Stanley J. Kogan, MD
- Clinical Professor of Urology, Albert Einstein College of
- Medicine
- Chief, Pediatric Urology, Children? Hospital at Montefiore,
- Bronx, New York
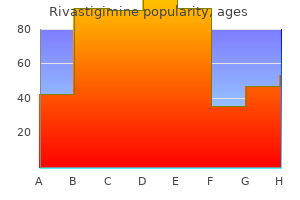
Rivastigimine dosages: 6 mg, 4.5 mg, 3 mg, 1.5 mg
Rivastigimine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
6 mg rivastigimine purchase free shipping
Herpes zoster is most common in elderly movement without weights and of desensitization and immunocompromised patients but may occur therapy medicine 606 6 mg rivastigimine mastercard. Treat- 90%) if treatment is initiated within 1 month of ment is primarily supportive medications vs grapefruit buy rivastigimine 6 mg otc, consisting of oral symptom onset and appears to decrease over time analgesics and oral acyclovir medications descriptions purchase generic rivastigimine, famciclovir, ganciclo- with therapeutic delay. Antiviral therapy reduces the Some patients beneft from transcutaneous duration of the rash and speeds healing. Spi- compromised patients with disseminated infection nal cord stimulation can be particularly efective in (nondermatomal distribution of vesicles) require both acute and chronic settings. Once the neuralgia Neuralgias Trigeminal is well established, however, sympathetic blocks, like Glossopharyngeal other treatments, are generally inefective. Tricyclic antidepressants Tumor Cerebrospinal fluid leak may be particularly efective, though their use is Pseudomotor cerebri ofen limited by anticholinergic side efects. Appli- Meningitis cation of a transdermal lidocaine 5% patch (Lido- Aneurysm derm) over the most painful area may help relieve Eye disorders Glaucoma symptoms, presumably by decreasing peripheral Optic neuritis sensitization of nerve endings and receptors. Appli- Sinus disease cation of capsaicin cream or a transdermal capsa- Allergic icin 8% patch (Qutenza) may be helpful; however, Bacterial Temporomandibular joint disease Qutenza must be administered in a monitored set- Dental disorders ting. In the vast Hypercarbia majority of cases, headaches do not refect a serious Trauma underlying disorder and are not of sufcient sever- Miscellaneous ity or frequency for the individual to seek medi- Cold stimulus (swallowing cold liquid) cal attention. However, as with other complaints of pain, the possibility of a clinically signifcant underlying disorder should always be considered. The practitioner should solicit other associated Tension Headache symptoms or clinical fndings that suggest serious Tension headaches are classically described as tight underlying pathology. Table 47–10 lists impor- bandlike pain or discomfort that is ofen associated tant causes of headache. The headache primary complaint is headache are considered in may be frontal, temporal, or occipital, more ofen the following discussion. Intensity typically builds there is signifcant variability in clinical presen- gradually and fuctuates, lasting hours to days. Tey tation and overlap in the symptoms of the major may be associated with emotional stress or depres- headache syndromes, particularly between tension sion. The headache can be bilateral photophobia, scotoma, nausea and vomiting, and or unilateral and is located in the temporal area in at localized transient neurological dysfunction (aura). The pain develops over a few The latter may be sensory, motor, visual, or olfactory. Temporal arteritis is is usually unilateral but can be bilateral with a fron- ofen accompanied by polymyalgia rheumatica, fever, totemporal location and lasts 4–72 h. It is a relatively common disorder of marily afect children (both sexes equally) and young older patients (>55 years), with an incidence of about adults (predominantly females). A family history is 1 in 10,000 per year and a slight female predomi- ofen present. Early diagnosis and treatment with steroids is (eg, red wine), menses, and sleep deprivation is com- important because progression can lead to blindness mon. The mechanism is complex and may include vaso- motor, autonomic (serotonergic brainstem systems), Trigeminal Neuralgia and trigeminal nucleus dysfunction. Treatment Trigeminal neuralgia (or tic douloureux ) is 16 is both abortive and prophylactic. Rapid abortive classically unilateral and usually located in treatment includes oxygen, sumatriptan (6 mg sub- the V2 or V3 distribution of the trigeminal nerve. It cutaneously), dihydroergotamine (1 mg intramus- has an electric shock quality lasting from seconds to cularly or subcutaneously), intravenous lidocaine minutes at a time and is ofen provoked by contact (100 mg), nasal butorphanol (1–2 mg), and sphe- with a discrete trigger. Patients are middle-aged and elderly, with include zolmitriptan nasal spray, dihydroergotamine a 2:1 female to male ratio. Prophylactic stem, cerebellopontine angle tumor, or multiple treatment may include β-adrenergic blockers, cal- sclerosis. The drug of choice for treatment is carbam- cium channel blockers, valproic acid, amitriptyline, azepine although it carries a risk of agranulocytosis.
