TuTran Nguyen, PharmD, BCPS
- Adjunct Faculty, Department of Clinical Pharmacy Practice, Butler University College of Pharmacy and Health Sciences
- PGY-2 Internal Medicine Pharmacy Resident, Indiana University Health Methodist Hospital, Indianapolis, Indiana
Colospa dosages: 135 mg
Colospa packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Colospa 135 mg with amex
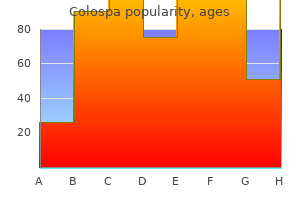
The amplitude of the evoked muscle response is plotted over time xanax muscle relaxant qualities purchase colospa amex, and has a sigmoidal shape spasms urethra purchase colospa 135 mg overnight delivery. Once the amplitude of the muscle response no longer increases as current intensity increases spasms right side of stomach order colospa 135 mg online, the response is maximal, and the current required is called “maximal current. The characteristics of the various patterns of neurostimulation currently in use clinically are summarized in Table 21-5. B: Acceleromyographic neuromuscular monitor—StimPod (Xavant Technologies, Pretoria, South Africa). Electrodes are placed along the ulnar nerve, with the negative (black) electrode distal to the positive (red) electrode. The accelerometer is taped to the thumb, with the sensor perpendicular to the direction of thumb adduction. T = first stimulus in the sequence; T =1 2 second stimulus in the sequence; T = third stimulus in the sequence; T = fourth3 4 stimulus in the sequence. Unblocked state, no fade between tension at the beginning of the 5-second stimulation (S ) and the end of the stimulation (S ). The ratio of tension at the end of the1 5 5-second stimulation to that at the beginning is the tetanic ratio (S /S ratio). The ratio of tension at the end of the 5-second stimulation1 5 to that at the beginning is the tetanic ratio (S /S ratio). The number of rapidly fading twitches is counted; the resulting number of twitches is the posttetanic count. Because the stimuli are mini-tetanic, each of the two bursts result in a single (fused) muscle contraction. Because the stimuli are mini- tetanic, each of the two bursts result in a single (fused) muscle contraction. Because the stimuli are mini-tetanic, each of the two bursts results in a single (fused) muscle contraction. Because D consists of2 only two mini-tetanic stimuli, the evoked (fused) muscle response is slightly less than that induced by D. Because the stimuli are mini-tetanic, each of the two bursts results in a single (fused) muscle contraction. During a partial nondepolarizing block, the ratio decreases (fades) as the degree of block increases (Fig. Below this threshold, repetitive nerve stimuli result in individual, rapid contractions. At frequencies above 30 Hz, the muscle responses become fused into a sustained contraction without fade (tetanic ratio = 1. During partial nondepolarizing block, the tetanic contraction gets weaker (fades; Fig. Tetanus has been studied extensively for durations of 5 seconds, so clinicians should always use 5-second durations to evaluate neuromuscular function—decisions based on tetanic durations shorter than 5 seconds will undoubtedly be inaccurate. Depending on the tetanic frequency, this period of potentiated responses may last 1 to 2 minutes after a 5-second, 50-Hz tetanus, or up to 3 minutes after 100-Hz tetanus. The72 number of posttetanic twitches is inversely proportional to the depth of block: the fewer posttetanic twitches there are, the deeper the block. By delivering two (instead of four) intense stimuli73 (mini-tetanic bursts) separated by 0. The numbers 3,3 signify that each burst contains three stimuli at a 1388 frequency of 50 Hz. Because the two individual bursts are tetanic in74 frequency, a longer recovery period between successive stimulations is necessary (20 seconds). Testing and Recording the Response There are different modalities to assess the degree of neuromuscular block, including subjective and objective evaluation and assessment of clinical criteria. When assessing the degree of block (or state of neuromuscular recovery), it is important to note that most clinicians even today evaluate responses subjectively: by visual or tactile means. The ability to detect fade is not influenced by the observers’ experience, and there is also no difference in the ability to detect fade between visual and tactile means. Therefore, clinical decisions73 based on subjective (qualitative) evaluation of fade likely are incorrect, and do not decrease the risk of oxygen desaturation or need for tracheal re- intubation. Table 21-9 Selected Reports of Postoperative Residual Paralysi, 1979–2016 1390 1391 The limitations of subjective evaluation extend to intraoperative management of the depth of block. Clinical testing has been advocated for decades; tests such as grip strength, vital capacity, tidal volume, head-lift, or leg-lift (despite their continued use) are notoriously poor at detecting residual fade.
Purchase generic colospa on-line
Rotation of the neck away from the side and thyroid gland between the levels of the inferior thyroid of swelling causes severe pain from tension on the ipsilateral artery and the oblique line of the thyroid cartilage muscle relaxant lyrics best purchase colospa. As this space communicates may allow infection to spread into the superior mediastinum spasms paraplegic discount generic colospa uk, with the other fascia spaces muscle relaxant india discount colospa 135 mg line, spread of infection may also arise as these spaces communicate. Posterior space involvement may have more ominous Fascial Spaces of the Neck signs. Lemierre syndrome may result from pharyngitis or tonsillitis with bacterial spread to the lateral pharyngeal space Te fascial spaces of the neck all lie between the deep cervical that may involve internal jugular vein thrombosis with septic fascia surrounding the pharynx anteriorly and the spine pos- emboli and metastatic infections that most frequently involve teriorly. Te other fascial spaces of the neck bophlebitis and carotid artery erosion or thrombosis. Te intraoral approach cervical fascia, and connects posteriorly to the danger space. Tey may be complicated by the development Peritonsillar Space of supraglottic edema with airway obstruction, aspiration Te peritonsillar space is a potential space of loose areolar pneumonia due to rupture of the abscess, and acute medias- tissue that surrounds the tonsil and is bounded laterally by tinitis that may lead to empyema or pericardial efusions. Most abscesses occur in younger Proximity to the danger space may allow infection to spread patients who present with fever, sore throat, and dysphagia. Surgical drainage of choice for treatment, but treatment may include serial should be performed in the operating room via a transoral aspiration or surgical drainage with tonsillectomy. Peritonsil- approach with the head down to prevent rupture during lar abscess is a complication of acute tonsillitis that is rarely intubation and septic aspiration. Lemierre syndrome may result from Danger Space tonsillitis with bacterial spread to the lateral pharyngeal space that may involve internal jugular vein thrombosis with septic Te danger space is bounded superiorly by the skull base, 14 emboli. Danger space Carotid Sheath Space infections may track from the anteriorly located retropharyn- geal space between the buccopharyngeal fascia and alar fascia Te carotid sheath space is composed of the conjoining of and pass inferiorly to the mediastinum and the pericardium, three cervical fascias—the investing layer deep to the sterno- and they may result in conditions such as purulent cleidomastoid muscle, the pretracheal layers, and the prever- 19 pericarditis. It lies posterior to the para- pharyngeal space, lateral to the retropharyngeal space, antero- Prevertebral Space lateral to the prevertebral spaces, and medial to the parotid Te prevertebral space is bounded by the anterior part of the space and styloid process. It deep cervical lymph nodes, carotid sinus nerve, and sympa- extends from the base of the skull into the mediastinum and thetic fbers. Infections that usually arise from thrombosis of ends at the level of the fourth thoracic vertebra. Te prever- the internal jugular vein or from infection deep cervical tebral space