Vicki E. Nagano, MD
- Department of Nuclear Medicine
- Kaiser Sacramento
- Sacramento, California
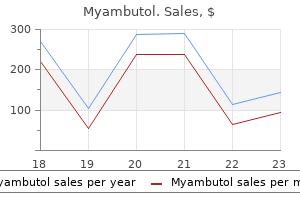
Myambutol dosages: 800 mg, 600 mg, 400 mg
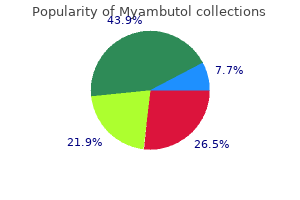
Myambutol packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Purchase myambutol once a day
The initial alpha phase reflects rapid distribution in blood and highly perfused organs (eg antibiotic resistance upec myambutol 600 mg buy amex, brain virus news myambutol 400 mg purchase mastercard, liver global antibiotic resistance journal 600 mg myambutol order overnight delivery, heart, kidney), characterized by a steep exponential decline in concentration. This is followed by a slower declining beta phase reflecting distribution into less well perfused tissue (eg, muscle, gut), and may assume a nearly linear rate of decline. The potential toxicity of the local anesthetics is affected by the protective effect afforded by uptake by the lungs, which serve to attenuate the arterial concentration, though the time course and magnitude of this effect have not been adequately characterized. Metabolism and Excretion The local anesthetics are converted to more water-soluble metabolites in the liver (amide type) or in plasma (ester type), which are excreted in the urine. Since local anesthetics in the uncharged form diffuse readily through lipid membranes, little or no urinary excretion of the neutral form occurs. Acidification of urine promotes ionization of the tertiary amine base to the more water-soluble charged form, leading to more rapid elimination. Ester-type local anesthetics are hydrolyzed very rapidly in the blood by circulating butyrylcholinesterase to inactive metabolites. However, excessive concentrations may accumulate in patients with reduced or absent plasma hydrolysis secondary to atypical plasma cholinesterase. The amide local anesthetics undergo complex biotransformation in the liver, which includes hydroxylation and N- dealkylation by liver microsomal cytochrome P450 isozymes. There is considerable variation in the rate of liver metabolism of individual amide compounds, with prilocaine (fastest) > lidocaine > mepivacaine > ropivacaine ≈ bupivacaine and levobupivacaine (slowest). As a result, toxicity from amide-type local anesthetics is more likely to occur in patients with hepatic disease. Many other drugs used in anesthesia are metabolized by the same P450 isozymes, and concomitant administration of these competing drugs may slow the hepatic metabolism of the local anesthetics. Decreased hepatic elimination of local anesthetics would also be anticipated in patients with reduced hepatic blood flow. For example, the hepatic elimination of lidocaine in patients anesthetized with volatile anesthetics (which reduce liver blood flow) is slower than in patients anesthetized with intravenous anesthetic techniques. Delayed metabolism due to impaired hepatic blood flow may likewise occur in patients with congestive heart failure. Membrane potential—The primary mechanism of action of local anesthetics is blockade of voltage-gated sodium channels (Figure 26–1). The excitable membrane of nerve axons, like the membrane of cardiac muscle (see Chapter 14) and neuronal cell bodies (see Chapter 21), maintains a resting transmembrane potential of –90 to –60 mV. During excitation, the sodium channels open, and a fast, inward sodium current quickly depolarizes the membrane toward the sodium equilibrium potential (+40 mV). As a result of this depolarization process, the sodium channels close (inactivate) and potassium channels open. The outward flow of potassium repolarizes the membrane toward the potassium equilibrium potential (about –95 mV); repolarization returns the sodium channels to the rested state with a characteristic recovery time that determines the refractory period. These ionic fluxes are similar to , but simpler than, those in heart muscle, and local anesthetics have similar effects in both tissues. Sodium channel isoforms—Each sodium channel consists of a single alpha subunit containing a central ion-conducting pore associated with accessory beta subunits. The pore-forming alpha subunit is actually sufficient for functional expression, but the kinetics and voltage dependence of channel gating are modified by the beta subunit. A variety of different sodium channels have been characterized by electrophysiologic recording, and subsequently isolated and cloned, while mutational analysis has allowed for identification of the essential components of the local anesthetic binding site. Nine members of a mammalian family of sodium channels have been so characterized and classified as Na 1. Channel blockade—Biologic toxins such as batrachotoxin, aconitine, veratridine, and some scorpion venoms bind to receptors within the channel and prevent inactivation. This results in prolonged influx of sodium through the channel and depolarization of the resting potential. However, in contrast to the local anesthetics, their binding site is located near the extracellular surface.