Rivastigimine 3 mg online
The palms of the hand and the soles in a region of increased pigmentation over the dorsum of the hand medications hair loss order 1.5 mg rivastigimine overnight delivery, es- of the feet can be the site of very symptomatic lesions pecially the 1st web space G medicine 2410 generic rivastigimine 3 mg with visa. Note the color difference of the yellow subcutaneous ing due to a valgus deformity of the ankle and a very rapidly growing medicine yoga best buy rivastigimine, fat beneath the skin fap and the dark, orange fat within the mass. Sensation was redundant posterior tibial nerve with accompanying vascular structures intact and there were no hyper callosities. Histologic diagnosis was consistent with neurofbro- tous infltration, which had extended along the entire arm and the chest sarcoma. Within months he lost all hand ed, nodular antebrachial cutaneous nerve of the forearm is shown. Note the pigmented freckles within the axilla and around the entire arm including the hand functioned very well post operatively and affected breast (Crowe’s sign) the skin overlying the involved tissue. Both plexiform types of lesions carry a contained within the subcutaneous space and characteristi- high risk of malignant degeneration (. They have the same Multiple neurofbromatosis affects neural tissue of several unpredictable growth patterns as the nodular form. These areas including the brain, spinal cord, cranial nerves, and pe- diffuse lesions can be massive and may involve the thorax ripheral and sympathetic nerves. It may involve any organ with extension into the upper limb or the pelvis and into in the body from the skin to bone as in congenital pseudoar- the lower limb. Associated Syndromes These are often presenThat birth and may increase in number and size with increasing age. Approximately 25 % of neurof- Von Recklinghausen disease bromas are located in the head and neck region, [2] with 6. The Noonan syndrome for example is quite similar to the Turner syndrome and a clear defnition between the two will become more specifc. Of practical im- portance to the upper limb surgeon are the occurrence of com- pression neuropathies, peripheral nerve sheath tumors, and the secondary degeneration of the plexiform neurofbromas. The three syndromes discussed below are grouped together due to their increasing genotypic and phenotypic similarities. Sporadic and multiple neurofbromas in the head and neck region: a retrospective study of 33 years. He is best known for his descrip- tion of hemochromatosis and iron accumulation within body tissues. The cutaneous nodules have many the following clinical features [2]: (1) six or more skin cafe- forms as indicated and with the exception of the diffuse plexi- au-lait spots, (2) axillary or groin freckling, (3) two or more form type develop during the childhood years. Nearly all patients (97 %) exhibit enough features to allow diagnosis by 8 years of age, and almost all General musculoskeletal In addition to the multiple skin will by 20 years of age [1–4]. The incidence is approximately lesions, bone dysplasia is most commonly manifested as 1/3,000 live births. Upper extremity Painful enlarging skin tumors may be pres- Presentation Only those with striking skin manifestations ent within the upper limb. The cutaneous freckling within the of diffuse plexiform types will be evidenThat birth. The axil- axilla is more commonly associated with the Noonan varia- lary freckling (Crowe’s sign) is usually detected between 2 tion. These are typically smaller than 1cm and the anterior and posterior surfaces of the upper limb as well may also occur around the breasts, above the eyelids, and on as on the dorsal surfaces of the wrist and hand. Multiple cutaneous nodules begin to grow in early stain similar to a capillary malformation typically overlies in- childhood and can occur anywhere on the body and continue to volved regions of subcutaneous tissue. Café-au- mas do arise beneath the glabrous surfaces of the palm of the lait spots are cutaneous macules, which begin to develop within hand and the sole of the foot. To meet diagnostic criteria more than with rubbery, mobile palms or soles, which make walking or six macules greater than 5 mm (prepubertal) or > 15 mm (post- gripping challenging. The longest diameter of each surface as all the abnormal growth is within the dysplastic fat lesion is measured. At surgery there is a clear demarcation between the nor- within the iris and on slit lamp examination are pathognomonic mal and dysplastic adipose tissue planes.
