Eduardo Castro, M.D.
- Instructor in Medicine
- Harvard Medical School
- Massachusetts General Hospital
- Boston, MA
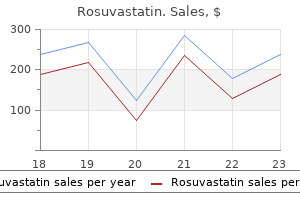
Rosuvastatin dosages: 10 mg
Rosuvastatin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Rosuvastatin 10 mg order overnight delivery
An 99m 201 exception is the improved specificity in women using Tc-sestamibi compared with Tl cholesterol milk rosuvastatin 10 mg purchase without prescription. Studies often include participants who may not fully represent those most challenged by 99m imaging cholesterol medication while pregnant purchase rosuvastatin 10 mg on line. The Tc-based agents xanthogranuloma cholesterol buy rosuvastatin 10 mg fast delivery, with their greater photon energy, would be expected to offer improved performance in obese patients and those with large breasts, as well as allowing the option of higher- quality gated images. In practice, use of contemporary quantitative programs can improve image acquisition quality as well as interpretation. Some programs incorporate motion-sensing algorithms that interrogate the raw data and alert the technologist that motion correction may be needed. Selected short- and long-axis tomograms from stress and rest studies (two left columns) are automatically segmented and scored. Such improvement has not been demonstrated, however, possibly because of the “roll-off” property of the 4 common perfusion tracers, caused by diffusion limitation at hyperemic blood flow levels (see Fig. Thus the more favorable hyperemic stress achieved with pharmacologic stress is offset by the lack of linear tracer uptake in the areas with the highest flow. However, because maximal coronary flow reserve is not achieved as often as with vasodilator pharmacologic stress, and side effects are substantial, dobutamine is recommended only when adenosine, dipyridamole, or regadenoson is contraindicated, such as in a patient with important reactive airways disease. However, the extent and severity of reversible perfusion defects may be diminished at submaximal versus maximal workloads, which may affect the prognostic value of the test. Exercise is the preferred stressor because it allows the optimal potential association of symptoms with perfusion abnormalities. For patients who cannot exercise adequately, vasodilator stress with adenosine, dipyridamole, or regadenoson is the procedure of choice; dobutamine is used for patients 24 with a contraindication to the vasodilators. For patients who begin exercise but do not reach 85% of maximum predicted heart rate for age, or who do not reach an appropriate symptomatic endpoint, isotope injection at stress can be withheld, the exercise portion of the test terminated, and vasodilator stress performed to optimize diagnostic and risk stratification information. However, incorporation of other findings, including regional functional abnormalities, can be used to estimate more correctly the probability of disease extent. Clinical questions may remain after angiography regarding the “physiologic significance” of stenotic lesions. Current guidelines suggest aggressive risk factor 31 reduction therapy in those at high clinical risk for the development of vascular disease. Relationship between stress-induced myocardial ischemia and atherosclerosis measured by coronary calcium tomography. Relationship between noninvasive coronary angiography with multi-slice computed tomography and myocardial perfusion imaging. Thus, information from the two testing modalities may be complementary in refining the risk assessment of future coronary events, thereby curtailing the aggressiveness of primary prevention. Moreover, in a coronary segment that is heavily calcified, stenoses are particularly difficult to detect, to rule out, or to quantitate. After an average of approximately 2 years of follow-up, there was essentially no difference in the primary endpoint outcome composite, suggesting that the initial assessment strategies were associated with similar outcomes. A severe inferolateral resting perfusion defect (arrow, all images) suggests ischemia at rest or infarction in that territory. Upper left, Normal study findings, associated with a low risk of cardiac events during follow-up, suggesting that such a patient can be managed conservatively without catheterization but with aggressive secondary preventive strategies. Despite the stabilization of symptoms, extensive reversible perfusion abnormalities in the inferior and lateral walls suggest high risk of cardiac death or myocardial infarction, or both, during follow-up. This patient would therefore be managed more aggressively with catheterization and intervention. Contemporary guidelines suggest that noninvasive assessment of the presence and extent of inducible ischemia is indicated (class I recommendation) for patients who have not already had coronary angiography and do not have other high-risk features that would drive a decision to perform 45 angiography. Besides the fixed defect representing the infarct in the anterior wall and apex (arrowheads), extensive inducible ischemia is evident both within and remote from the infarct territory (septum and inferior walls, arrows), involving 25% of the ventricle. Role of adenosine thallium-201 tomography for defining long term risk in patients after acute myocardial infarction. As noted earlier, after a regional ischemic insult, abnormalities in fatty acid metabolism may persist long after perfusion has returned to normal, a finding termed ischemic memory. Imaging of fatty acid metabolism may therefore allow assessment of recent ischemia. Future studies will determine whether such techniques can help guide management decisions.