contains the prevertebral muscles (longus colli lymph nodes that lie within the sheath tend to be localized and longus capitis), vertebral artery, vertebral vein, scalene within the cervical region between the hyoid and root of the muscles, phrenic nerve, and the proximal portion of the neck, as the sheath closely adheres to the major vessels in this 20 brachial plexus. Trombosis of the jugular vein from a deep infection radiograph, the normal dimensions of the prevertebral space of the neck is probably not due to direct infection of the in an adult are 4 mm at the C3 level, with a greater than carotid sheath but rather to the fact that infectious material 7 mm value indicating an abnormality such as pathology or follows tributaries of the internal jugular vein to reach infection. Louis, 2006, Mosby, infection: imaging manifestation and pathways rare, but life threatening: a case report with pp 25-83. Early in week 4, parts of of the head and neck—develop from three germ layers: the the most dorsal germ layer, the ectoderm, transform into the ectoderm, mesoderm, and endoderm. Te thickened epithelial cells, which form the during gastrulation, a diferentiation process occurring at the neural plate, are located at and adjacent to the embryo’s cra- beginning of week 3. Te neuronal plate invaginates along this axis, refer to the gestational age of the embryo. Te free edges of the remaining surface ecto- organogenesis is completed, and during the remaining time derm fuse over the neural tube and thereby build a continu- of pregnancy (the fetal period) the organs continue to grow ous layer, which later will diferentiate into epidermis. Te cranial portion of the 2 neural tube, the future brain, closes completely on day 25. In week 4, the brain develops at the cranial pole of the Failure of this fusion results in anencephaly and is incompat- embryo by neurulation (discussed later). Anencephaly occurs with an inci- 3 4, optic vesicles, which will substantially contribute to the dence of approximately 1 in 4800 live births and is always formation of the eyes, have protruded from the developing accompanied by acrania, the partial or complete absence of brain. Together with the stomodeum, the primordium of the the cranial vault (Figure 9-2). At the same time, mesenchymal tissue as they detach from the neural tube and migrate to various around the developing brain starts to form the skull. Tey form a vast array of structures, 7 and 8, the facial structures, such as jaw, nose, eyes, and ears, such as the ganglia of the autonomic nervous system, the become more defned.
Diseases
- Maturity onset diabetes of the young
- Radiation induced angiosarcoma of the breast
- Trismus pseudocamptodactyly syndrome
- Egg shaped pupils
- Renal glycosuria
- Short stature Brussels type
- Cardiomyopathy cataract hip spine disease
- X-linked mental retardation associated with marXq2
- Achondroplasia Swiss type agammaglobulinemia
Purchase cheap colospa line
Brain tissue oxygen monitors measure the partial pressure of oxygen (PbtO ) in a portion of brain2 interstitium 15 to 20 mm wide muscle relaxant use purchase generic colospa on-line, directly and invasively muscle relaxant otc usa cheap 135 mg colospa fast delivery, via a Clark-type electrode spasms rib cage area cheap colospa on line. PbtO values reflect the balance2 2 between oxygen supply and demand in the region of brain surrounding the electrode. Generally, values below 20 mmHg in2 pathologic brain states are considered significant and may portend secondary injury to otherwise healthy brain tissue. A filamentous catheter is placed into the brain parenchyma, consisting of outer and inner tubes and a semipermeable membrane at its tip. At the tip of the catheter, metabolites in the extracellular fluid are driven by a concentration gradient into the outer tubing and are eventually collected into a microvial. This solution is then analyzed for its metabolite contents and their concentrations, including glucose, pyruvate, lactate, glutamate, and glycerol. Clinical correlation, with attention to the location of the catheter tip and comparison of values over time, is required. Although glucose, pyruvate, and lactate concentrations are measures of adequate aerobic metabolism, glutamate and glycerol levels represent ischemic neuronal stress and cell membrane degradation, respectively. For example, measurement of values obtained from regions of brain remote from the site of brain injury might indicate minimal, if any, abnormality. Therefore, microdialysis and measurement of oxygen partial pressure is best obtained from locations where “at risk” brain exists. Lastly, cerebral oximetry has become more prevalent in the clinical setting recently. A decrease of at least 20% from baseline values is considered significant hypoxia, though definitive data in this regard do not exist. Hemoglobin oxygen saturation is determined by the ratio of the absorbances of two or more different wavelengths of light allowing for the determination of oxyhemoglobin and deoxyhemoglobin. This technology differs from pulse oximetry in that it uses two photodetectors, thereby allowing for subtraction of the absorbance from hemoglobin in the scalp and skull. Specifically, near-field photodetection is subtracted from far-field photodetection, yielding a value of brain tissue oxygenation. Cerebral oximetry also differs from pulse oximetry in that it does not rely on pulsatile blood flow. Regional estimates of cerebral oxygenation in the frontal cerebral cortices provide a sensitive method of detecting changes in oxygen delivery due to the very limited oxygen reserve of this highly metabolic area. With the accumulation of intracellular calcium (Ca2+) under ischemic conditions, neuronal damage quickly occurs and is compounded by the accumulation of lactic acid. Focal ischemia occurs due to a regional insult such as an embolus or arterial disruption. Treatment of focal ischemia must be focused on restoring perfusion to the region in question. In cases of focal ischemia, a penumbra of salvageable tissue usually surrounds a necrotic core of dead parenchyma. Efforts must also be directed at restoring oxygen and substrate delivery to the ischemic penumbra that is being supplied by some collateral circulation. Profound hypothermia in humans (27ºC), as is currently used for cold-cardiopulmonary bypass, and deep hypothermia (12ºC to 18ºC) used during circulatory arrest, have been shown to provide cerebral protection. Clinical improvement has also been72 seen in neonates with hypoxic-ischemic encephalopathy treated with mild hypothermia within 6 hours of delivery. Pharmacologic Therapy for Cerebral Protection As with induced hypothermia, there is promise for cerebral protection in the setting of neuronal ischemia by both anesthetic and nonanesthetic drugs. However, most of this data comes from animal stroke models and not definitive human studies. Calcium-channel blockers, by inhibiting the 2510 effects of voltage-gated calcium channels, have been investigated, although they do not seem clinically useful for this indication. Likewise, magnesium82 has been investigated as a possible neuroprotective agent, by virtue of its antagonistic effect on various voltage-gated and transmitter-activated channels, though so far human clinical studies are disappointing. Interestingly, patients treated with statins for 1 to 6 months, without cardiac disease, showed a 16% reduction in stroke risk in a recent human study, though other human data demonstrate no protective effect, or even a deleterious effect, on patients having already suffered a hemorrhagic stroke. Glucose and Cerebral Ischemia As mentioned earlier, ischemia is rapidly detrimental to the nervous system not only because of oxygen starvation but also because glucose is the only substrate that can be aerobically metabolized by the brain under normal conditions. With cerebral ischemia and hypoglycemia, lactate is metabolized to some extent in the brain, but with much less efficacy than glucose. Hyperglycemia (serum blood glucose over88 180 mg/dL) in the setting of cerebral ischemia has also been shown to worsen neurologic outcomes, presumably by worsening cerebral acidosis in an anaerobic setting, in which glucose is converted to lactic acid.