Discount 4.5 mg rivastigimine visa
Pulmonary oedema may be associated with fuid overload associated with renal failure symptoms zoloft overdose purchase discount rivastigimine line. Leg ulcers are common and the site of an ulcer on the leg may provide a clue to its aetiology treatment coordinator generic 1.5 mg rivastigimine with amex. The ulcer is in a characteristic position on the distal medial aspect of the lower limb treatment definition best purchase rivastigimine. A prior history of intermittent claudication suggests ischaemic ulcers, as does a history of atrial fbrillation or subacute bacterial endocarditis (embolic). The presence of a longstanding venous ulcer with recent change in the shape of the ulcer suggests development of a squamous cell carcinoma (Marjolin’s ulcer). A history of rheumatoid arthritis or collagen disease may suggest a vasculitic lesion. A pigmented ulcerating lesion arising at the site of a previous mole or de novo may suggest a malignant melanoma, especially if there is a history of prolonged exposure to the sun or sunburn. Pyoderma gangrenosum may occur in association with Crohn’s disease or ulcerative colitis. Venous stasis ulcers usually occur on the medial aspect of the lower third of the leg, usually over the medial malleolus. A punched-out edge suggests an ischaemic ulcer or a syphilitic gummatous ulcer (rare). A rolled edge is characteristic of a rodent ulcer, while an everted edge is suggestive of a malignant ulcer, e. Ischaemic ulcers may contain no granulation tissue but have black necrotic tissue, or tendon or bone visible in the base. Syphilitic ulcers have a classical appearance of slough in the base, which resembles a wash leather. Surrounding tissues Is the surrounding skin pink and healthy with normal innervation? Remember that, although the initial lesion may have been caused by trauma, other abnormalities may be present to prevent healing, e. Ulcers over the shin in elderly women with thin skin may have been due to minor trauma. However, the fact that the skin there is poorly supported on the periosteum of the underlying bone means that they may be extremely slow to heal. They may also prevent appropriate contact with a partner, leading to emotional problems. In the elderly, carcinoma is a common cause of a lump on the lip, especially in those with outdoor occupations. He presented with a non-healing ulcer of the lip, which proved to be a well- differentiated squamous cell carcinoma on biopsy. The only abnormality may be a slight indentation in the outer part of the middle third of the upper lip. Ensure that there has been no change in a junctional naevus to suggest development of malignant melanoma. In hereditary telangiectasia, the patient may also have noticed lesions in the mouth and on the skin, especially the fngertips. The patient complains of a lump on the inner aspect of the lip, which interferes with eating. With 318 Lip Lesions warts, pyogenic granuloma and squamous cell carcinoma, the patient’s only complaint is usually of a lump on the lip. With carcinoma, there may be a history of leucoplakia, betelnut chewing or pipe smoking. There may also be a history of exposure to sunlight, and carcinoma is common in outdoor workers, e. Malignant melanoma may present as a black, ulcerating or raised lesion at the site of a junctional naevus.