Buy myambutol paypal
Using linear pharmacokinetics antibiotic resistance of e.coli 800 mg myambutol order visa, the resulting total steady-state ethosuximide serum concentration would equal Dnew = (Cssnew/Cssold) Dold = (90 μg/mL / 55 μg/mL) 700 mg/d = 1145 mg/d antimicrobial mouthwashes generic myambutol 800 mg mastercard, rounded to 1100 mg/d or 550 mg every 12 hours epstein-barr virus 800 mg myambutol purchase. A steady-state trough total ethosuximide serum concentration should be measured after steady state is attained in 1–2 weeks. Ethosuximide serum concentrations should also be measured if the patient experiences an exacerbation of their epilepsy, or if the patient develops potential signs or symptoms of ethosuximide toxicity. Ethosuximide clearance can be computed using a steady-state ethosuximide concen- tration: Cl = [F(D/τ)] / Css = [1(350 mg/12 h)] / (55 mg/L) = 0. A steady-state trough total ethosuximide serum concentration should be measured after steady state is attained in 1–2 weeks. Ethosuximide serum concentrations should also be measured if the patient experiences an exacerbation of their epilepsy, or if the patient develops potential signs or symptoms of ethosuximide toxicity. Enter patient’s demographic, drug dosing, and serum concentration/time data into the computer program. The pharmacokinetic parameters computed by the program are a volume of distri- bution of 25 L, a half-life equal to 36 h, and a clearance equal to 0. The one-compartment model first-order absorption equations used by the program to compute doses indicates that a dose of 600 mg every 12 hours will produce a steady-state ethosuximide concentration of 95 μg/mL. Estimate clearance and volume of distribution according to disease states and con- ditions present in the patient. Once the correct clearance and volume of distribution estimates are identified for the patient, they can be converted into the ethosuximide half-life (t1/2) and elimination rate constant (k) estimates using the following equations: t1/2 = (0. A steady-state trough ethosuximide serum concentration should be measured after steady state is attained in 3–5 half-lives. Since the patient is expected to have a half- life equal to 40 hours, the ethosuximide steady-state concentration could be obtained any time after the sixth day of dosing (5 half-lives = 5 ⋅ 40 h = 200 h or 8 d). Ethosux- imide serum concentrations should also be measured if the patient experiences an exacerbation of their epilepsy, or if the patient develops potential signs or symptoms of ethosuximide toxicity. The suggested initial maintenance dosage rate for ethosuximide in an older patient is 15 mg/kg/d: 60 kg ⋅ 15 mg/kg/d = 900 mg/d, rounded to 1000 mg daily. This dose would be titrated upward in 3–7 mg/kg/d increments every 1–2 weeks while monitoring for adverse and therapeutic effects. A steady-state trough total ethosuximide serum concentration should be measured after steady state is attained in 1–2 weeks. Ethosuximide serum concentrations should also be measured if the patient experiences an exacerbation of their epilepsy, or if the patient develops potential signs or symptoms of ethosuximide toxicity. Using linear pharmacokinetics, the resulting total steady-state ethosuximide serum concentration would equal Dnew = (Cssnew/Cssold) Dold = (60 μg/mL / 40 μg/mL) 1000 mg/d = 1500 mg/d, or 750 mg every 12 hours. A steady-state trough total ethosuximide serum concentration should be measured after steady state is attained in 1–2 weeks. Ethosuximide serum concentrations should also be measured if the patient experiences an exacerbation of their epilepsy, or if the patient develops potential signs or symptoms of ethosuximide toxicity. A steady-state trough total ethosuximide serum concentration should be measured after steady state is attained in 1–2 weeks. Ethosuximide serum concentrations should also be measured if the patient experiences an exacerbation of their epilepsy, or if the patient develops potential signs or symptoms of ethosuximide toxicity. Enter patient’s demographic, drug dosing, and serum concentration/time data into the computer program. The pharmacokinetic parameters computed by the program are a volume of distri- bution of 42 L, a half-life equal to 32 h, and a clearance equal to 0. The one-compartment model first-order absorption equations used by the program to compute doses indicates that a dose of 750 mg every 12 hours will produce a steady-state ethosuximide concentration of 61 μg/mL. Enter patient’s demographic, drug dosing, and serum concentration/time data into the computer program. The pharmacokinetic parameters computed by the program are a volume of distri- bution of 48 L, a half-life equal to 29 h, and a clearance equal to 1. The one-compartment model first-order absorption equations used by the program to compute doses indicates that a dose of 1750 mg every 24 hours will produce a steady-state ethosuximide concentration of 48 μg/mL. To avoid possible gastroin- testinal side effects, this daily dose should be given in as a divided dose of 750 mg in the morning and 1000 mg in the evening. Enter patient’s demographic, drug dosing, and serum concentration/time data into the computer program.