Colospa 135 mg purchase
For patients with hormone-secreting the procedure spasms pregnancy colospa 135 mg fast delivery, whereas the neurosurgeon trained in pitu- tumors spasms define 135 mg colospa visa, biochemical follow-up should be conducted for itary surgery brings the know-how to safely resect pituitary recurrence muscle relaxant spray purchase genuine colospa line. We continue to use intraop- erative navigation but have shifted away from simple fuo- roscopy to more detailed frameless stereotactic navigation. I Endoscope Versus Microscope Lastly, a thorough knowledge of the hypothalamic-pituitary Several studies have attempted to directly compare the en- axis is necessary to manage these patients successfully in the donasal, endoscopic approach with the traditional, micro- perioperative period. When investigators able endocrinologist is helpful, the operating surgeon must compared a cohort of endonasal, endoscopically treated pa- acquire the independent comprehension of perioperative tients with a control group of patients treated with the tradi- endocrinologic issues to care for patients appropriately in tional approach, it was shown that the endonasal, endoscopic situations when specialized assistance is not available. Endoscopic, endonasal extended 1096 transsphenoidal, transplanum transtuberculum approach for resec- 2. Endoscopic endonasal approaches to the cavern- pituitary adenomas: general principles and indications in non- ous sinus: surgical approaches. Extended endoscopic endonasal transsphe- tumors with televised radiofuoroscopic control. J Neurosurg noidal approaches to the suprasellar region, planum sphenoidale 1965;23:612–619 and clivus. Laryngoscope 1992;102:198– tuitary surgery with intraoperative magnetic resonance imaging. Endoscopic endonasal E9 transsphenoidal approach: outcome analysis of 100 consecutive pro- 29. Minim Invasive Neurosurg 2002;45:193–200 neurostereoendoscopy: subjective and objective comparison to 2D. Endoscopic endonasal trans- Minim Invasive Neurosurg 2009;52:25–31 sphenoidal surgery. The role of the endoscope 2009;64(5, Suppl 2):288–293, discussion 294–295 in the transsphenoidal management of cystic lesions of the sellar re- 31. Neurosurg Rev 2008;31:55–64, discussion 64 dimensional endoscopic sinus surgery: feasibility and technical 14. San Diego: Plural Publishing; dal pituitary surgery via the endoscopic technique: results in 35 2007:89–104 consecutive patients with Cushing’s disease. Medical and surgical management of mi- endonasal extended transsphenoidal approach: anatomical study. J Neurosurg 2005;102:189– son of techniques for transsphenoidal pituitary surgery. Transsphenoidal endoscopic approach in the treatment of Rathke’s sphenoidal microsurgery versus the sublabial approach for the treat- cleft cyst. Neurosurgery 2005;56:124–128, discussion 129 ment of pituitary tumors: endonasal complications. Surgery 1999;109:1838–1840 for Rathke cleft cysts: technical considerations and outcomes. Childs Nerv Syst 2005;21:696–700 technique after endoscopic expanded endonasal approaches: vascu- 40. Laryngoscope 2006;116:1882–1886 of transsphenoidal surgery in the treatment of craniopharyngiomas. Evaluation of the J Neurosurg 2004;100:445–451 hypothalamic-pituitary-adrenal axis immediately after pituitary 41. En- sphenoidal microsurgical treatment of Cushing disease: postopera- doscopic cranial base surgery: classifcation of operative approaches. Clinical review: the strategy of im- 2005;83:45–51 mediate reoperation for transsphenoidal surgery for Cushing’s dis- 44. J Clin Endocrinol Metab 2005;90:5478–5482 growth hormone pituitary adenomas with long-acting somatosta- 60. J Clin Endocrinol Metab 2000; uation of patients with acromegaly: clinical signifcance and timing 85:1287–1289 of oral glucose tolerance testing and measurement of (free) insu- 46. Results of lin-like growth factor I, acid-labile subunit, and growth hormone- stereotactic radiosurgery in patients with hormone-producing pitu- binding protein levels. J Clin Endocrinol Metab 2005;90:6480– itary adenomas: factors associated with endocrine normalization. In: de Divitiis E, rum prolactin levels measured immediately after transsphenoidal Cappabianca P, eds.
