of estrogens were not determined, although trials of E2 and CEE predominated. The review also found that the reduction in weekly hot flash frequency was similar for opposed and unopposed estrogen regimens compared to placebo (opposed: 77. Symptom severity seemed to be better treated by opposed (odds ratio=0. However, differences between trials could also contribute to this discrepancy. Sleep disturbances/night sweats A trial of CEE in women with hot flashes and nighttime awakening at baseline indicated improvement in menopausal symptoms and measures of psychological well-being, but not in parameters of sleep quality such as total sleep time, sleep onset time, number of awakenings, 84 and REM sleep duration compared to placebo. Sleep disturbances were measured along with 85 other quality-of-life measures in a subset of 1511 women enrolled in the WHI. At one year of follow-up there was a small improvement (0. A trial of transdermal E2 indicated significant improvement in sleep quality, sleep onset, 86 and decreased nocturnal restlessness and awakenings compared to placebo. In this trial, participants on E2 were less tired in the daytime and had associated alleviation of vasomotor, somatic, and mood symptoms. Women with the worst insomnia had the best improvement with E2. Two other trials of transdermal E2 indicated significant declines in night sweats compared 68, 70 to placebo. A small, fair-quality trial of postmenopausal women taking oral conjugated equine estrogens did not find significant improvement in sleep 29 symptoms and a study of transdermal estradiol found an improvement in sleep at 12 weeks 33 41, 42 (p=0. Hormone therapy Page 36 of 110 Final Report Update 3 Drug Effectiveness Review Project Mood changes Nine trials of estrogen reporting mood outcomes met eligibility criteria, including one 17 45 trial comparing E2 and E2V, one of oral E2 compared to placebo, two of transdermal E2 87, 88 34,64, 89-91 compared to placebo, and five of CEE compared to placebo. In the head-to-head comparison trial of E2 and E2V, women were asked if symptoms of irritability, nervousness, anxiety, or depression were present or not before and after treatment cycles. Mood disturbances were more frequently reported by the E2 group (82%) than the E2V 17 group (68%) at baseline. At the end of treatment, symptoms were reduced to 52% in the E2 group compared to 44% in the E2V group (p=0. In placebo-controlled trials, one study that randomized early postmenopausal women to oral E2 reported significantly improved scores after one year on the Beck Depression Inventory (21 items) as well as on the manic-depressive melancholia subscale (12 items) and the anxiety 45 subscale (14 items), but not on the asthenia subscale or mania subscale. One trial of transdermal E2 enrolled 50 women meeting DSM-IV criteria for major depressive disorder (26 women), dysthymic disorder (11 women), or minor depressive disorder 87 (13 women). Remission of depression, measured by the Montgomery-Asberg Depression Rating Scale, was observed in 68% of women using E2 compared with 20% using placebo (p=0.
Purchase v-gel australia
The ongoing RESPONSE symptoms herbs during pregnancy purchase v-gel australia, including painful enlargement of the spleen and hemody- trial is evaluating ruxolitinib in PV and ET patients who are namic decompensation juvena herbals order 30 gm v-gel fast delivery. Among Back to the bench: understanding disease resistance ET patients herbals aps pvt ltd generic v-gel 30 gm with mastercard, 49% normalized platelet counts and 13/14 subjects with In MF, clinical resistance to JAK inhibition can manifest as 9 baseline platelet counts 1000 10 /L experienced a 50% worsening blood counts (which must be distinguished from drug- 54 reduction. In PV and ET, the effects of JAK inhibitors on related cytopenias), increasing splenomegaly, return of MF-related morbidity end points such as incidence of thrombosis or bleeding symptoms, and/or transformation to AML. In contrast to intermediate- or high-risk MF, where disease progression may occur despite using higher doses of JAK adjudicating effects on survival may be feasible, natural history inhibitors or in the setting of recurrent dose holds/reductions for studies in PV and ET are less tenable because of the long life hematologic or