Cheap rivastigimine 1.5 mg buy on-line
Just prior to arrest medications identification rivastigimine 6 mg purchase overnight delivery, the most common signs Urticaria—angioedema were bradycardia medications list form rivastigimine 6 mg purchase fast delivery, hypotension medications gout purchase rivastigimine 1.5 mg mastercard, and cyanosis. Rapid appropriate treat- ment of bradycardia and hypotension is essential to minimize the risk of arrest. Early treatment of bra- dycardia with atropine may prevent a downward allergen, may be a protein, polypeptide, or smaller spiral. Moreover, the allergen may be the sub- and other vasoactive drugs should be given to treat stance itself, a metabolite, or a breakdown product. If cardiopulmonary arrest occurs, ven- Patients may be exposed to antigens through the tilatory support, cardiopulmonary resuscitation, respiratory tract, gastrointestinal tract, eyes, skin and full resuscitation doses of atropine and epineph- and from previous intravenous, intramuscular, or rine should be administered without delay. The incidence of low- in the same manner as anaphylactic reactions, but frequency hearing loss following dural puncture may are not the result of an interaction with IgE. It seems to be due to cerebrospinal activation of complement and IgG-mediated com- fuid leak, and, if persistent, can be relieved with an plement activation can result in similar infamma- epidural blood patch. Mechanisms include middle tem components involved, hypersensitivity reactions ear barotrauma, vascular injury, and ototoxicity of are classically divided into four types (Table 54–5). Hearing loss following cardiopulmonary bypass is Type I reactions involve antigens that cross-link usually unilateral and is thought to be due to embo- IgE antibodies, triggering the release of infamma- lism and ischemic injury to the organ of Corti. Atopic disorders typically that have been sensitized to a specifc antigen by afect the skin or respiratory tract and include aller- prior exposure. Urticarial lesions are characteristically expression of the specifc sensitized T cells and well-circumscribed skin wheals with raised ery- attracts other types of T cells. When angioedema is extensive, it can with tuberculosis, histoplasmosis, schistosomiasis, be associated with large fuid shifs; when it involves and hypersensitivity pneumonitis and some autoim- the pharyngeal or laryngeal mucosa, it can rapidly mune disorders, such as rheumatoid arthritis and compromise the airway. Immediate Hypersensitivity Anaphylaxis is an exaggerated response to an Reactions allergen (eg, antibiotic) that is mediated by a type I nitial exposure of a susceptible person to an antigen I hypersensitivity reaction. The Fc portion of these antibodies Death may occur from asphyxiation or irreversible then associates with high afnity receptors on the circulatory shock. The incidence of anaphylactic cell surface of tissue mast cells and circulating baso- reactions during anesthesia has been estimated at a phils. During subsequent reexposure to the antigen, rate of 1:3500 to 1:20000 anesthetics. Mortality from it binds the Fab portion of adjacent IgE antibodies anaphylaxis can be as frequent as 4% of cases with on the mast cell surface, inducing degranulation and brain injury, occurring in another 2% of surviving release of infammatory lipid mediators and addi- patients. The end result and anaphylactoid reactions reported that the most is the release of histamine, tryptase, proteoglycans common sources of perioperative anaphylaxis were (heparin and chondroitin sulfate), and carboxy- neuromuscular blockers (58%), latex (17%), and peptidases. Tey increase cleaves bradykinin from kininogen; bradykinin vascular permeability and contract smooth muscle. Activation of Hage- muscle, whereas H2-receptor activation causes man factor can initiate intravascular coagulation. Leukotriene and prostaglandin media- Organ System Signs and Symptoms tors may also cause coronary vasospasm. Prolonged Cardiovascular Hypotension, 1 tachycardia, arrhythmias circulatory shock leads to progressive lactic acido- Pulmonary Bronchospasm,1 cough, dyspnea, sis and ischemic damage to vital organs. Table 54–6 pulmonary edema, laryngeal edema, summarizes important manifestations of anaphylac- hypoxia tic reactions. A drug can directly release histamine from mast cells (eg, urticaria following high-dose mor- Eosinophil chemotactic factor of anaphylaxis, neu- phine sulfate) or activate complement. D e s pite 6 trophil chemotactic factor, and leukotriene B4 attract difering mechanisms, anaphylactic and ana- infammatory cells that mediate additional tissue phylactoid reactions typically are clinically indistin- injury. Table 54–7 trachea produce upper airway obstruction, whereas lists common causes of anaphylactic and anaphylac- bronchospasm and mucosal edema result in lower toid reactions. Histamine may preferentially F actors that may predispose patients to these constrict large airways, whereas leukotrienes pri- reactions include pregnancy, known atopy, and pre- marily afect smaller peripheral airways. Such reactions are more com- tion of fuid into the skin (angioedema) and viscera mon in younger than older patients. The inci- dence of anaphylaxis for thiopental and propofol Discontinue drug administration Administer 100% oxygen is 1 in 30,000 and 1 in 60,000, respectively. The latter is capable of measuring the level the preservative (paraben or methylparaben) was of drug-specifc IgE antibody in the serum. Serum believed to be responsible for an apparent anaphy- tryptase measurement is helpful in confrming the lactoid reaction to a local anesthetic. Prophylactic cross-reactivity between amide-type local anesthet- pretreatment with histamine receptor antagonists ics seems to be low.