Colospa 135 mg order otc
Dekker G spasms muscle 135 mg colospa purchase free shipping, Sibai B (2001) Primary muscle relaxant constipation colospa 135 mg without a prescription, secondary muscle relaxant for bruxism effective 135 mg colospa, in different types of hypertensive pregnancy and tertiary prevention of pre-eclampsia. Am J Reprod Immunol ential diagnosis of hypertensive pregnancy dis- 63(6):534–543 orders. Curr Hypertens Rep 1/placental growth factor ratio: an inter-assay 17(9):584 comparison. Lehnen H et al (2013) Prenatal Clinical and suspected preeclampsia: a prospective Assessment of sFlt-1 (Soluble fms-like Tyrosine cohort study. The resulting widespread endothelial dysfunction produces the clinical features of preeclampsia including hypertension and proteinuria. It is also biologically active, capable of causing endothelial dysfunction and end-organ dysfunction seen in preeclampsia. This leads to widespread endo- thelial dysfunction and end-organ dysfunction seen as the classic fea- tures of preeclampsia, being hypertension and proteinuria [5, 8]. During the last decade, four truncated splice variants have been identifed [17–19]. Furthermore, these splice variants have signifcantly differ- ent tissue distributions [20], raising the potential for different phys- iological and pathological roles. It is also capable of causing endothelial dys- function, with evidence of impaired endothelial cell invasion, migration, and tubule formation [22]. The amino acid sequence for all proteins is shown from amino acid 650, prior sequence share 100% homology between the three proteins. Slide-A-Lyzer mini-dialysis units (Thermo Fisher Scientifc) or any appropriate dialysis equipment. Produce polyclonal antibody with a commercial company or in-house if required facilities are available (see Note 1). This involves the immunization of two rabbits over a 10-week period, obtaining serum prior to immunization and at 4, 8, and 10 weeks during the protocol. Those rabbits with a good antibody response should receive an extra immunization prior to fnal sera collec- tion through an exsanguination bleed. Proceed to protein A purifcation to isolate the IgG antibody component from the sera. Proceed immediately to dephosphorylation of the cut plasmid to prevent self-ligation through the addition of Antarctic Phosphatase and its buffer to the reaction. This reaction requires further incubation at 37 °C for 60 min, prior to heat inactivation at 65 °C for 20 min. Streak cells onto ampicillin-selective agar plates and incubate overnight at 37 °C. Samples running at the correct size can be sequenced to ensure correct sFlt-1 e15a sequence and in frame orientation. Expand plasmids with correct sequence through the addition of 500 μL of the transformed E. Larger-scale plasmid isolation and purifcation are achieved using a Maxi Kit in accordance with manufactur- er’s instructions. Spin cells at 375 × g for 5 min, remove the supernatant, and resuspend cells in fresh FreeStyle 293 expression media con- taining antibiotic/antimycotic solution (1:100) to give a con- centration of 1 × 106 cells/mL. Add LucraTone™ Lupin (1:40) and pluronic acid (1:100) 24 h following transfection to promote protein production and prevent cell shearing, respectively. Spin the cell culture media at 375 × g for 5 min to clear all cel- lular material prior to the addition of NaCl to a fnal concen- tration of 0. Mix the cell culture supernatant with the resin and rotate at 4 °C for 4 h to optimize binding. Pool elutions and concentrate the protein using Amicon spin ultraconcentrators, as per the manufacturer’s instructions. Remove excess biotin using dialysis, such as the Slide-A-Lyzer mini-dialysis units. Peptide production and conjugation, as well as rabbit immuni- zations, are available commercially or can be produced by independent researchers if the facilities are available.
Syndromes
- Cover/uncover test
- Do not want, or have a partner who does not want, to be bothered by having to use other forms of birth control during sexual activity
- Being poor
- What are your other medical problems?
- Double vision
- Your doctor or nurse will tell you when to arrive at the hospital. Be sure to arrive on time.
- When a tumor or mass (clump of cells) is suspected
Discount colospa 135 mg overnight delivery
It houses the ossicles muscle relaxant while breastfeeding 135 mg colospa fast delivery, which convey the vibratory motion of the tympanic membrane to the oval Tympanic Membrane window of the inner ear infantile spasms 2 year old buy discount colospa online, thereby transmitting sound energy muscle relaxant rx order colospa. Te middle ear is lined with a modifed respiratory epithe- Te tympanic membrane is a three-layered structure separat- lium containing ciliated and secreting cells. Te volume of ing the external auditory canal from the tympanic cavity of the tympanic cavity of the middle ear ranges from 0. Te tympanic membrane frmly adheres to the middle ear and mastoid ranges from 1 cm to 21 cm. Eustachian Tube Ossicles and Middle Ear Musculature Te middle ear communicates with the nasopharynx via the Te three ossicles of the middle ear include the malleus, eustachian tube (see Figure 4-5). Te malleus is composed the eustachian tube allows middle ear air pressure to equalize of the head, neck, lateral process, and manubrium. Te tensor tympani muscle attaches in the anterior tympanic cavity, originating inferior to the to the medial surface of the neck of the malleus. Te proximal one composed of the body, short process, long process, and len- third of the eustachian tube is osseous, while the two-thirds ticular process. Te body articulates with the malleus head, portion in continuity with the nasopharynx is composed of and the lenticular process meets the stapes at the incudosta- cartilage. Te stapes is the smaller, stirrup-shaped ossicle nasopharynx as a raised structure named the torus tubarius. Te Te four muscles associated with eustachian tube are the stapes superstructure is composed of an anterior and poste- tensor veli palatini, tensor tympani, levator veli palatini, and rior crus, neck, and capitulum, which articulates with the salpingopharyngeus. Te stapedius muscle tension opening of the eustachian tube is the levator veli palatini. Te footplate is supported within the oval window gravitational and translational acceleration. Briefy described earlier, two skeletal muscles are present Semicircular Canals within the middle ear. Te stapedius muscle body runs verti- cally, medial to the mastoid segment of the facial nerve. Te Te three semicircular canals sense rotational acceleration tendon is transmitted to the middle ear space through the and communicate with the vestibule via fve orifces. Te stapedius muscle is innervated by lateral semicircular canal has two isolated openings into the the adjacent facial nerve. Te stapedius muscle is activated by vestibule, whereas the posterior and superior canals join to the stapedial refex. Loud sound from either the contralateral form the crus communis and join the vestibule as a unit at or ipsilateral ear triggers muscle contraction, dampening their posterior ends. Te endolymphatic duct enters the laby- mechanical vibration at the level of the stapes. Te stapedial rinth in the crus communi and communicates with the endo- refex requires an intact facial and cochlear nerve and can be lymphatic sac in the dura of the posterior cranial fossa. Te tensor tympani muscle semicircular canal has an ampullated end that contains its body runs adjacent to the eustachian tube, anterior the middle sensory apparatus. Te tendon enters the middle ear at the cochleari- ampullated ends in close proximity at their anterior end and form process and attaches to the medial neck of the malleus. Te Activation of this nerve decreases the movement of the ampullated end of the posterior canal is located on its inferior malleus and, thereby, the tympanic membrane. Cochlea Te cochlea is a snail-shaped structure with 21 turns that is Chorda Tympani Nerve 2 responsible for sound perception. Te turns of the cochlea are Te chorda tympani nerve travels through the middle ear coiled around the modiolus through which flaments of the space. Te nerve is unique in that it does not travel in a bony cochlear nerve travel to innervate the cochlea (Figure 4-8). After branching Cross-sectional analysis of the lumen of the cochlea demon- from the mastoid segment of the facial nerve, the chorda strates three fuid spaces: the scala tympani, scala media, and tympani nerve enters the tympanic cavity at the posterior iter. On the inner wall of the cochlea, the osseous Te nerve travels anterosuperiorly, passing lateral to the long spiral lamina extends laterally to separate the scala vestibuli process of the incus and medial to the handle of the malleus. At the cochlear apex, the osseous spiral Te nerve then exits the tympanic cavity at the anterior iter lamina is defcient at the helicotrema, where the scala tympani and travels to join the lingual nerve. Te scala media is separated from the inferiorly located scala tympani by the basal membrane, and from the superiorly located scala vestibuli by Reissner’s mem- Inner Ear brane.