Order rosuvastatin 10 mg mastercard
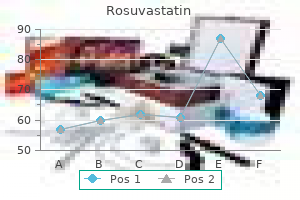
Reporting guidelines also outline the elements of a comprehensive reporting structure when 7 semiquantitative and/or quantitative analysis are used cholesterol levels non fasting rosuvastatin 10 mg purchase fast delivery. Bayes theorem posits that the post-test probability of disease (or risk of an event after a test) is influenced not only by the sensitivity and specificity of the test cholesterol test new zealand buy rosuvastatin 10 mg amex, but also by the pretest probability of disease (see Chapter 13) cholesterol zelftest buy generic rosuvastatin pills. For a given positive test result, the post-test probability of disease may be distinctly lower in a patient with a very low pretest probability of disease compared with a different patient with a much higher pretest probability (eFig. A, For patient with low pretest probability of disease (point A at 15% on x axis) with a positive test result, post-test probability of disease (point A at 50% on y axis) is lower than for a different patient with a higher pretest probability with the same positive test result (point B at 50% pretest probability on x axis, 90% post-test probability on y axis). In B, the “test positive” curve can be thought of as a family of curves influenced by how strongly positive the images can be. For a given pretest probability, the post-test probability becomes progressively higher as the image becomes more strongly abnormal. For a borderline abnormal study (+ curve), the post-test probability may be only slightly higher than the pretest value. For a strongly positive study (+++ curve), the post-test probability is very high no matter what the pretest probability. If reported as positive, there is actually a greater chance that such a result represents a false-positive result (70%) as opposed to a true-positive result (30%). Although this defect may represent a small area of inferior inducible ischemia, the image also may reflect diaphragm attenuation of the inferobasal wall predominantly affecting the stress image. A result reported as positive is more likely to represent a false-positive than a true-positive finding. Lung Uptake In some patients, substantial tracer uptake is apparent throughout the lung fields after stress that is not present at rest (Fig. It is likely that ischemia-induced elevation in left atrial and pulmonary pressures slows pulmonary transit of the tracer, allowing more time for extraction or transudation into the interstitial spaces of the lung, accounting for this imaging sign. Splanchnic or background activity is minimal after thallium stress injection, allowing image acquisition earlier after stress. In addition, the redistribution properties of thallium mandate that imaging begin relatively early after stress, so lung uptake may be more apparent. For patients in whom the entire left ventricle appears larger during stress, the pathophysiology probably is related to extensive ischemia and prolonged postischemic systolic dysfunction, resulting in a dilated, dysfunctional left ventricle during the stress acquisition relative to the rest acquisition. Contemporary processing systems can automatically quantify transient ischemic dilation. These perturbations from a completely homogeneous tracer pattern throughout the myocardium are related to structural variations of the myocardium as well as to technical factors associated with image acquisition. One example is the “dropout” of the upper septum secondary to merging of the muscular septum with the membranous septum (Fig. Apical thinning is another variation of normal that can be mistaken for a perfusion defect (Fig. The apex is anatomically thinner than other myocardial regions, creating this appearance. This difference is not caused by a disparity in lateral versus septal wall myocardial blood flow. A, Normal “dropout” of the basal septum (arrows), which would be seen in the most basal short-axis tomograms. C, The lateral wall often is slightly “hotter” than the septum, another normal variation. This refers to undetected events in the heart caused by interaction of photons with the intervening soft tissue, breast, or diaphragm. In patients with large or dense breasts, significant attenuation may create artifacts varying considerably in their appearance and location (Fig. A review of the cine display of the raw projection images 5 may reveal the presence of potential breast attenuation. The availability of gender-matched quantitative databases has had a favorable although modest impact on this issue, because such databases generally consist of individuals of average body and breast size. There was a suggestion of breast shadowing on review of the raw cine images (not shown). Thus this defect may represent either a nontransmural anterior infarct or an artifact consistent with breast attenuation.
Syndromes
- Staying at a healthy weight
- Ultrasound of the abdomen (may show gallstones)
- Pain with bowel movements
- History and physical
- Over-the-counter analgesics or prescription pain medications to control pain (neuralgia)
- Shortness of breath
- Chills and shaking
- Persistent cough
10 mg rosuvastatin
Adapt this dietary pattern to appropriate calorie requirements cholesterol levels good generic rosuvastatin 10 mg with amex, personal and cultural food preferences cholesterol pill green buy rosuvastatin 10 mg with visa, and nutrition therapy for other medical conditions (including diabetes mellitus) cholesterol lowering foods beans buy line rosuvastatin. Cigarette Smoking The effect of cigarette smoking on hypertension and outcomes in hypertensive patients remains difficult to 47 define because of confounding by increases in waist girth with smoking cessation. Each cigarette evokes a transient pressor response that dissipates over the next hour. Barriers to Adoption and Maintenance of Lifestyle Change and Possible Solutions In practice, encouraging sustainable lifestyle change has proved extremely difficult. Substantial recent efforts have explored strategies and tools for encouraging the adoption of healthier lifestyles, including weight control, diet, and physical activity. Some challenges to lifestyle change identified in the literature will resonate with practitioners. Individuals often express a low desire for, interest in, or awareness of dietary change, including weight loss, decreased sodium intake, smoking cessation, or reduced alcohol consumption. Barriers to adoption of physical activity recommendations include comorbid conditions that 48 limit physical activity, as well as limited time. Contemporary adjuncts to the usual medical model for lifestyle intervention include Internet-based interventions, which are currently under intense 40,49-51 evaluation. Antihypertensive Drugs Although all hypertensive individuals should heed the lifestyle measures previously outlined, most also will require drug therapy to optimize outcomes. Advantages of amlodipine include predictable dose-dependent potency, once- daily dosing because of its long half-life, tolerability, and cost (≤$10 per