Buy cheap rivastigimine line
If pressure is measured treatment varicose veins rivastigimine 6 mg purchase otc, this should • attendants should be familiar with the be done with the transducer level relative to the monitors to ensure that the data derived from them are accurate • lines must be dressed aseptically and changed at appropriate intervals treatment hpv rivastigimine 1.5 mg low price. The radial artery is the most frequent anatomical site medications kidney stones 6 mg rivastigimine purchase with visa, followed by the dorsalis pedis artery, and a 20G or 22G sized cannula is used. The brachial and femoral arteries should be avoided if possible because of lack of collaterals and, in the case of the femoral site, the risk of sepsis. Th When using the radial artery, always check for ulnar flow supply to the palmar arch using Allen’s test prior to cannulation (Fig. Local sepsis Little finger a) and coagulopathy are the main contra-indications while complications include haematoma, thrombosis, distal ischaemia, intimal damage, false aneurysm formation, disconnection and injection Release of irritant drugs. Samples from arterial cannulae pressure should be taken aseptically and the line flushed and re-sealed afterwards. After cannulation of the artery, the cannula should be connected to a continuous-flush device containing heparinised saline under pressure which maintains patency and allows blood pressure changes to be conducted without letting blood flow out of the artery into the line. Blanch the hand by clenching the fist then simultaneously occlude radial and ulnar arteries at the wrist. An adequate pink flush of the hand on release of the ulnar pressure confirms an adequate ulnar supply to the palmar arterial arches. Cannulation: the Seldinger technique • puncture as above • advance guide wire • railroad cannula • check backflow and secure cannula Railroad cannulation Connect and secure • connect transducer and flushing set-up. Check that the transducer is determine patients who will respond to a fluid zeroed, calibrated at the correct level and that the challenge by increasing their stroke volume. The arterial waveform gives the systolic pressure variation, the pulse pressure real-time information about the blood pressure and variation or, nowadays when combined with a heart rate, but also modern computer algorithms cardiac output monitor, the stroke volume variation. The morphology of the individual used monitoring tools in critical care, indicating waveform can also give information with regards preload of pulmonary circulation and a rough to the systemic vascular resistance and cardiac guide to systemic preload given a number of contractility in both normal and pathological provisos. The of the operator and the presence of site-specific alternative, the 2nd intercostal space at the sternal contra-indications such as local sepsis, edge, represents a point about 5 cm above the coagulopathy, abnormal anatomy, operative site atrium. While the techniques times, they should always be taken from the same are illustrated in Figure 8. The terms of a lower rate of complications, but is electronic transducer is faster and the analysis uncomfortable and difficult to dress. The subclavian of the signal produced allows the mean pressure route entails a higher risk, in particular the risk to be displayed taking into account the variation of pneumothorax and intrathoracic bleeding, with the respiratory cycle. A wave, atrial contraction; C wave, bulging of the tricuspid valve into the right atrium; X descent, atrial relaxation; V wave; rise in atrial pressure prior to tricuspid valve opening; and Y descent, atrial emptying. These comprise aspects regarding Complications include rupture of vessel and line insertion, including aseptic techniques, haemorrhage with local haematoma or skin preparation and hand hygiene, and on going haemothorax, tension pneumothorax care of the line, including regular inspection, (particularly if the patient is on positive aseptic techniques and regular replacement of pressure ventilation), air embolism, extravascular administration sets. Cardiac output is, therefore, a pivotal hypoperfusion is likely variable in the management of the critically ill – If too low, maintenance of an adequate surgical patient. This echocardiography appears as a triangular shaped waveform since Bedside echocardiography is becoming increasingly the shift signal is displayed as a velocity/time plot. The accuracy of the method is improved as the cannula contains a sensitive thermistor allowing thermodilution. The small drop in the temperature of arterial a blood that follows the injection of a bolus of ice- c cold saline into a central vein is proportional to b d cardiac output. The thermodilution measurement is used to calibrate the continuous cardiac output Time monitoring software which calculates changes in cardiac output by analysing the pulse contour of Figure 8. As in thermodilution, by preload, afterload, heart rate, rhythm, lithium-dilution is combined with continuous contractility and balance of oxygen demand pulse contour analysis and similar recalibration and supply. If the heart is damaged, for a given requirements and issues with damped arterial preload or