Buy myambutol 400 mg cheap
The most likely explanation of these aches has begun on therapy with Topamax as prophy- fndings relates to which of the following medications? Which of the following would be important (B) Hydrochlorothiazide coexisting conditions to know about? While in Thailand virus scan order myambutol 600 mg mastercard, (B) Location 2 he enjoyed the local cuisine including many meals of (C) Location 3 raw sushi antimicrobial additive for plastic order discount myambutol on line. The physician wants to treat the patient (D) Location 4 right away to prevent the development of cholangio- carcinoma bacteria uti myambutol 600 mg order on line. The surgeon begins (D) Pyrantel pamoate once she has lost her eyelash refex and her breathing (E) Sodium stibogluconate pattern became regular. The patient does remember being warned of (E) Stage V reduviid bugs and that their bites are painless. What is the most ap- (D) Solubility propriate treatment for the dormant form of the para- site in the liver? He presents to his primary (B) Clindamycin care physician complaining of loss of libido, delayed (C) Metronidazole ejaculation, and occasional inability to ejaculate. Her anesthesia is induced initially with an (D) Referral for outpatient sexual therapy inhaled, nonfammable anesthetic that contains no (E) Stop paroxetine and begin bupropion halogenated carbons. Bethanechol is used to infusion increases the likelihood that the patient will stimulate the atonic bladder, particularly in postpar- develop hand–foot syndrome. Prostaglandins lost in the urine when high amounts of sodium pass from surface mucous cells and somatostatin from D cells through the distal convoluted tubule (as is the case directly inhibit acid secretion. Ranitidine is an H2- with potassium-wasting diuretics) because of a receptor antagonist, meaning it blocks the proacid effect sodium-potassium exchange pump on the distal of endogenous histamine. It decreases acid by mimicking the inhibitory causing preformed aquaporins to be inserted on the effect of endogenous prostaglandins. However, this drug is effects to be aware of including red eye and excessive also metabolized through the biliary system of the liver hair growth of eyelashes. Palmar–plantar erythrodysesthesia, or hand– perfused tissues rapidly attain a steady state with the foot syndrome, is a common reaction with many chemo- partial pressure of anesthetic in the blood. This, unclear, but excessive friction (as with walking and and the fact that they have a large volume, prolongs working with hands) and high temperatures seem to the time required to achieve steady state. However, disorder, and fuoxetine is approved to treat child- like the other halogenated gases, it produces dose- hood depression. It has a pungent odor and stimulates respiratory only treat obsessive-compulsive disorder in this refexes (e. The antipsy- 9 The answer is C: A 62-year-old man with a history of chotics are considered to be the only effcacious treat- four-vessel coronary artery bypass. Not all patients respond, and a history of cardiac disease is at greatest risk of anes- complete normalization of behavior is seldom achieved. A greater proportion of who are resistant to the traditional agents, especially in any given drug will enter the cerebral circulation treating the negative symptoms of schizophrenia under these circumstances. As a result, the dose of (social withdrawal, blunted emotions, ambivalence, induction drug must be reduced. However, this tive symptom of schizophrenia and does not usually patient is a healthy marathon runner and is likely improve with frst-line therapy. Plasma levels decline analgesics for treatment of chronic pain with severe rapidly as a result of redistribution, followed by a anxiety. The initial redistribution half-life is ment of the motor and phonic tics of Tourette disor- between 2 and 4 min. Data are limited as to its effcacy in treating diarrhea, and it is usually only used in refrac- 15 The answer is C: Inhibits 5-a-reductase. Of the choices listed, angina is the most status was caused by high levels of ammonia in his common condition to coexist with hypertension. Normally, the liver converts excess ammonia (B) Asthma is the least common coexisting condition into water-soluble urea to be excreted by the kidneys; with hypertension. Once it arrives in the colon, however, it is converted to various organic 17 The answer is D: Inhibitor of myenteric plexus activity. Loperamide is an opioid-receptor agonist but does Ammonia that diffuses into the colon is converted to not affect the central nervous system. This patient’s problem is that he can- The cause is either increased production or decreased not make urea. If necessary, drug therapy includes niacin and/ on the speed at which his liver can produce urea from or fenofbrate or a statin.