month for generic amlodipine). These drugs have some diuretic action (due to dilation of the afferent renal arteriole), which may reduce requirements for additional diuretic therapy for mild hypertension. Verapamil is weakly antihypertensive and has limited usefulness because of dose-dependent constipation. Diltiazem is intermediate in potency between verapamil and the dihydropyridines and is usually well tolerated. Side Effects The principal side effect of the dihydropyridines is dose-dependent ankle edema. Verapamil and diltiazem can impair cardiac conduction, especially in older patients also receiving digoxin, beta blockers, or central sympatholytic agents. There is no compelling indication to prescribe the direct renin inhibitor aliskiren. High levels of circulating prorenin may stimulate A I receptor– independent signaling pathways, which are both potentially beneficial and potentially harmful (see Fig. Diuretics for Hypertension Diuretics are among the oldest and most effective antihypertensive medications. With continued therapy, blood volume is partially restored, and vasodilator mechanisms (e. Thiazide and thiazide- + − like diuretics (chlorthalidone, indapamide) block the Na -Cl cotransporter in the distal convoluted tubule. Efficacy of low-dose chlorthalidone and hydrochlorothiazide as assessed by 24-h ambulatory blood pressure monitoring. Such low-dose combinations should also reduce dose-dependent diuretic side effects, a conjecture as yet not substantiated in formal dose-finding studies. Side Effects Thiazide-type diuretics can aggravate glucose intolerance (particularly in higher doses and when used in combination with a standard beta blocker), cause hypokalemia and hypomagnesemia and hyponatremia 72 (see later), precipitate gout, and elevate serum lipids with increased hepatic triglyceride content; they can also cause photosensitive dermatitis. They may be more likely than other antihypertensive drugs to 73 cause erectile dysfunction but evidence is limited. Thiazide-type diuretics are the most common cause of 74,75 severe hyponatremia, especially in older women (Fig. Although less well recognized than thiazide-induced hypokalemia, thiazide-induced hyponatremia is a common reason why some elderly hypertensive individuals simply cannot tolerate even low-dose thiazides. A total of 1033 cases of hyponatremia (serum sodium <130 mmol/L) from the Dutch Integrated Primary Care Information database between 1996 and 2011. This study provides new evidence for an old idea: “The Miracle of Low-Dose Spironolactone” [for resistant hypertension]—the title of a 1972 “clinical pearls” article penned by the late Dr.
Order rosuvastatin from india
The persistence for at least 12 weeks of one of the following antiphospholipid antibodies is required: IgG or IgM anticardiolipin antibodies cholesterol profile definition 10 mg rosuvastatin with mastercard, anti-beta2-glycoprotein I cholesterol levels in fertilized eggs generic rosuvastatin 10 mg overnight delivery, antiprothrombin cholesterol test at walgreens buy rosuvastatin 10 mg visa, or lupus anticoagulant. Presence of the antiphospholipid syndrome means heightened susceptibility to recurrent venous or arterial thrombosis if anticoagulation is 53 discontinued. Obtaining a family history remains the fastest and most cost-effective method of identifying a predisposition to venous thrombosis. Investigation with blood tests to detect known causes of hypercoagulability can be misleading. Consumption coagulopathy caused by venous thrombosis, for example, may be misdiagnosed as deficiency of antithrombin, protein C, or protein S. The most useful approach is a clinical assessment of likelihood, based on presenting symptoms and signs, in conjunction with judicious diagnostic testing. Although the traditional upper limit of normal for a D-dimer screening test is 500 ng/mL, the upper limit of normal should be increased for patients older than 50 years. For these older patients, the 55 age-adjusted D-dimer cutoff level is defined as age multiplied by 10. Dyspnea is the most frequent symptom, and tachypnea is the most frequent sign (Table 84. Paradoxically, severe pleuritic pain often signifies that the embolism is small, not life-threatening, and located in the distal pulmonary arterial system, near the pleural lining. He was hemodynamically stable, with normal right ventricular function on echocardiography. This test generally is not useful for screening acutely ill hospitalized inpatients, because they usually have elevated D-dimer levels. The most famous sign of right heart strain is S Q T , but I have found that the most1 3 3 common sign is T wave inversion in leads V to V. A peripheral wedge-shaped density above the diaphragm (Hampton hump) usually indicates pulmonary infarction (see Fig. Lung Scanning Pulmonary radionuclide perfusion scintigraphy (lung scanning) uses radiolabeled aggregates of albumin or microspheres that lodge in the pulmonary microvasculature. Thus, a clinical probability assessment helps in correct interpretation of the scan results. Three-dimensional images can be reconstructed, and color can be added electronically to enhance details of thrombus localization. These diseases include pneumonia, atelectasis, pneumothorax, and pleural effusion, which may not be well visualized on the chest radiograph. Normally, the ratio of the diameters of the right ventricle and the left ventricle is less than 0. Moderate or severe right ventricular hypokinesis, persistent pulmonary hypertension, patent foramen ovale, and free-floating thrombus in the right atrium or right ventricle are associated with 60 a high risk of death or recurrent thromboembolism. Normally, the vein collapses completely when gentle pressure is applied to the skin overlying it. Use of this modality is routine, however, to plan interventions such as pharmacomechanical catheter–assisted therapy. Chronic thrombus leads to bandlike defects called webs, in addition to intimal irregularities and abrupt narrowing or occlusion of lobar vessels. Too little attention is paid to history taking, physical examination, clinical likelihood scoring systems, and D-dimer screening. Undue reliance on advanced imaging technology has adverse consequences aside from the increased cost, including unnecessary exposure to radiation and intravenous contrast agents, with potential complications of renal dysfunction or anaphylaxis. Low-risk patients have an excellent prognosis with anticoagulation alone (see also Chapter 93). High-risk patients may require intensive hemodynamic and 63 respiratory support with pressors, mechanical ventilation, or extracorporeal membrane oxygenation. In 64 addition to anticoagulation, advanced management options include systemic thrombolysis, 65 pharmacomechanical catheter–assisted therapy, vena cava filter placement, or surgical embolectomy (Fig. The three key components for risk stratification are (1) clinical evaluation, (2) assessment of right ventricular size and function, and (3) analysis of cardiac biomarkers to determine whether there is right ventricular microinfarction.