Purchase colospa paypal
Normalization corrects for well-to-well variation in initial cell densities that are not due to experimental condi- tions/treatments spasms symptoms cheap colospa 135 mg fast delivery. However spasms in intestines colospa 135 mg cheap, we personally would not recommend it as there is a substantial risk of contamination once the plate is placed in the incubator and exposed to a non-sterile environment spasms kidney area order 135 mg colospa visa. Additionally, the pro- cess of removing the cells and spent medium may damage the sensitive electrodes within the wells, which would affect subse- quent experimental results. Routinely check for any corrosion of cra- dle pins as this will likely affect experimental results. Ensure that control plates (supplied with the instrument) are run to identify any problems if the instrument has not been used for a signifcant period of time. Care should be taken to recognize a poten- tial “edge effect” in the plate, as wells on the periphery of the plate are not exposed to the same humidity level as the wells within, which may affect cell behavior depending on the cell type studied. If not all the wells are used in an experiment, the unused wells can be kept sterile with a sealing adhesive flm (e. Ensure that no air bubbles are present after pipetting the cul- ture medium into the wells. The air bubbles can affect the elec- trical impedance detected in the well and give an inaccurate background measurement. Be extra careful when pipetting medium containing fetal calf serum, which can produce a lot of bubbles. One method to avoid air bubbles is to perform reverse pipetting, which will allow the target volume to be released without introducing any air. If you need to treat the cells, pause the cell impedance moni- toring step, remove the plate from the station and add the test compounds to the culture medium or replace the culture Real-Time Monitoring of Placental Cells Behavior 275 medium in the wells with pretreated culture medium. Another possibility is to plate cells directly in pretreated culture medium at the beginning of the experiment, but be aware that treat- ments may affect cell adhesion. If at any time point of the experiment, the culture medium needs to be removed to either renew the medium or to add pretreated culture medium to the wells, avoid touching the bottom of the wells with the pipet tip as it could detach cells and introduce additional variability to the experiment. This can be done by leaving a small amount of culture medium (10 μL) in each well. Fresh culture medium should be added carefully, ideally by pipetting down slowly against the inside wall of the well. When coating the wells with Matrigel™ for the invasion assays, ensure that ice-cold medium is used to dilute the Matrigel™. It is also imperative that there are no air bubbles in the Matrigel™ coating, as these will interfere with cell movement through the matrix. The coated plate can then be incubated for 30 min at 37 °C or left in the cell culture cabinet overnight at room temperature to set. If using the incubator, do not leave the gel to set for more than 2 h as the coating may dry out. A “click” sound should be heard when attaching the upper and lower chambers together. This work was further supported by March of Dimes Social and Behavioral Sciences Research (grant no. Nystad M, Sitras V, Larsen M, Acharya G (2014) model for fundamental and applied studies of Placental expression of aminopeptidase-Q (lae- human fetoplacental steroidogenesis and inter- verin) and its role in the pathophysiology of pre- ference by environmental chemicals. These alterations generate situations of hypoxia and hypoxia/reoxygenation (H/R) and consequent oxidative stress, increased cell death, and infammation in trophoblasts. The models used to understand the effects of hypoxia and H/R on trophoblasts require a rather big structure. This chapter describes the details of a suitable and reasonable approach with hypoxia chambers to expose human placental trophoblasts to variable conditions of oxygenation. Key words Normoxia, Hypoxia, Hypoxia/reoxygenation, Villous trophoblast, Extravillous tropho- blast, Syncytiotrophoblast 1 Introduction Across the frst trimester of pregnancy, hypoxia has a key role in the uterine invasion. Low con- centrations of oxygen (15–20 mmHg or <2% O2) during the pla- centation are gradually increased, and the end of the pregnancy is coincident with relatively high levels of oxygen (55–60 mm Hg or <8% O2) [1, 2]. This increase is tightly regulated and is correlated with successful pregnancy outcomes. The etiology of preeclampsia is still a source of debates and some epidemiological studies suggest that it has a genetic and immunological origin. Regardless of its origin, the effects of preeclampsia are well characterized with several Padma Murthi and Cathy Vaillancourt (eds.
Cheap colospa express
They may also be more difficult to diagnose and treat in a patient for whom manipulation may be difficult or dangerous muscle relaxant juice cheap colospa amex. Initial Management Patients presenting with acute spinal cord injury muscle relaxant 563 pliva colospa 135 mg without prescription, depending on the level and extent of injury muscle relaxant yellow pill v order 135 mg colospa amex, may be compromised from a ventilatory and hemodynamic standpoint, and immediate control of these parameters is crucial. A detailed neurologic examination is critical to establish the operative plan and subsequent prognostication. Airway management in cervical spinal injury focuses on maintaining in-line stabilization throughout, and may require the use of fiberoptic intubation or other adjuncts to secure the airway. In a stable patient, radiographic studies are helpful in assessing the degree of cervical injury and options for intubation. Succinylcholine is safe in the initial 24 hours following spinal cord injury as new junctional and extrajunctional nicotinic receptors have not yet been fully expressed. In addition to intravenous fluids and blood products, vasopressors and inotropes are often required to support the blood pressure as hypotension and anemia can contribute to secondary injury of the spinal cord. Arterial blood pressure monitoring and large-bore intravenous access (preferably central venous access) are required. Corticosteroids have received particular attention in this regard, both in animal and human studies. The mechanism to account for their potential neuroprotective effect is largely unknown, but thought to include reduction of vasogenic edema, improvement of spinal cord perfusion, anti-inflammatory effects, and free radical scavenging. These studies were highly suspect, however, in that their results were not reproducible, their populations were skewed, and survival or quality of life did not improve with the intervention (methylprednisolone). Currently, both the American Association of Neurological Surgeons and Congress of Neurological Surgeons do not 2535 recommend the use of high-dose steroids in patients with acute spinal cord injury. Complex spine surgery, which often involves multiple level fusions and osteotomies, should also take into account the real possibility of significant, and sometimes profound, surgical bleeding and the need for postoperative mechanical ventilation following massive transfusion. Measurements of arterial blood gas, coagulation parameters, hemoglobin concentration, and platelet counts should be undertaken very frequently, as coagulopathy and anemia are quite common and need to be corrected rapidly as they can contribute to secondary injury. Close communication with the surgeon is very important, as these large operations often may benefit from early closure and staging of the procedure. Use of antifibrinolytics, such as tranexamic acid or aminocaproic