Myambutol 600 mg order overnight delivery
It is a potent antagonist at autonomic ganglia and to ventilate the paralysed patient’s lungs bacteria 1000x myambutol 800 mg purchase amex, recovery may causes significant hypotension antimicrobial towels martha stewart purchase myambutol on line. It benefits some cases ase and so its persistence in the body is increased by neostig- of trigeminal neuralgia antibiotic used for urinary tract infection buy myambutol 600 mg online. Anaphylactic reactions are caused by the interaction of anti- Repeated injections of suxamethonium can cause brady- gens with specific immunoglobulin (Ig) E antibodies, cardia, extrasystoles and even ventricular arrest. These are which have been formed by previous exposure to the anti- probably due to activation of cholinoceptors in the heart gen. It can be used in Caesarean from anaphylaxis but are not caused by previous exposure section as it does not cross the placenta readily. Intravenous nium depolarisation causes a release of potassium from anaesthetics and muscle relaxants can cause anaphylactic muscle, which in normal patients will increase the plasma or anaphylactoid reactions; rarely, they are fatal. This is a problem only if the pa- laxants are responsible for 70% of anaphylactic reactions tient’s plasma potassium concentration was already high, during anaesthesia, and suxamethonium accounts for for example in acute renal failure. The latter had long been Only those who are competent at tracheal intubation and interested in the problem of local anaesthesia in the eye, for ventilation of the patient’s lungs should use these drugs. The drugs are used: Observing that numbness of the mouth occurred after taking cocaine orally, Koller realised that this was a local • to provide muscular relaxation during surgery, to anaesthetic effect. He tried cocaine on animals’ eyes and enable intubation in the emergency department, and introduced it into clinical ophthalmological practice, while occasionally to assist mechanical ventilation in Freud was on holiday. The use of cocaine spread rapidly intensive therapy units; and and it was soon being used to block nerve trunks. Chemists • during electroconvulsive therapy to prevent injury to then began to search for less toxic substitutes, with the re- the patient from excessive muscular contraction. Other muscle relaxants Desired properties Drugs that reduce spasm of the voluntary muscles without Innumerable compounds have local anaesthetic proper- impairing voluntary movement can be useful in spastic ties, but few are suitable for clinical use. Useful substances states, low back syndrome and rheumatism with muscle must be water soluble, sterilisable by heat, have a rapid spasm. Baclofen reduces spasticity and flexor spasms, but, as it has no action on voluntary muscle power, function is com- Mode of action monly not improved. Ambulant patients may need their leg spasticity to provide support, and reduction of spasticity Local anaesthetics prevent the initiation and propagation of the nerve impulse (action potential). By reducing the 9 passage of sodium through voltage-gated sodium ion chan- There are wide inter-ethnic differences. When cases are discovered the family should be investigated for low plasma cholinesterase activity and nels they raise the threshold of excitability; in consequence, affected individuals warned. The fibres in nerve trunks Prolongation of action by are affected in order of size, the smallest (autonomic, sen- vasoconstrictors sory) first, probably because they have a proportionately greater surface area, and then the larger (motor) fibres. The addition of a vasocon- strictor such as adrenaline/epinephrine reduces local The distribution rate of a single dose of a local anaesthetic blood flow, slows the rate of absorption of the local anaes- is determined by diffusion into tissues with concentra- thetic, and prolongs its effect; the duration of action of li- tions approximately in relation to blood flow (plasma docaine is doubled from 1 h to 2 h. By injection or infiltration, concentration of adrenaline/epinephrine should be 1 in local anaesthetics are usually effective within 5 min 200 000, although dentists use up to 1 in 80 000. Enough adrenaline/epinephrine can be absorbed to (usually the hydrochloride) dissociates in the tissues to lib- affect the heart and circulation, and reduce the plasma po- erate the free base, which is biologically active. An alternative vasoconstrictor is felypressin Absorption from mucous membranes on topical applica- (synthetic vasopressin), which, in the concentrations used, tion varies according to the compound. Those that are well does not affect the heart rate or blood pressure and may absorbed are used as surface anaesthetics (cocaine, lido- be preferable in patients with cardiovascular disease. Absorption of topically applied local an- aesthetic can be extremely rapid and give plasma concentrations comparable to those obtained by injection. Ab- anxiety, restlessness, tremors, euphoria, agitation and sorption is very slow and a cream is applied under an occlu- even convulsions, which are followed by depression. Uses Ester compounds (cocaine, procaine, tetracaine, benzo- caine) are hydrolysed by liver and plasma esterases, and Local anaesthesia is generally used when loss of conscio- their effects may be prolonged where there is a genetic en- usness is neither necessary nor desirable, and also as an zyme deficiency. It can be levobupivacaine, ropivacaine) are dealkylated in the used for major surgery, with sedation, although many liver. It is invaluable when Impaired liver function, whether caused by primary the operator must also be the anaesthetist, which is often cellular insufficiency or low liver blood flow as in cardiac the case in some parts of the developing world.