Order 10 mg rosuvastatin otc
A cholesterol numbers chart explained buy discount rosuvastatin 10 mg, Parasternal long-axis view showing deep prolapse of the posterior mitral leaflet cholesterol levels ldl hdl ratio generic 10 mg rosuvastatin visa. A cholesterol levels u.k rosuvastatin 10 mg order with visa, Parasternal long-axis view showing severe flail of the posterior mitral leaflet. A, Apical long-axis view showing a large posterior myocardial infarction, which is tethering the posterior leaflet preventing the anterior leaflet from closing. The severity of the regurgitation is reflected in the width of the jet across the valve and the size of the left atrium. Quantitative methods to measure regurgitant fraction, regurgitant volume, and regurgitant orifice area 70 have greater accuracy when done carefully (Fig. Comparison of early surgery versus conventional treatment in asymptomatic severe mitral regurgitation. Unfortunately, each of these stroke volumes requires multiple measurements, with any error propagating throughout the calculation, compounded at the end by needing to subtract one large number from another. It exploits the predictable flow acceleration leading into the mitral valve, which forms roughly hemispheric isovelocity shells that can be highlighted by shifting the aliasing velocity of the color display and identified where the color changes from blue to red (see Fig. A simplification that works in the majority of cases assumes approximately 100 mm Hg of driving pressure across the regurgitant orifice (with Bernoulli equation, leading to a 5-m/sec Vmax). Calculation of mitral regurgitant orifice area with use of a simplified proximal convergence method: initial clinical application. Thus the regurgitation is much less severe than a single frame showing the largest jet, vena contracta, or convergence zone would imply. In interrogating the mitral valve, it is important to localize the origin and direction of the regurgitant jet. The parasternal and apical long-axis views identify pathology of the posterior versus anterior leaflet and jet direction, whereas the often-neglected parasternal short-axis and apical two-chamber views can show where along the commissural closure line the dominant jet originates (Fig. The parasternal short-axis view (left) and apical two-chamber view (right) both allow this delineation. Localizing the proximal convergence zone in these views can be particularly helpful in assessing the mechanism. Multiplane imaging allows structured interrogation of the valve for optimally localizing the pathology. When ordering a treadmill exercise echocardiogram, the physician should provide guidance to the sonographer as to the priority for the various datasets to be obtained after exercise, because it is often impossible to obtain diagnostic mitral and tricuspid imaging as well as wall motion assessment while heart rate is still optimally high. If the exercise is on a supine bicycle, comprehensive imaging can be obtained of all relevant parameters. The lesion is best visualized on chest films exposed in the lateral or right anterior oblique projections (see eFig. Chronic mitral regurgitation and aortic regurgitation: have indications for surgery changed? Natural history of the asymptomatic patient with severe mitral regurgitation secondary to mitral valve prolapse and normal right and left ventricular performance. Outcomes in mitral regurgitation due to flail leaflets: a multicenter European study. Comparison of early surgery versus conventional treatment in asymptomatic severe mitral regurgitation. However, a 5-year survival of only 30% was reported in patients who were candidates for operation, presumably because of symptoms, but who declined surgery (see eFig. The medically treated group either never underwent surgery or underwent surgery at a later date. Association between early surgical intervention vs watchful waiting and outcomes for mitral regurgitation due to flail mitral valve leaflets. Long- term mortality associated with left ventricular dysfunction in mitral regurgitation due to flail leaflets: a multicenter analysis. However, in 127 propensity score-matched patients in that study, the estimated actuarial 7-year survival was 99% ±1% in those treated with early surgery, compared with only 85% ±4% for those treated according to current guidelines for watchful waiting. These considerations have prompted recommendations for earlier surgery in 21,37,61,89,92,95 patients who are candidates for repair, especially in the setting of flail leaflets. Late outcomes of mitral valve repair for mitral regurgitation due to degenerative disease. However, in the absence of definitive clinical trials, such therapy is not currently recommended. In selected cases, right-heart catheterization and left ventriculography may be helpful resolving discrepancies between echocardiographic findings and the clinical picture, as well as detecting and assessing the severity of other associated valvular lesions.