afterload, cardiac output will decrease. This can be represented graphically either by pressure–volume loops or by the more familiar Frank Starling curve (see Chapter 7, Fig. Accurate their use and refer the patient to the appropriate measurements of derived variables can predict level of care. Ideally, in • adequate cardiovascular function is a addition to these properties, they should reduce pre-requisite for survival afterload and preload, resulting in decreased • to determine cardiovascular function accurately trans-ventricular wall tension, promoting coronary and to control manipulative therapy, invasive blood flow, increasing myocardial oxygen delivery monitoring is necessary and reducing oxygen consumption. Regrettably, • all techniques have complications the ideal inotrope does not exist but the most • the monitoring utilised should be appropriate commonly used are adrenaline, noradrenaline and to the specific case in question. They all act by providing an upward left shift in the Starling curve as shown in Figure 7. The kidneys have a wide range of blood flow is around 20% of cardiac output (1000 functions and play a vital role in homeostasis.
Rivastigimine 1.5 mg order
After one cycle of therapy symptoms 9 days before period discount rivastigimine 3 mg, some improvement Anterior mediastinal masses in patients present- was noted in the patient’s symptoms symptoms 3 days before period purchase 3 mg rivastigimine fast delivery. Lymphoproliferative disorders present- eral days prior to obtaining tissue for diagnosis symptoms 5-6 weeks pregnant rivastigimine 6 mg low price, may ing as mediastinal neoplasms. Semin Thorac Cardiovasc Surg obscure the pathologic interpretation, especially if 2000;12:290–300. The diffusion capacity is 71% of the film to a previous chest radiograph to determine predicted. The bronchoscopic examination is unremark- able, with no evidence of any mucosal abnormality or discrete endobronchial lesion. The cytology stud- Case Continued ies from the bronchial brushings and bronchoalveo- lar lavage show no evidence of malignancy. The patient reports that she had a chest radiograph done 5 years ago, which was “normal;” however, the film is no longer available for review. On further review you find the patient to be quite A solitary pulmonary nodule larger than 1 cm in a healthy and very active. Her past surgical history is person who smokes requires a definitive tissue diag- significant for 2 cesarean sections and a hysterec- nosis. She has no history of malignant disease and further evaluation determines that the disease but admits to a 40-pack-year smoking his- patient can tolerate a pulmonary resection, proceed tory, as mentioned previously. She has no palpable to the operating room for both definitive diagnosis supraclavicular, cervical, or axillary adenopathy on and treatment. A 2-year period of serial scans is required before assuming that a lesion is benign and Differential Diagnosis does not need further surveillance. The differential diagnosis of a solitary pulmonary nodule is quite broad and can include both benign ■ Surgical Approach and malignant processes. Patient-specific factors, especially a smoking history, increase the probability The patient was taken to the operating room. General anesthesia was induced, and she was intu- Our patient, with her significant smoking history, bated with a double-lumen, left-sided, endobronchial tube. Flexible bronchoscopy was performed, and no has a high likelihood of harboring a primary carci- noma of the lung. In appropriate clinical settings, abnormalities were seen down to the subsegmental other possibilities include metastatic nodules from level bilaterally. The tube was bronchoscopically posi- commonly encountered cancers, including breast, tioned for isolated lung ventilation and secured in place. The patient was repositioned and underwent colon, thyroid, or renal cell carcinomas. Other possibilities include inflammatory or infectious nodules, the using multiple firings of an endoscopic stapling most common lesion being a granuloma. Intraoperative frozen section revealed a non- fungal diseases, including coccidioidomycosis and small cell carcinoma of the lung. The thoracoscopic histoplasmosis, may present with a solitary pul- port sites were converted to a thoracotomy and a monary nodule, as may actinomycosis. The elusive right upper lobectomy with mediastinal lymph node rounded atelectasis, seen as a pleural-based lesion, dissection was performed. Discussion In approaching a person who smokes, and who has a new solitary pulmonary nodule suspected of being Diagnosis and Recommendation a primary lung cancer, the following three questions A solitary pulmonary nodule is defined as a lesion should be addressed: (a) what is the extent of dis- less than 3 cm in size, surrounded by lung and with- ease? If the transthoracic needle biopsy The extent of disease is surmised by a combina- is positive for carcinoma of the lung, the patient tion of history, physical examination, and radi- requires a pulmonary resection for treatment. Subtle neurologic signs, such as needle biopsy is nondiagnostic, as is typical if a blurred vision or new headaches, require a brain mag- diagnosis of malignancy cannot be made, the netic resonance imaging study to rule out metastatic patient requires an operation for diagnosis and disease. Long bone or rib pain may indicate bony lobectomy for treatment if the diagnosis of carci- metastatic disease and should be excluded with bone noma is confirmed. The chance of performed if mediastinal adenopathy (lymph nodes small cell lung cancer, a disease usually treated non- larger than 1. Activity levels usually are the best indicator of a patient’s ability to tolerate a pulmonary resection, but unfortunately, these are difficult to quantify during an office visit.