nonhematologic toxicity. Consensus definitions of clinical resistance to JAK inhibitor therapy are now being formulated to Potential uses of JAK inhibitors in other MPNs and guide physician management of patients. Although patients with myelodysplastic syndrome/MPNs “intolerance” or “resistance” to ruxolitinib are being evaluated in Therapeutic application of JAK inhibitors is being explored in the trials of alternate JAK inhibitors, the protocols do not use uniform less common MPNs that exhibit low-frequency V617F mutations55 criteria to define these terms. Thus far, sequencing of the JAK2 gene in small atypical CML, and refractory anemia with ring sideroblasts and numbers of patients has not uncovered acquired resistance muta- thrombocytosis. The JAK2 pathway mediates antiapoptosis signals tions. However, an vitro screen of libraries of mutagenized JAK2 in response to the eosinophilopoietic cytokines IL-5 and GM-CSF, V617F cDNA identified mutations in the drug-binding region that as well as the oncogenic tyrosine kinase FIP1L1-PDGFRA, suggest- confer resistance to ruxolitinib. In additional preclinical experiments, JAK2 V617F- in-depth responses indicate that ruxolitinib (and, by implication, expressing Ba/F3 cells exposed to ruxolitinib led to development of other JAK inhibitors) may be more effective when JAK2 activation drug-resistant subclones that carried a novel JAK2 variant missing is mediated by chromosomal rearrangement rather than by point amino acids 76-820. Recently, CSF3R (G-CSF receptor) mutations (FERM-JAK2). The FERM-JAK2 variant alters the JAK2 kinase were identified in 60% of CNL and atypical CML patients. This short-form variant of JAK2 has not yet been reported CSF3R T618I-mutated CNL patient with ruxolitinib resulted in a in patients on JAK inhibitor therapy. Another rational use of JAK mutation leading to constitutive signalling causes polycyth- inhibition is in Chuvash polycythemia, in which VHL mutants (eg, aemia vera. JAK2 V617F and beyond: role of genetics and SOCS1 and fail to form a heterodimeric E3 ligase that targets aberrant signaling in the pathogenesis of myeloproliferative phosphorylated JAK2 for ubiquitin-mediated destruction. Small-molecule inhibitors achieved among a subset of 18 patients with post-MPN AML, in myeloproliferative neoplasms: are we aiming for the right suggesting modest antileukemic efficacy in this patient population. The pseudokinase domain Summary of JAK2 is a dual-specificity protein kinase that negatively The unprecedented success of tyrosine kinase inhibitors in CML regulates cytokine signaling. Dusa A, Mouton C, Pecquet C, Herman M, Constantinescu SN. Improve- JAK2 V617F constitutive activation requires JH2 residue F595: ments in spleen size, symptom burden, and QOL represent clinically a pseudokinase domain target for specific inhibitors. Given that current JAK inhibitors are challenged polycythemia vera and idiopathic erythrocytosis. The JAK2 exon 12 mutations: A comprehensive a subset of patients and are generally modest in nature, review. MPLW515L is a novel mutant-specific JAK inhibitors are being pursued. Application of somatic activating mutation in myelofibrosis with myeloid JAK inhibitors in earlier stage MF, before genetic complexity and metaplasia. MPL515 mutations in in the pretransplantation setting also merit further study. Novel mutations in the The author thanks the Charles and Ann Johnson Foundation for their inhibitory adaptor protein LNK drive JAK-STAT signaling in support of the Stanford MPN Center. Frequent CBL Conflict-of-interest disclosure: The author has received research mutations associated with 11q acquired uniparental disomy in funding from Gilead, Sanofi, and Incyte and has consulted for myeloproliferative neoplasms. Epigenetic inactivation of suppressors of cytokine signalling in Philadelphia-chromo- some negative chronic myeloproliferative disorders. Jason Gotlib, MD, MS, Associate Professor of Medicine (Hematol- 18. The myeloprolifera- ogy), Stanford Cancer Institute, 875 Blake Wilbur Dr, Rm 2324, tive disorder associated JAK2 V617F mutant escapes negative Stanford, CA 94305-5821; Phone: 650-725-0744; Fax: 650-724- regulation by suppressor of cytokine signaling 3. JAK2V617F expression References in murine hematopoietic cells leads to MPD mimicking human 1.