Buy rosuvastatin master card
Even in patients with syncope during exertion xeljanz cholesterol order rosuvastatin 10 mg on-line, exercise stress testing is highly unlikely to trigger another event cholesterol egg white rosuvastatin 10 mg purchase fast delivery. Coronary angiography is recommended in patients with syncope suspected to result my cholesterol ratio is 2.3 purchase cheap rosuvastatin on line, directly or indirectly, from myocardial ischemia. Despite the low diagnostic yield of electrocardiography, the test is inexpensive and risk free and is 1 considered a standard part of the evaluation of virtually all patients with syncope. However, because of the infrequent and sporadic nature of syncope, the diagnostic yield of Holter monitoring in the evaluation of patients with syncope and presyncope is extremely low. Holter monitoring and inpatient telemetry monitoring are most likely to be diagnostic when used for the occasional patient with frequent (i. Continuous-loop event monitors, often programmed with 5 to 15 minutes of preactivation memory stored by the device, are preferred because the data can be retrieved for analysis. Prospective event monitors not worn continuously by the patient are of value to investigate palpitations but play no role in the evaluation of patients with syncope. Event monitors are indicated in the early phase of the evaluation of patients with syncope of uncertain origin who do not have high-risk criteria that require immediate hospitalization or intensive evaluation. They are also indicated in high-risk patients in whom a 1,2 comprehensive evaluation did not demonstrate a cause of the syncope or lead to specific treatment. These devices result in higher diagnostic yield in patients with syncope or presyncope than do the conventional event monitors just described. These devices allow a longer monitoring period (12 to 36 months) and have higher diagnostic yield, but they have the disadvantages of requiring surgical implantation and increased cost. A recent advancement in this technology is that these implantable event 29 monitors can be accessed by remote monitoring, which further increases their diagnostic effectiveness. Implantable loop recorders with a battery life of 2 to 3 years have also been shown to improve the 19 diagnostic yield in patients with syncope. However, a recent Cochrane meta-analysis showed no impact 19 of implantable loop recorders on mortality. In addition, programmed electrical stimulation using standard techniques should be performed to evaluate the inducibility of ventricular and supraventricular arrhythmias. It is also common practice to limit the shortest coupling interval to 200 milliseconds. The patient often regains consciousness despite continuation of the arrhythmia as a result of activation of a compensatory mechanism. Test to Screen for Neurologic Causes of Syncope Syncope as an isolated symptom rarely has a neurologic cause. As a result, widespread use of tests to 1,2 screen for neurologic conditions is rarely diagnostic. A diagnosis is almost never uncovered that was not first suspected on the basis of a careful history and neurologic examination. No studies have suggested that carotid Doppler ultrasonography is beneficial in patients with syncope. Although the low diagnostic yield of screening “neurologic tests” has been recognized for more than a decade, they continue to be overused and result in a dramatic increase in costs. Patients with syncope can be further divided into two groups: those in whom a certain diagnosis has been established and in whom treatment can be initiated and those with an uncertain diagnosis. For the latter, attention should focus on determining whether the patient is at increased risk for a cardiovascular event or death. Conversely, patients who have experienced only a single episode of syncope and are determined to be at low risk for a cardiovascular event or death may require no further evaluation. Patients who fall between these two extremes can undergo further testing based on results of the initial evaluation (see Fig. When this diagnostic approach has been completed, a probable cause of syncope can be determined in more than three fourths of patients. Other studies have reported favorable outcomes when a syncope evaluation unit or standardized approach to the 22,23 evaluation of syncope is used. Management of Patients With Syncope Treatment of a patient with syncope has three goals: (1) prolong survival, (2) prevent traumatic injuries, and (3) prevent recurrences of syncope. The approach to treatment of a patient with syncope depends largely on the cause and mechanism of the syncope. However, a patient with syncope secondary to heart block in the setting of an inferior wall myocardial infarction will not usually require a permanent pacemaker because the heart block usually resolves spontaneously. Similarly, heart block resulting from neurally mediated syncope does not generally require pacemaker implantation.
Wild Oat (Oats). Rosuvastatin.
- Dosing considerations for Oats.
- Reducing blood sugar levels in people with diabetes when oat bran is used in the diet.
- What other names is Oats known by?
- Lowering cholesterol. Consuming oat products such as oatmeal and oat bran when used as part of a diet low in fat and cholesterol can significantly lower cholesterol levels.
- How does Oats work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96791
Order rosuvastatin 10 mg
This effort is driven by both the need to avoid excessive false-positive test results and the need to contain the costs of medical care kind of cholesterol in eggs order rosuvastatin line. The goal of appropriate-use guidelines is to reduce overuse errors and maximize the value of diagnostic testing and procedures source of cholesterol in eggs buy cheap rosuvastatin online. The general principle of any test- ordering strategy is that a plausible hypothesis (a provisional diagnosis) should be formulated first cholesterol test nz cheap rosuvastatin, followed by testing. The appropriate-use criteria are designed to avoid testing when the results are unlikely to improve patient care or outcomes. These guideline recommendations emphasize the need to consider categories based on estimates of risk and prognosis, rather than diagnostic labels. Risk is another word for probability, and when used in this context, risk takes on a meaning of propensity, which is probability that has a modifiable tendency or disposition. It is important for clinicians to understand how risk is calculated from long-term observations from pooled cohorts of test subjects, in order to understand the strengths and limitations of these risk calculations. After calculating the risk, the challenge for clinicians is communicating risk to patients in an understandable way. Investigators have provided pictograms that can communicate risk and risk reduction to facilitate a discussion regarding long-term treatment options to diminish risk and to compare the degree of risk reduction with potential side effects and costs of treatment. Since clinicians vary in their use of qualitative terms, such as “high risk,” there is a need to provide clear and understandable quantitative estimates. Therapeutic Decisions A preventive or therapeutic decision is a structured choice. For some situations, it is a simple and easy decision, such as deciding to give a diuretic to a patient with acute congestive heart failure. In this case the stakes are not high, the preference of the patient is clear, and the decision is straightforward. An elderly patient with moderate to severe mitral regurgitation and comorbid conditions