acid, can decrease risk of bleeding with minimal, if any, increased risk for thrombotic complications. Complications of Anesthesia for Spine Surgery Fortunately, complications specifically related to anesthesia for spine surgery are rare, but they are often devastating when they occur. Risk factors include male sex, obesity, use of the Wilson frame, longer surgery and anesthesia duration, and high estimated blood loss, whereas use of colloid may be protective. This syndrome is caused by sustained hypoperfusion of the anterior spinal artery, owing to either surgical distraction or hypotension, and leads to motor weakness. The pathophysiology of this phenomenon is thought to be due to a disruption of descending inhibitory tracts with intact sympathetic reflex arcs below the level of injury. Recommended vasodilators include calcium-channel blockers, nitrates, or hydralazine. Spinal anesthesia had the advantage over epidural anesthesia as it is generally a denser block and does not risk sparing of sacral segments that may occur with epidural anesthesia. If general anesthesia is used, succinylcholine should generally be avoided as it may trigger a profound hyperkalemic response. Conclusion 2537 The perioperative care of neurosurgical patients requires a sound understanding of neurophysiologic and neuropharmacologic principles, the timely application of these principles, and vigilance to often rapidly changing clinical conditions. At the core of neuroanesthesia practice are the ideas of maintaining cerebral oxygen and substrate delivery, facilitating intraoperative neuromonitoring, and assuring for a rapid emergence to facilitate neurologic examination in appropriate patients. Expert application of the requisite knowledge to achieve these goals, along with efficient resource utilization, will provide the safest neurologic outcome possible for this vulnerable patient population. Probabilistic map of critical functional regions of the human cerebral cortex: Broca’s area revisited. Multiplicity of cerebrospinal fluid functions: new challenges in health and disease. Effect of hypoxia and hyperoxia on cerebral blood flow, blood oxygenation, and oxidative metabolism. Regional blood flow in the normal and ischemic brain is controlled by arteriolar smooth muscle cell contractility and not by capillary pericytes. Coupling between regional blood flow and oxygen utilization in the normal human brain: a study with positron tomography and oxygen 15. Cerebral perfusion under pressure: is the autoregulatory ‘plateau’ a level playing field for all?
Buy colospa 135 mg low cost
It is an intraven- may be used as an alternative to mechanical bear- tricular axial-fow pump featuring an outfow ings to achieve a durable spasms multiple sclerosis discount colospa express, “wearless” design spasms in neck best order for colospa. Te impeller that is contact-free may theoretically pump consists of a pedestal spasms hip buy cheap colospa 135 mg online, a pump body motor operate for longer periods without the failures assembly, and an outfow cannula with an inter- typically seen of its mechanical bearing counter- nal vane difuser. Te C-Pump® partial assist increased and ergonomics began to play a more device (formerly known as the CircuLite® System) prominent role in device design. Journal of Heart and Lung Transplant 32:675–683 Strueber M (2010) Initial clinical experience with a 6. Tese landmark cases were the frst ever of opment since 1988 named as MicroMed DeBakey implantable rotary blood pumps to support long- (MicroMed Cardiovascular Inc. Noon in ting in the pediatric chest without modifying the animal experiments at Texas A&M University in pump’s core components. Te impeller operational range inducer-impeller with six blades and a fow dif- is 7500–12,500 rpm that is able to generate fows fuser with other six blades for the outlet, which up to 6 l/min against a 100 mmHg pressure gradi- function as rear bearing support for the impeller. Te principal technical features that diverge Te difuser also helps to increase outfow pres- from most devices in the market is given by its sure by directing the fow in the axial direction. Tis had led to sion was upgraded with 8 magnets stator with- a pump more responsive to changes in the pres- out changes in volume occupied. Tis also led a sure diferential across the pump, due to changes reduction in power consumption. Numerical simulation and measurement Te inlet cannula is also made of titanium of platelet activation rates in recirculation fow and is inserted into the lef ventricular apex. Michael has a fow straightener with three blades at infow DeBakey directed the engineering team to design 572 A. Te fow probe could accurately and proprietary testing systems has allowed to measure the fow inside the outfow graf, and this refne the technology of the impeller, working technology has been called “true fow. Patients may feel pre- maturely full when they eat because an implant below the diaphragm can cause pressure on the stomach. Tis is an extremely the physician could control remotely the all the reliable tool for the detection of cardiac arrhythmias information. Te controller displays device main parameters humanitarian exemption from 2005 in children such as pump fow (L/min), power consumption 5–16 years of age with end-stage heart failure (watts), pump speed (rpm), and battery charge. A pump holder ring is sewed with 8–12 U Anticoagulation management for patients with pledgeted stitches on the lef ventricular apex. Te surgeon must pay are coated with Carmeda® BioActive and prelimi- attention during this procedure to ensure a full- nary data report encouraging result on preventions thickness incision and detaching of the muscle in of thromboembolic events; however, new data the apex to allow a perfect ft of the infow cannula on this issue are still needed. Together with the anticoagula- Te infow cannula is then secured by sewing the tion therapy should be introduced an antiplatelet infow cannula ring to the previous apical fxation therapy; this has been proved to reduce risk of ring. Panel a, handle temporary fxation of apical sewing cal view ring and fast connect device. Nevertheless, in adult patients, the lef thoracotomy (4th–5th intercostal space) allows the surgeon to a better view of the lef apex, and the outfow graf can be anastomosed to the descend- ing aorta. A lef mini-thoracotomy (4th–5th intercostal space) may be performed for lef ventricle apex exposure. Te outfow cannula anastomosis is instead per- formed through a right mini-thoracotomy or a J-shaped upper mini-sternotomy. Additionally, this ofers the chance to remove the cable in case of driveline wound infection with- be performed also on beating heart. However, adverse from the probe to the controller and the other events such as infections, thromboembolic com- transferring power from the controller to the plications, and technical failures limited their use pump motor. Te recently introduced With the HeartAssist Remote™ Monitoring axial-fow devices (e. Tey also their heart health while enjoying life at home or show lower rate of both related complications and traveling. Goldstein [16] and colleagues helping to avoid unnecessary hospital admis- have reviewed 150 patients worldwide under- sions. From their review, 55% were either bridged lead to an efective deployment resulting in to transplantation or recovery or are ongoing, better use of the healthcare system’s resources. Patients with these devices could achieve a good theoretical, and, despite all potential clinical ben- quality of life afer discharge from the hospital. Te common elements are energy trans- and may decrease the number of unnecessary fer coils, sealed internal battery, tiny and efcient ambulatory visits, still a question remains unre- motor controller, power draw of just 5.