Purchase myambutol 800 mg visa
It is recommended as a second-line agent for the bundles of recommended control measures (see upper and lower respiratory tract infections including those p infection labs cheap myambutol 600 mg free shipping. Ithasbalancedrenalandhepaticexcretion Reversible arthropathy has developed in weight-bearing so dose modification in renal failure is not necessary virus medication purchase myambutol 800 mg otc. Rupture of tendons can antibiotics for uti make you tired myambutol 400 mg buy online, notably the Achilles, has oc- This group includes: curred, more commonly in the elderly and those taking • Metronidazole and tinidazole (antibacterial and corticosteroids concurrently. It is also effective at reducing rates of staphy- lococcal peritonitis in patients receiving chronic ambula- • Treatment of sepsis to which anaerobic organisms, e. Such • Amoebiasis (Entamoeba histolytica), including both strains may fail to be eradicated from the nares, but their intestinal and extra-intestinal infection. A topical gel preparation is useful for edible mushroom Clitopilus scyphoides, binds to a site on reducing the odour associated with anaerobic infection of the 50 S bacterial ribosomal subunit and is active against fungating tumours. For treatment furred tongue and an unpleasant metallic taste in the of infected eczema and similar conditions it is applied in a mouth; also headache, dizziness and ataxia. Rashes, urti- thin layer to the skin twice daily and covered with a sterile caria and angioedema occur. Systemic absorption is curs if treatment is prolonged and epileptiform seizures very low and the most commonly reported adverse reaction if the dose is high. It is sometimes used orally for bowel Tinidazole is similar to metronidazole in use and adverse decontamination, by inhalation via a saline nebuliser in effects, but has a longer t½ (13 h). It is excreted mainly patients with cystic fibrosis who are infected with Pseudo- unchanged in the urine. The longer duration of action of monas aeruginosa, and is applied to skin, including external 189 Section | 3 | Infection and inflammation ear infections. It is currently undergoing a renaissance with be monitored daily and the dose reduced to 12–18-hourly systemic use for severe infections with multiply resistant in patients with creatinine clearance <10–20 mL/min. Re- Gram-negative pathogens such as pseudomonads and Aci- cently published case series of parenteral use have reported netobacter when no alternative agents are available. The few problems of serious toxicity even in patients who re- usual dose is 1–2 million units 8-hourly. Its principal bination with intravenous colistin therapy), and it can use now is topical application for skin, eye and external be administered intrathecally. Penicillin allergy: how America, and the Society of Infectious and biochemical basis and clinical to diagnose and when to treat. This chapter considers the bacteria Usually, the infecting organism(s) is not known at the that cause disease in individual body systems, the drugs time of presentation and treatment must be instituted on that combat them, and how they are best used. Urgent sup- • Neonatal septicaemia is usually due to Lancefield port of the circulation and other organs is necessary for sur- Group B streptococcus or coliforms: benzylpenicillin vival, and rapid assessment by senior medical staff and plus gentamicin [vancomycin þ ceftazidime]. It is necessary to treat metastatic infection: patients with prolonged around 15 patients with antibiotic to cure one patient faster bacteraemia or who fail to settle promptly should be than the natural resolution rate. Judgement is re- anaerobes and coliforms: piperacillin-tazobactam þ quired as to whether any particular organism is acting as a clindamycin [meropenem þ clindamycin]. Choice of antibiotic should be guided by culture • Septicaemia in patients rendered neutropenic by and sensitivity testing; therapy may need to be prolonged. Amoxicillin or co- occasionally with skin and soft tissue infection and amoxiclav is satisfactory, but the clinical benefit of antibi- after packing of body cavities, such as the nose. Children under the tion with optimal circulatory and respiratory support and age of 2 years with bilateral otitis, and those with acute au- glycaemic control, and administration of hydrocortisone ral discharge (otorrhoea) benefit most from antibiotic and recombinant human activated protein C for severe treatment. Pneumococcal vaccination is modestly