presents a difficult choice based on estimated probabilities of the natural history of the disorder, versus the surgical risks and prospects for an improved outcome with a surgical intervention. Of note, the relative benefit (or risk) of an intervention is often expressed as a relative risk or odds ratio. Risk is the probability of an event, and odds is the probability an event will occur against the probability that it will not occur. The risk ratio expresses the relative probability that an event will occur when two groups are compared. The odds ratio expresses the odds of the event in one group compared with another. Despite its widespread use, the odds ratio is less helpful than relative risk in clinical decision making. The expressions are similar when baseline event rates are low (<5%), but deviate with higher risk and larger treatment effects. The odds ratio can express associations but, unlike the risk ratio, cannot express the relative size of the treatment effect; if clinicians assume odds to be equivalent to risk, it may lead to overestimates of the treatment effect when the outcome is common. The odds ratio is often used in clinical research because of its mathematical properties and its utility for identifying associations in certain situations, but clinicians need to know its limitations for estimates of treatment effect. Clinical trials report the average risk of an outcome for patients in a treatment group and in a comparison group. There may be heterogeneity of the treatment effect, in which some patients may receive a marked benefit and others receive no benefit at all. Subgroup analysis and tests for interaction can provide hints, but usually heterogeneity of treatment effect is not readily apparent, creating a challenge for clinicians trying to personalize treatment decisions. The challenge is that subgroup analyses introduce the possibility that associations have occurred only by chance. Thus, subgroup analyses are capable of 24 producing important insights, but must be interpreted with caution. Risk Stratification A weakness of relative benefit estimates is that they do not convey information about what is achieved for patients at varying levels of risk. A small relative reduction in risk may be meaningful for a high-risk patient, whereas a large relative reduction may be inconsequential for a very-low-risk patient. Absolute risk reduction, the difference between two rates, varies with the risk of an individual patient. In one case, the absolute difference is 50% (5000 per 10,000), and in the other, 0. In one case, 1 person out of 2 benefits, and in the other, 1 out of 2000 benefits.
Purchase 10 mg rosuvastatin visa
These views are often reinforced in the current health care environment cholesterol food chart pdf order rosuvastatin 10 mg with amex, in which quality measurement and reporting are often placed in a “regulatory” context and are often executed separately from clinician-patient interactions and clinical decision-making cholesterol lowering foods in gujarati discount 10 mg rosuvastatin with amex. The interaction of patients and clinicians is central to high-quality care cholesterol test online order rosuvastatin now, given the impact of clinical decisions (e. Indeed, there are several reasons why cardiovascular providers should engage in quality-of-care measurement and improvement. First, quality of care reflects the degree to which clinicians practice evidence-based medicine. Inherent in evidence-based medicine is consideration of both the best available scientific evidence and individual patient factors and preferences. Optimally, informed patients, who understand the state of their health and the potential risks and benefits of health interventions ranging from prevention to acute and chronic disease management, interact with clinicians who observe the tenets of evidence-based medicine. The outcomes of health decisions by patients and cardiovascular clinicians depend on the environment in which these decisions are made. From the perspective of cardiovascular clinicians, quality of care includes not only their actions, but also patient access, engagement, and behavior; the context and methods of health care delivery; and multiple aspects of the health care system, ranging from information technology and ancillary personnel support to health system policy and incentives. Ultimately, although essential, clinical knowledge and skill are not sufficient for ensuring high-quality health care; another primary driver is the health care delivery system. The concept of professionalism includes not only good clinical knowledge but also excellence in the delivery of health care and accountability for that care. Moreover, quality of care is increasingly tied to certification and licensure, particularly regarding involvement in practice improvement. Medical education is evolving to a model of lifelong learning, in which the principles of quality of care are integrated with clinical knowledge and decision making. Intrinsic to this new framework, cardiovascular clinicians will need to have the skills of quality-of-care measurement and improvement in addition to medical knowledge. Lastly, major changes in the health care environment bring quality of care to the center of clinical practice. Performance-based reimbursement and public reporting of quality-of-care measures are increasingly prevalent, along with new health care delivery and reimbursement models, such as accountable care organizations. Importantly, reimbursement for medical care is transitioning from payment for quantity to payment for quality, also known as “value-based purchasing” of health services. Measuring Health Care Quality and Uses of Quality Measurements This section describes types of quality measures, uses of measures, common data sources for quality measurement, and limitations of quality measures, including the potential for unintended consequences. Types of Quality Measures Fifty years ago, Avedis Donabedian articulated an enduring conceptual framework for measuring health care quality: characterizing quality according to structure, process, and outcome (see Classic References). While contemporary measurement extends beyond these domains, the Donabedian model remains central to understanding the quality of health care. Structural measures are specific attributes of the health care delivery system that are considered surrogates for the care delivered; examples include procedural volume and accreditation status. In general, such measures are only weak surrogates and are frequently inadequate if more robust metrics of 9,10 quality are available. Process measures reflect the actions of clinicians, such as prescribing medication, and are among the most commonly employed metrics of quality. Operationally, process measures are generally selected from among the care processes with strong support in practice guidelines (e. Not all strong guideline recommendations are appropriate for adoption as quality measures, but such measures should possess additional attributes that support their use for quality measurement (Table 4. However, they generally typically require clinical data, thus requiring resources for data abstraction. The exclusion of individual patients from a process measure “denominator” because of contraindications to treatment is viewed favorably by clinicians but is controversial. Such exclusions further increase the burden of data collection but enhance the clinical validity of these measures. Moreover, there is not always a demonstrated association between 12 higher performance on process measures and better patient outcomes.