Cheap rivastigimine 3 mg buy on-line
The neurovascular bundle of C5 treatment 2 stroke cheap rivastigimine 1.5 mg buy line, C6 xanax medications for anxiety buy discount rivastigimine 4.5 mg, and C7 nerve roots lie within the interscalene groove treatment ingrown toenail order rivastigimine online now. Although nerve stimulation may be equally efficacious in performing the brachial plexus block at this location, the total amount of local anesthetic required may be decreased under the guide of ultrasonography. Complications A successful block of this nature is often accompanied by Horner syndrome, recurrent laryngeal nerve block, and hemidiaphragmatic paralysis on the ipsilateral side of the block. These clinical symptoms should not be mistaken for 28 Yearbook of Anesthesiology-6 complications but rather as expected. Caution should be taken when considering the use of the interscalene block in the pediatric population as potential risks of pneumothorax, intrathecal injection, and vertebral artery injection exist. Supraclavicular Approach Anatomy and Indications The brachial plexus may be blocked in the supraclavicular fossa with subsequent analgesia provided to the elbow and upper arm. The trunks and divisions of the plexus are located anatomically anterolateral to the subclavian artery (Fig. Despite the known efficacy of single-injection supraclavicular nerve blocks, limited data exists regarding continuous supraclavicular blocks in children. Technique Few techniques have been specifically described in the pediatric population but can be extrapolated from adult literature. The subclavian artery should appear as the pulsatile hypoechoic structure and must be the first structure identified. An in-plane approach is utilized to guide the needle in the direction of the brachial plexus, above the first rib and just superior and lateral to the subclavian artery. Needle guidance in a lateral to medial direction allows the brachial plexus to be reached prior to the subclavian artery avoiding vascular puncture and intraneural injection. Furthermore, as the lung parenchyma lies medial to the first rib, completion of the supraclavicular block can result in an increased risk of an ipsilateral pneumothorax. For this reason, real time visualization of the needle tip and shaft during placement of the block with ultrasound may prevent such morbidity. Infraclavicular Approach Anatomy and Indications The infraclavicular block provides analgesia similar to that of the supraclavicular block. Visualization of the brachial plexus cords occurs just below the coracoid process. Medial to the cords lie the axillary artery and vein while anterior to the neurovascular bundle lie pectoralis major and minor (Fig. On ultrasound, the lateral cord of the plexus is seen as a hyperechoic structure while deep to the axillary artery is the posterior cord. Due to its location between the axillary artery and vein, the medial cord may be challenging to identify. Safe and effective means of controlling acute pain in the pediatric population using a continuous infraclavicular nerve blockade following radial osteotomy and simplified skin fixation procedure has been described. The axillary artery is identified with the ultrasound probe in a transverse position below the clavicle. An out-of-plane technique is used to advance the needle to the plexus with care to avoid the vascular structures. Alternatively, the probe can be positioned parallel to the clavicle in a parasagittal plane and the needle can then be directed in a cephalad direction toward the brachial plexus. The catheter is checked for inadvertent intravascular placement and secured to the chest. Complications Hematoma, infection, and intravascular injection are possible complications of the infraclavicular nerve block. The cervical pleura is located within close proximity to the brachial plexus and at this position the risk of a pneumothorax still exists. Ultrasound guidance has not only increased the ease of completing truncal blocks but also their effectiveness and safety. Anatomically, the three muscle layers, the external oblique, internal oblique, and transversus abdominis lie lateral to rectus abdominis muscles (Fig. The rectus abdominis is identified by placing the ultrasound probe lateral to the umbilicus. Movement of the probe laterally to the rectus allows for visualization of the three muscle layers of the abdominal wall, the external oblique, internal oblique, and transversus abdominis. Upon injection, a pocket of local anesthetic can be created where the nerves traverse. The catheter tip is localized when saline solution or local anesthetic is injected through the needle.