Order v-gel 30 gm mastercard
Nine of these 11 trials noted a significant reduction in proteinuria with combination compared with monotherapy herbals shoppe hedgehog products safe 30 gm v-gel, but only 5 showed that effect as independent of blood pressure quest herbals purchase v-gel 30 gm fast delivery. Of the 5 trials using equivalent doses in mono and combo therapy herbals world buy v-gel uk, only 1 of the 5 showed that combination therapy was superior to either 86 monotherapy for reduction in proteinuria independent of blood pressure control. Of the 5 trials that compared half dose combination therapy to double that dose monotherapy, 3 of the 5 showed significant reduction in proteinuria with combination therapy that was independent of 84, 94, 104 blood pressure control. Of the 6 trials designed with all participants on monotherapy with ACE-I or AIIRA followed by the addition of the other type of agent compared with placebo, only 2 of the 6 showed a clear and significantly greater reduction in proteinuria for combination therapy 109, 110 compared with monotherapy. Further, in the trial by Kim and colleagues, subgroup analysis only showed significantly greater reduction in proteinuria with combination therapy among those with IgA nephropathy, and not among those with diabetic nephropathy. Similarly, another trial among these 6 also showed a significant reduction in 1 subgroup of chronic kidney disease patients (IgA nephropathy), but not in another included subgroup (diabetic 112 nephropathy). A fourth trial within this group showed a significantly greater reduction in proteinuria in combination therapy compared with monotherapy, but only with the highest dose of combination therapy (whereas a group with lower dose combination therapy did not reveal a 111 statistically significant decrease in proteinuria compared with monotherapy). In total, only 4 of 16 studies found a statistically significantly greater reduction in proteinuria among those on combination therapy with ACE-I and AIIRA compared with monotherapy with either agent that was independent of blood pressure management. These studies suggest do not provide consistent and convincing data regarding the reduction in proteinuria with combination compared with monotherapy with these agents. DRIs, AIIRAs, and ACE-Is Page 59 of 144 Final Report Drug Effectiveness Review Project Monotherapy with ACE-I and AIIRA compared with combination therapy Losartan Losartan in combination with lisinopril One trial (N=10) compared the effects of combination therapy using losartan and lisinopril to monotherapy with losartan or lisinopril on reduction in proteinuria and changes in creatinine 89 clearance. Participants were randomized to escalating doses of lisinopril or losartan in order to identify the optimal antiproteinuric dose for each participant. Participants were then crossed-over the alternate agent and the same process was repeated. After the optimal antiproteinuric dose of ACE-I and AIIRA was identified for each participant, all participants were placed on combination therapy of both agents at their optimal antiproteinuric dose. This trial showed a 51% reduction in proteinuria for those on losartan alone, a 69% reduction in proteinuria for those on lisinopril alone, and a 78% reduction in proteinuria for those on combination therapy at optimal antiproteinuric doses. Reduction in proteinuria with combination therapy was found to be significantly greater (P<0. Combination therapy was also noted to lower blood pressure significantly more than losartan monotherapy. Changes in creatinine clearance compared with baseline were not statistically significant for either monotherapy, but were statistically significantly lower among those on combination therapy (P<0. This trial reported 1 withdrawal, which was not related to adverse events. Two adverse events were reported for each therapy arm in this trial: the incidence of potassium levels greater than 5. Two participants experienced both elevated potassium and dizziness in the combination therapy group (20% event rate for each adverse event). Losartan monotherapy resulted in a 10% adverse event rate for each adverse event (meaning 1 participant for each), and lisinopril monotherapy resulted in a 20% event rate for hyperkalemia (2 participants) and a 10% event rate for dizziness (1 participant). None of these adverse events resulted in a withdrawal of therapy. Losartan in combination with enalapril Two trials compared the combination of losartan plus enalapril to monotherapy with either 93, 103 losartan or enalapril (N=105). Complete details of both of these trials are discussed previously and can also be seen in Evidence Table 9. Both trials compared monotherapy with losartan 25 mg per day or enalapril 10 mg per day to combination therapy with losartan 25 mg per day plus enalapril 10 mg per day. Despite significant similarities in design, these trials resulted in different outcomes. In the trial with shorter duration of follow-up (N=51), combination therapy resulted in a 66% reduction in proteinuria, as compared with a 25% reduction in proteinuria for 103 losartan monotherapy and a 45% reduction in proteinuria for enalapril monotherapy. Reduction in proteinuria was found to be statistically greater among those on combination therapy when compared with either monotherapy (P=0. No significant changes were found in creatinine clearance.
Fraser, 54 years: Combined results from 2 fair-quality randomized controlled trials of 1869 Japanese patients with stroke found a lower rate of both neutropenia (1% compared with 3%; relative risk, 0. In septic abortion, there may be foul- smelling discharge.
Tragak, 50 years: An understanding of the immunopathogenesis of HIV-1 infection is a major prerequisite for rationally improving therapeutic strategies, developing immunother- apeutics and prophylactic vaccines. Triptan compared with placebo: Characteristics and outcomes Results Author Year Country Number screened/ Trial Name eligible/ Number withdrawn/ (Quality Score) enrolled lost to fu/analyzed Relief at various times Carpay nr/nr/481 37(8.
Ateras, 51 years: Im m ediate R elease (ER vs IR ) O xybutyninER vs O xybutyninIR Versi M eanchangeinurgeincontinenceepisodes/wk: 2000 -15. Indications Addressed This review addresses the use of atypical antipsychotics to treat schizophrenia, bipolar disorder, major depressive disorder, behavioral and psychological symptoms of dementia in adults, and pervasive developmental disorders and disruptive behavior disorders in children.
Thorek, 36 years: M eanage48years 41% fem ale 78% white 6% black 16% other J asperson 30patientsinGerm anywhoseesophagitishealedafter6- AllGrade4(Savary-M iller) 36treated,6didnotheal,30included. Both placebo- and pramlintide-treated patients required increases in their total daily insulin doses during the 52 weeks (change in total daily dose from baseline for pramlintide compared with placebo: pramlintide: +8 to +11% vs.