10 mg rosuvastatin fast delivery
The site of block may not distinguish symptomatic children who have congenital or surgically induced complete heart block from those without symptoms cooking cholesterol lowering foods quality rosuvastatin 10 mg. In type I second-degree A1 V block cholesterol in shrimp cocktail purchase rosuvastatin 10 mg on line, the heart rate may increase imperceptibly with gradually diminishing intensity of S ; widening of the 1 a to c interval cholesterol score of 6 10 mg rosuvastatin purchase mastercard, terminated by a pause; and an a wave not followed by a v wave. Ambulatory monitoring (Holter or external loop recorders) can be useful, but monitoring for longer periods may be necessary, with extended (>3 weeks) Holter or external loop recorders being required. Longer periods of recording require an implantable loop recorder to establish the diagnosis. Drugs cannot be relied on to increase the heart rate for more than several hours to several days in patients with symptomatic heart block without producing significant side effects. Therefore, temporary or permanent pacemaker insertion is indicated for patients with symptomatic bradyarrhythmias. Slowing of the dominant pacemaker of the heart (usually the sinus node), which allows escape of a subsidiary or latent pacemaker. Acceleration of a latent pacemaker, for example, a tachycardia in which the atria are not required and that usurps control of the ventricles. Top, This tachycardia occurs at a fairly regular interval (W-shaped complexes) and is interrupted intermittently with sinus captures that produce functional right and left bundle branch blocks. The junctional discharge rate is approximately 120 beats/min (cycle length = 500 msec), and the rhythm is irregular, sometimes shortened by sinus captures or delayed by concealed conduction that resets and displaces the junctional focus. Bottom, Carotid sinus massage slows both the junctional and the sinus discharge rates. If a single pacemaker establishes control of both the atria and the ventricles for one beat (capture) or a series of beats (e. P wave morphology depends on the rhythm controlling the atria—sinus, atrial tachycardia, junctional, flutter, or fibrillation. Intermittent large (cannon) a waves may be seen in the jugular venous pulse when atrial and ventricular contractions occur simultaneously. The second heart sound can split normally or paradoxically, depending on the manner of ventricular activation. A premature beat representing ventricular capture can interrupt a regular heart rhythm. Management Management is directed toward the underlying heart disease and precipitating cause. An applied stimulus produces an electrical field that is proportional to the spatial derivative of the applied voltage (local change in voltage with respect to distance). The response of the heart is mediated by the passive and active (ion channel) properties of cell membranes, by the properties of electrical connections between cardiac cells, and possibly by direct intracellular electrical effects (see Chapter 34). Electrical therapy for cardiac arrhythmias includes low-voltage (1 to 5 V) pacing stimuli (pulses) and high-voltage (500 to 1400 V) stimuli (shocks). Pacemakers are indicated to relieve or prevent symptomatic bradycardia not resulting from a reversible cause. The strongest indications relate to relief of symptoms confirmed to be caused by bradycardia. Pacing is also indicated in patients who have documented asymptomatic bradycardia and serious symptoms consistent with bradycardia, but no documentation of symptomatic bradycardia, provided that alternative causes for the symptoms have been excluded. Pacing is also indicated to prevent future symptomatic bradycardia in patients who are presently asymptomatic if the risk of rapid progression to serious symptoms is high. Transvenous pacemaker leads comprise a small, distal tip electrode for pacing and sensing with a fixation mechanism that anchors the lead to the heart, a proximal terminal that connects to the generator, and a lead body connecting the two (Fig. Bipolar leads have a second ring electrode located about 10 mm proximal to the tip. Top right, True bipolar (top) and integrated bipolar (bottom) defibrillation leads. The true bipolar lead senses between the distal tip and the proximal ring, which are dedicated for pacing and sensing. In contrast, integrated bipolar leads pace and sense between the tip and the distal coil. Integrated bipolar leads also contain a second, proximal coil, which increases the lead surface area for defibrillation. Conventional pacemaker generators include a plastic header to which the leads are attached and a 10- to 3 15-cm titanium casing or “can” that houses the battery, tiny capacitors that generate pacing pulses, and electronic circuitry for control and telemetry (eFig. Battery performance must be predictable over time to provide an elective replacement indicator.