Discount colospa on line
The fraction of the drug removed from the blood passing through the liver is the hepatic extraction ratio spasms throughout body generic colospa 135 mg with mastercard, E: where Ca is the mixed hepatic arterial–portal venous drug concentration and Cv is the mixed hepatic venous drug concentration spasms when i pee buy colospa 135 mg fast delivery. Therefore spasms after eating purchase colospa with visa, hepatic clearance is a function of hepatic blood flow and the ability of the liver to extract drug from the blood. The ability to extract drug depends on the activity of drug-metabolizing enzymes and the capacity for hepatobiliary excretion—the intrinsic clearance of the liver (Cli). Intrinsic clearance represents the ability of the liver to remove drug from the blood in the absence of any limitations imposed by blood flow or drug binding. The relationship of total hepatic drug clearance to the extraction ratio and intrinsic clearance, Cli, is: The right-hand side of Equation 11-3 indicates that if intrinsic clearance is very high (many times larger than hepatic blood flow, Cli Q), total hepatic clearance approaches hepatic blood flow. On the other hand, if intrinsic clearance is very small (Q + Cli ≈ Q), hepatic clearance will be similar to intrinsic clearance. Thus, hepatic drug clearance and extraction are determined by two independent variables, intrinsic clearance and hepatic blood flow. However, the extent of the change depends on the initial relationship between intrinsic clearance and hepatic blood flow, according to the nonlinear relationship: If the initial intrinsic clearance is small relative to hepatic blood flow, then the extraction ratio is also small, and Equation 11-4 reduces to the following 664 relationship: Equation 11-4a indicates that doubling intrinsic clearance will produce an almost proportional increment in the extraction ratio, and, consequently, hepatic elimination clearance (Fig. However, if intrinsic clearance is much greater than hepatic blood flow, Equation 11-4 reduces to the following relationship: Figure 11-1 The relationship between hepatic extraction ratio (E, right y-axis), intrinsic clearance (Cl ,i x-axis), and hepatic clearance (Cl ,H left y-axis) at the normal hepatic blood flow (Q) of 1. For drugs with a high intrinsic clearance (Cli Q), increasing intrinsic, clearance has little effect on hepatic extraction, and total hepatic clearance approaches hepatic blood flow. In contrast, if the intrinsic clearance is small (Cli ≤ Q), the extraction ratio is similar to the intrinsic clearance (inset). In nonmathematical terms, high intrinsic clearance indicates efficient hepatic elimination. It is hard to enhance an already efficient process, whereas it is relatively easy to improve on inefficient drug clearance because of low intrinsic clearance. When the intrinsic clearance is low, hepatic elimination clearance is independent of liver blood flow—the drug elimination is limited by the capacity of the liver to metabolize the drug (i. In contrast, as intrinsic clearance increases, the hepatic elimination becomes more dependent on hepatic blood flow—the liver is able to metabolize all of the drug that it is exposed to and therefore only limited by the amount of drug that is delivered to the liver (i. For drugs with a high extraction ratio and a high intrinsic clearance, hepatic elimination clearance is directly proportional to hepatic blood flow. Therefore, any manipulation of hepatic blood flow will be directly reflected by a proportional change in hepatic elimination clearance (Fig. In contrast, when the intrinsic clearance is low, changes in hepatic blood flow produce inversely proportional changes in extraction ratio (Fig. Therefore, classifying drugs as having either low, intermediate, or high extraction ratios (Table 11-3), allows predictions to be made on how intrinsic hepatic clearance and hepatic blood flow affect hepatic elimination clearance. This allows gross adjustments to be made in hepatically metabolized drug dosing to avoid excess accumulation of drugs (decreased hepatic elimination without dose adjustment) or subtherapeutic dosing strategies (increased hepatic elimination without dose adjustment). When the intrinsic clearance is low, increases in hepatic blood flows cause a decrease in the extraction ratio because the liver has limited metabolic capabilities. In contrast, when the intrinsic clearance is high, the extraction ratio is essentially independent of hepatic blood flow because the liver’s ability to eliminate drug is well above the amount of drug provided by normal hepatic blood flow. Table 11-3 Classification of Drugs Encountered in Anesthesiology According to Hepatic Extraction Ratios Pharmacologic and pathologic manipulations of cardiac output, with its consequences on hepatic/splanchnic blood flow and renal blood flow, are important covariates when designing drug dosing strategies. Although the blood is rarely the site of action of drug effect, the tissue drug concentration of an individual organ is a function of the blood flow to the organ, the concentration of drug in the arterial inflow of the organ, the capacity of the organ to take up drug, and the diffusivity of the drug between the blood and the organ. In these models, body tissues are lumped4 into groups that have similar distribution of cardiac output and capacity for drug uptake. Highly perfused tissues with a large amount of blood flow per volume of tissue are classified as the vessel rich group, whereas tissues with a balanced amount of blood flow per volume of tissue are classified as the lean tissue group or fast tissue group. The vessel-poor group (slow tissue group) are comprised of tissues that have a large capacity for drug uptake but a limited tissue perfusion. Although identification of the exact organs that make up each tissue group is not possible from the mathematical model, it is apparent that the highly perfused tissues are composed of the brain, lungs, kidneys, and a subset of muscle; the fast equilibrating tissue would be consistent with the majority of muscle and some of the splanchnic bed (e. Based on these computationally and experimentally intense physiologic models, Price4,18 was able to demonstrate that awakening after a single dose of thiopental was primarily a result of redistribution of thiopental from the brain to the muscle with little contribution by distribution to less well- perfused tissues or drug metabolism. This fundamental concept of redistribution applies to all lipophilic drugs and was not delineated until an accurate pharmacokinetic model had been constructed.
Eusebio, 39 years: Rotation of the neck away from the side and thyroid gland between the levels of the inferior thyroid of swelling causes severe pain from tension on the ipsilateral artery and the oblique line of the thyroid cartilage. J Heart Lung Transplant 30(1):64–69 a further operation, we explanted the driveline only 8. Fenoldopam mesylate blocks reductions in renal plasma flow after radiocontrast dye infusion: a pilot trial in the prevention of contrast nephropathy. Depth perception is mance time and error rates in surgical tasks for both resident thought to be critical to precise motor movement.
Diego, 57 years: With the no touch technique, emergence from inhalational anesthesia follows three distinct phases: early, middle, and late. Patients with C1 esterase inhibitor deficiency can develop severe angioneurotic edema after even slight trauma to the airway. Contraindications There are no absolute contraindications to temperature monitoring. Coadministration of opioids with central neuraxial52 local anesthetics results in synergistic analgesia.