Snorre, 44 years: This changes the conformation of the DPAF peptide and influences the antibody-epitope binding reaction. Comparison of the efficacy compared with warfarin at different levels of predicted international and safety of new oral anticoagulants with warfarin in patients with normalized ratio control for stroke prevention in atrial fibrillation.
Fabio, 60 years: We rated the internal validity of each trial based on the methods used for randomization, allocation concealment, and blinding; the similarity of compared groups at baseline; maintenance of comparable groups; adequate reporting of dropouts, attrition, crossover, adherence, and contamination; loss to follow-up; and the use of intention-to-treat analysis. The control group might receive a placebo, a different treatment for the disease, or no treatment at all.
Osko, 43 years: Disodium Crom ogly cate Germ any P atientswith lessthan one AE18vs. Nevirapine, rilpivirine and etravirine are not recommended in combination with rifamycins.
Ben, 58 years: Antiemetics Page 339 of 492 Final Report Update 1 Drug Effectiveness Review Project Evidence Table 9. Johanson JF, Gargano MA, Holland PC, Patchen ML, Ueno R.
Kurt, 45 years: Fedratinib (SAR302503), an Histone deacetylase (HDAC) inhibitors (givinostat) are also a inhibitor of JAK2V617F, FLT3, and RET, was removed from rational MPN therapy considering that HDAC modulates several clinical trials in November 2013 as a result of neurological complica- genes involved in cell cycle regulation, hematopoiesis, prolifera- tions including Wernicke’s encephalopathy. The impor- tance of a sustained virological treatment success for clinical benefit has also been reported from other cohorts (Thiebaud 2000, Lohse 2006).
Navaras, 28 years: Genotypic drug resistance and long-term mortality in patients with triple-class antiretroviral drug failure. Thus, dendritic cells may serve as scouts in the peripheral tissue, bringing exogenous antigen to lymph nodes when stimulated by signs of infection or tissue damage.
Gonzales, 26 years: Atazanavir is a component of the following: • Reyataz capsules, 150 mg, 200 mg, 300 mg • Reyataz oral powder for oral suspension, 50 mg packet • Evotaz film-coated tablets, 300 mg plus 150 mg cobicistat Dosage: 300 mg atazanavir QD combined with 100 mg ritonavir (instead of riton- avir, cobicistat may also be used as a booster). Published online ahead of print May 30, meeting abstract].
Wenzel, 35 years: Diabetes Mellitus Twenty-two observational studies evaluated the association of atypical antipsychotics with 187, 215, 335, 547, 550, 575, 584, 585, 588, 590, 596, 600, 603, 606, 614-621 development of new-onset diabetes mellitus. Treatment of tuberculosis: an intra-ovarian environment that is not conducive Guidelines, 4th edn.
8 of 10 - Review by J. Narkam
Votes: 180 votes
Total customer reviews: 180
References
- Malthaner RA, Wong RK, Rumble RB, et al: Neoadjuvant or adjuvant therapy for resectable esophageal cancer: A systematic review and meta-analysis. BMC Med 2:35, 2004.
- Erickson BA, Lu X, Vaughan-Sarrazin M, et al: Initial treatment of men with newly diagnosed lower urinary tract dysfunction in the Veterans Health Administration, Urology 83:304n311, 2014.
- Spencer SS. Corpus callosum section and other disconnection procedures for medically intractable epilepsy. Epilepsia 1988; 29(Suppl. 2):S85.
- Rossanese M, Novara G, Challacombe B, et al: Critical analysis of phase II and III randomised control trials (RCTs) evaluating efficacy and tolerability of a-3-adrenoceptor agonist (Mirabegron) for overactive bladder (OAB), BJU Int 115(1):32n40, 2015.
- Slaton JW, Kropp KA: Conservative management of suspected bladder rupture after augmentation enterocystoplasty, J Urol 152(2 Pt 2):713n715, 1994.
- Hadziselimovic F, Herzog B, Hocht B, et al: Screening for cryptorchid boys risking sterility and results of long-term buserelin treatment after successful orchiopexy, Eur J Pediatr 146(Suppl 2):S59nS62, 1987. Hadziselimovic F, Huff D, Duckett J, et al: Long-term effect of luteinizing hormone-releasing hormone analogue (buserelin) on cryptorchid testes, J Urol 138(4 Pt 2):1043n1045, 1987. Hadziselimovic F, Huff D, Duckett J, et al: Treatment of cryptorchidism with low doses of buserelin over a 6-months period, Eur J Pediatr 146(Suppl 2):S56nS58, 1987. Hadziselimovic F, Hocht B, Herzog B, et al: Infertility in cryptorchidism is linked to the stage of germ cell development at orchidopexy, Horm Res 68(1):46n52, 2007.
- Hamada Y, Kawachi K, Nakata T, et al: Antiinflammatory effect of heparin-coated circuits with leukocyte-depleting filters in coronary bypass surgery, Artif Organs 25:1004, 2001.