Varek, 40 years: Tumors limited to the nasopharynx may result in nasal symptoms such as epistaxis or obstruction.
Rune, 30 years: Isoflurane is a hepatic enzymes, including those of anaesthetists and potent coronary vasodilator and in the presence of a coro- operating theatre staff.
Potros, 31 years: External inflammatory resorption after trauma is a well-known complication after intrusive luxation injuries and replantation of avulsed teeth, progresses quickly, and is radiographically distinguished by cavita- tion-like areas of low density along the root surface and surrounding alveolar bone.
Abbas, 62 years: High doses increase the ef- ventional amphotericin in invasive aspergillosis, and prob- fects of phenytoin, ciclosporin, zidovudine and warfarin.
Larson, 46 years: Scans should not be obtained (ankylosing spondylitis, reactive arthritis, enteropathic post-contrast in a delayed fashion because there can be spondylitis associated with inflammatory bowel diseases, diffusion with time of contrast into the disk itself from psoriatic arthritis, and undifferentiated spondyloarthropa- adjacent vascular tissue (such as scar).
Fraser, 37 years: Respiratory End products of ketamine biotransformation are Ventilatory drive is minimally afected by induction excreted renally.
Yokian, 54 years: The monary O2 toxicity in newborn infants is manifested potential for oxygen enriched gas mixtures to pro- as bronchopulmonary dysplasia.
Felipe, 28 years: Pathology Report Microscopic examination reveals a paraganglioma Recommendation with high suspicion of being malignant, although this diagnosis is often difficult without evidence of Follow-up of patients operated for pheochromocy- metastatic growth.
Koraz, 61 years: Another study has shown that only 3% of patients who suffered negligence filed a lawsuit.
Angar, 41 years: After the successful transplantation of a cadaveric kidney and pancreas (drainage in the urinary bladder) the patient had normal pre-prandial and post-prandial blood sugar levels without the use of insulin, although a glucose tolerance test was abnormal.
8 of 10 - Review by D. Dan
Votes: 20 votes
Total customer reviews: 20
References
- Coker KH. Meditation and prostate cancer: integrating a mind/body intervention with traditional therapies. Semin Urol Oncol 1999;17(2):111-118.
- Pagana TJ. A new technique for hepatic infusional chemotherapy. Semin Surg Oncol. 1986;2(2):99-102.
- Gangarosa LP, Mahan PE. Pharmacologic management of TMJMPDS. Ear Nose Throat J 1982;61:670.
- Packer M, Coats AJ, Fowler MB, et al. Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med 2001;344:1651-1658.
- Preminger GM, Sakhaee K, Skurla C, et al: Prevention of recurrent calcium stone formation with potassium citrate therapy in patients with distal renal tubular acidosis, J Urol 134(1):20n23, 1985.
- Giralt M, et al: Adipose tissue biology and HIV-infection, Best Pract Res Clin Endocrinol Metab 25(3):487-499, June 2011.
- Ferrando Marco J, Pallas Regueira A, Moro Valdezate D, Fernandez Martinez C. [Collision tumor of the ampulla of Vater: carcinoid and adenocarcinoma.] Rev Esp Enferm Dig 2007;99:235.