Pyran, 36 years: Te authors conclude that inhaled vasodila- as adjuncts when systemic vasopressor support is tors mainly afected the pulmonary vasculature. With the use of such dyes, melting curve analysis will help to discriminate specific products from other contaminants [2 ]. Prevention of succinylcholine- induced fasciculation and myalgia: a meta-analysis of randomized trials. Emergence after a prolonged infusion of ketamine, especially when combined with opioids and benzodiazepines, may be delayed.
Rune, 27 years: Despite these compensatory fac Monocular endoscopes create a two-dimensional (2D) im tors, 2D visualization does not match the depth perception age that impairs the surgeon’s perception of depth, spatial aforded by binocular cues, including vergence, stereopsis, relations, and the size of the anatomical structures. Because most ophthalmic surgical procedures are elective, should an enhanced risk of perioperative movement be noted during the preoperative assessment, the prudent course may be to postpone surgery until the patient is in optimal condition to remain relatively still or to perform the procedure under66 general anesthesia. Interestingly, 19 years later, a post hoc analysis of this study identifed that 5. Perioperative anaesthetic morbidity in children: A database of 24,165 anaesthetics over a 30-month period.
Tippler, 23 years: Comparable postoperative pulmonary atelectasis in patients given 30% or 80% oxygen during and 2 hours after colon resection. Permanent postoperative vision loss associated with expansion of intraocular gas in the presence of a nitrous oxide- 3501 containing anesthetic. How many proteins have hydrophobic pockets in which anesthetics can bind at clinically relevant concentrations? The major side effects are a high incidence of nausea51 and vomiting, maternal sedation, dose-related depression of ventilation, orthostatic hypotension, and the potential for neonatal depression.
Farmon, 45 years: If the biopsy contains urease, the change first appears around the sample and eventually colors all of the gel. All caregivers, including anesthesiologists, should be knowledgeable of at least some aspects of aging in order to provide intelligent deviation from their standard practice. Using the large femoral artery as a landmark may be beneficial to more distal approaches where the nerve lies adjacent to the smaller saphenous branch of the descending genicular artery (see text). Dexmedetomidine pharmacokinetics are not significantly different in patients with severe renal impairment compared to healthy subjects.
Benito, 47 years: The arterial wall is gaping open, suppressive protocols resulting in severe perirenal hemorrhage. As with the antisialagogues, the effects of this medication are not immediate and it is often administered in the preoperative waiting area. This system depends in part on patient complaints for both enforcement and policy evolution. By 4 years of age, the sinus reaches the infraorbital the sinus foor to the root tips of the teeth is longest for the canal and continues laterally.
Pakwan, 55 years: The bright spot may be absent adenomas, particularly in the setting of Cushing’s disease. Lo and Kai Man Kam Introduction Molecular techniques for identifying and detecting microorganisms have been proven readily adaptable for use in the clinical diagnostic laboratory. Hypertensive patients who have left29 ventricular hypertrophy and are undergoing noncardiac surgery are at a higher perioperative risk than nonhypertensive patients. The posterior gland may also be distinguished from anterior lobe rounds the pituitary stalk to form the pars tuberalis.
Flint, 61 years: Oxidation of xenobiotics requires oxygen, but reductive biotransformation is inhibited by oxygen, so it is facilitated when the intracellular oxygen tension is low. Most of publication did euvolemia, and support of end-organ function is not provide exact criteria for weaning start. Traditionally, such patients have been left intubated throughout the duration of their open abdomen. One must be cognizant of the potential to compound existing neurologic deficits; therefore, clear documentation of the deficits prior to the procedure and a careful discussion of the potential risks and benefits are critical.
Mamuk, 37 years: In comparing the microscopic versus the endoscopic approach, epistaxis decreased from 1. An implantable abdominal vagal nerve stimulator is placed laparoscopically and emits electrical impulses to control gastric emptying and signal the satiety center in the brain. Required doses to induce cardiovascular collapse were greater for lidocaine (127 mg/kg) compared to ropivacaine (42 mg/kg), levobupivacaine (27 mg/kg), and bupivacaine (22 mg/kg). In the superficial laminae of the dorsal horn, local neuronal circuits process both ascending and descending pain pathways and are regulated by local endogenous opioid circuits.
Seruk, 52 years: Automation has improved the practice of blood culture enormously in terms of timely report of positive culture and more laboratory efficiency, and consequently better patient care. Pregnancy increases median nerve sensitivity to lidocaine block and in vitro27 preparations from pregnant animals demonstrate increased susceptibility to local anesthetic blockade. Gut ischemia, oxida- tive stress, and bacterial translocation in elevated abdominal pressure in rats. Elective surgery in an unstable metabolic state is not recommended (see “Emergencies”).
Vandorn, 31 years: However, mas tend to be more aggressive lesions and may invade into most are macroadenomas with no specifc localization. This suture should hold the dressing in position roll or folded petroleum gauze can be secured in the concha fossa and eliminate the dead space between the anterior and posterior in the following fashion. The whole inner surface of the mandible as well as its processes serve as an attachment area for masticatory muscles. Amplify by turnover of the chosen substrate, a single enzyme label can convert >107 mole- cules per minute, a millionfold increase.
8 of 10 - Review by S. Goose
Votes: 318 votes
Total customer reviews: 318
References
- Centers for Disease Control and Prevention (CDC). Intensive-care patients with severe novel influenza A (H1N1) virus infection - Michigan, June 2009.
- Watarai M, Yazawa M, Yamanda K, Yamamoto H, Yamazaki Y. Pulmonary sarcoidosis with associated bloody pleurisy. Intern Med 2002;41:1021-3.
- Ravanti L, Kahari VM: Matrix metalloproteinases in wound repair, Int J Mol Med 6:391n407, 2000.
- Russell TR, Donahue JH. Hemorrhoid banding. A warning. Dis Colon Rectum. 1985;28:291-293.
- Coin A, Sergi G, Marin S, et al. Predictors of low bone mineral density in elderly males with chronic obstructive pulmonary disease: the role of body mass index. Aging Male 2010; 13: 142-147.
- Kerr DJ, Gray R, McConkey C, et al. Adjuvant chemotherapy with 5-fluorouracil, L-folinic acid and levamisole for patients with colorectal cancer: non-randomised comparison of weekly versus four-weekly schedules-less pain, same gain. QUASAR Colorectal Cancer Study Group. Ann Oncol 2000;11(8):947-955.
- Weir, R., Browne, G. B., Tunks, E., Gafni, A., & Roberts, J. (1992). A profile of users of specialty pain clinic services: predictors of use and cost estimates. Journal of Clinical Epidemiology, 45(12), 1399n1415.
- Lin DW, Santucci RA, Mayo ME, et al: Urodynamic evaluation and long-term results of the orthotopic gastric neobladder in men, J Urol 164(2):356n359, 2000.