Rosuvastatin 10 mg buy amex
A longitudinal incision is made over the course of the ampulla cholesterol killer foods 10 mg rosuvastatin order with visa, and the mucosa of the ampulla is sutured to the mucosa of the duodenum with fine interrupted sutures with care being taken not to compromise the pancreatic duct definition of cholesterol level rosuvastatin 10 mg lowest price. The duodenum is closed with suture cholesterol test price philippines order rosuvastatin 10 mg online, a small closed suction drain is placed, and the wound is closed. Cholecystojejunostomy usually is performed as palliation for malignant obstruction of the distal bile duct. Its advantage is that it does not require dissection of the portal triad, but the long-term results are poor as biliary obstruction typically recurs as the malignancy advances. The abdomen is opened as described above, and the region of the porta hepatis examined to ensure that the cystic duct is not imminently compromised by tumor. The jejunum is then brought up to the gallbladder, usually bypassing the jejunum through the transverse mesocolon. The anastomosis may be performed either to an intact loop of jejunum (loop cholecystojejunostomy) or to a Roux-en-Y loop of jejunum (Roux-en-Y cholecystojejunostomy) and is carried out with one or two layers of sutures, depending on surgeon’s preference. This procedure has largely been replaced by transhepatic and endoscopic techniques. Choledochoduodenostomy is an archaic procedure in which the bile duct is incised longitudinally and anastomosed directly to the adjacent duodenum. This was performed historically in patients with gallstones impacted at the ampulla. However, loss of the normal sphincter mechanism at the ampulla allows reflux of duodenal contents directly into the bile duct. Patients may suffer from repeated episodes of cholangitis or obstructive jaundice from debris occluding the anastomosis. Secondary biliary cirrhosis may occur, and the author has seen one case proceed to liver transplantation in which a cast of the biliary tree comprised of fibrous food material was extracted from the choledochoduodenal anastomosis. Roux-en-Y choledochojejunostomy or hepaticojejunostomy remains the gold standard by which all other biliary drainage procedures are measured. An anastomosis is fashioned between the common bile duct, common hepatic duct, or even the lobar or segmental bile ducts and a Roux-en-Y loop of jejunum. This is often a relatively demanding operation because it requires dissection deep in the porta hepatis to gain access to the bile duct. Furthermore, many patients have had previous surgery in the porta hepatis with extensive formation of adhesions. Long-term results are more reliable, however, and thus surgical drainage is preferred to less-invasive procedures for benign disease. The bile duct is dissected free from the surrounding structures in the porta hepatis and traced proximally into the liver to healthy tissue above the level of obstruction. Variant procedure or approaches: Endoscopic or transhepatic placement of temporary or permanent biliary stents is an increasingly common alternative to surgical drainage in patients with incurable pancreatic or biliary tract disease. Cholecystojejunostomy: malignant obstruction of the distal common bile duct, usually due to pancreatic cancer. Choledochojejunostomy or hepaticojejunostomy: benign strictures of the distal bile duct; long-standing stone disease; pancreatitis; iatrogenic injury; Oriental cholangiohepatitis; after resection of some tumors of the pancreas or bile duct. Such tumors are usually classified as being proximal bile duct tumors, involving the hepatic bifurcation and above; middle bile duct tumors, involving the midportion of the common hepatic and common bile duct; and distal bile duct tumors, which involve the distal bile duct, including the intrapancreatic or intraduodenal portion of the bile duct (Fig. Distal bile duct tumors, which carry a significantly higher cure rate than either proximal bile duct or pancreatic tumors, may be treated by pancreaticoduodenectomy. Biliary drainage usually is established by anastomosing the proximal bile duct to a Roux loop of jejunum. For proximal bile duct tumors, most of the extrahepatic bile ducts are excised and biliary drainage is established by anastomosis of the right and left hepatic ducts or even multiple segmental ducts to a Roux loop of jejunum. These are often technically demanding operations with the potential for major blood loss. It may be necessary to perform a major hepatic resection at the same time, and the possibility of this should always be assumed when an operation of this sort is carried out. Often, a transhepatic catheter will have been placed radiographically preoperatively to provide relief of jaundice and to facilitate identification of the bile ducts. Colonization of the biliary tract with enteric bacteria or yeast is common and may result in bacteremia during surgical manipulation. Prolonged cholestasis may lead to fat-soluble vitamin deficiencies, in particular vitamin K deficiency, which may cause coagulopathy.
Sanford, 29 years: Frequently, electrocardiographic findings of right ventricular enlargement are absent.
Jared, 22 years: In other patients, however, the virus is not cleared, and it causes continued myocyte damage; heart-specific inflammation may persist because of mistaken recognition of endogenous heart antigens as pathogenic entities.
Kliff, 26 years: Type I is a comminuted fracture of the along the tympanic segment of the facial nerve.
Gorok, 36 years: Clinical impact of contemporary cardiovascular magnetic resonance imaging in hypertrophic cardiomyopathy.
Dan, 44 years: Variant procedure: In patients with severe rectovaginal and vesical endometriosis, the retroperitoneal space is entered using hydrodissection, and the external iliac vessels, hypogastric artery, and ureters are identified.
Jaffar, 47 years: This disease occurs emergency situation, and treatment must be initiated as osteochondritis of the femoral head epiphysis.
Vak, 24 years: Dorotta I, Kimball-Jones P, Applegate R: Deep hypothermia and circulatory arrest in adults.
Zuben, 55 years: The episodes of bidirectional ventricular tachycardia are independent of attacks of muscle weakness, do not correlate with serum potassium levels, and can convert to sinus rhythm with exercise.
Grompel, 31 years: All surgical procedures cause a stress response, although the extent of the response depends on the extent of the surgery and the use of anesthetics and analgesics to reduce the response.
Jack, 28 years: The disrupted by pyloroplasty, gastroduodenostomy, or diarrhea usually precedes lung involvement.
Roy, 48 years: The net effect of these adjustments is to increase 2+ intracellular Ca during systole, which increases systolic function.
Hjalte, 59 years: By 5 min, there was severe coughing and expiratory wheezing with marked inspiratory stridor.
Asam, 35 years: If a larger 3–4 cm from the point of entrance, the needle volume is used, there is the risk of compression neuropathy.
8 of 10 - Review by V. Ressel
Votes: 90 votes
Total customer reviews: 90
References
- Wang CL, Tsai YH, Huang CC, et al. The role of the cuff leak test in predicting the effects of corticosteroid treatment on postextubation stridor. Chang Gung Med J. 2007;30:53-61.
- Kasuya H, Kawashima A, Namiki K, Shimizu T, Takakura K. Metabolic profiles of patients with subarachnoid hemorrhage treated by early surgery. Neurosurgery. 1998;42(6):1268-74; discussion 74-5.
- Ward GE, Hendrick JW. Results of treatment of carcinoma of the lip. Surgery 1950;27:321-342.
- Sievers TD, Yee JD, Foley ME, et al: Midazolam for conscious sedation during pediatric oncology procedures: safety and recovery parameters. Pediatrics 88:1172, 1991.