greatestin the first 2 years after splenectomy (but islifelong), effective at reducing recurrences in children who are prone in children, and in those with splenectomy for haematolo- to them. Patients must be immunised against ap- propriate pathogens and receive continuous low-dose oral prophylaxis with phenoxymethylpenicillin (penicillin V), or erythromycin in those allergic to penicillin. Prevention of complications is more important than relief of the symptoms, which seldom last long and corticosteroids Sinusitis are much more effective than antibiotics at shortening As oedema of the mucous membrane hinders the drainage the period of pain. Severe sporadic or epidemic sore throat is ing anaerobes, spirochaetes) responds readily to benzylpe- likely to be streptococcal and the risk of these complica- nicillin; a single i. Metronidazole 200 mg 8-hourly by mouth for lin-allergic), given, ideally, for 10 days, although compli- 3 days is also effective. Do not use amoxicillin if the circumstances cillin is also used, to prevent the production of more toxin. In needed in unvaccinated children whose defences are com- a closed community, chemoprophylaxis of unaffected peo- promised, have damaged lungs or are less than 3 years old.
Creatine. Myambutol.
- What is Creatine?
- Slowing an eye disease called gyrate atrophy.
- How does Creatine work?
- Increasing strength in people with muscle diseases such as muscular dystrophy.
- Improving the athletic performance of young, healthy people during brief, high-intensity exercise such as sprinting. However, it does not seem to help highly trained athletes. It also does not seem to help increase muscle strength or body composition.
- What other names is Creatine known by?
- Increasing strength and endurance in patients with heart failure.
- Are there any interactions with medications?
- Rheumatoid arthritis (RA).
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96843
Buy 600 mg myambutol fast delivery
It is ef- Osteoporosis fective in endometriosis through its negative feedback 63 Androgens antibiotic 3rd generation purchase genuine myambutol on-line, Antiandrogens antibiotic used for lyme disease 400 mg myambutol order with amex, and Anabolic Steroids 731 (Deca-Durabolin) virus cleanup discount 400 mg myambutol overnight delivery, methandrostenolone (Dianabol), drogen for any reason, facial hair growth may progress oxymetholone (Anadrol, Adroyd), stanozolol (Winstrol), to total body hair growth, baldness may develop, breasts and oxandrolone (Anavar). In addition, cli- The protein anabolic compounds are most com- toral hypertrophy, uterine atrophy, and menstrual irreg- monly used to stimulate appetite and muscle mass in ularities may develop. Although some of the symptoms persons with advanced malignancy or other conditions are reversible and disappear upon cessation of therapy, characterized by advanced malnutrition. These com- several effects—baldness, growth of facial hair, clitoral pounds are also often abused by athletes who are trying enlargement, and deepening of the voice—are com- to build muscle mass. Steroids taken by women during pounds at the same time (stacking) or sequentially to pregnancy may cause pseudohermaphroditism in the try to maximize their anabolic effects. Athletes who use these compounds in this way are unaware of the potential adverse effects or do Androgen administration to male or female adults, es- not care. Since androgens stimulate the ac- As a class, the androgens are relatively safe and non- tivity of sebaceous glands, oily skin and acne are found toxic. However, in inappropriate doses or for inappro- in some individuals who are receiving androgen ther- priate reasons, their use can result in significant toxicity. A change in cholesterol levels can result from an- drogen therapy, such as decreased levels of high-density Toxicity in Men lipoprotein cholesterol and increased levels of low- The administration of androgens to sexually mature hy- density lipoprotein cholesterol. Testosterone administration can cause irritability, agita- Oral androgen preparations that have the 17-methyl tion, or aggressive behavior. Cessation of exogenous androgen ated with the development of benign liver tumors and treatment in normal males usually results in restoration a rare liver disorder involving the development of of normal sperm levels over a 6-month period. Finally, worsening of androgen replacement therapy in elderly men should be sleep apnea and precipitation of superior sagittal sinus monitored closely. Men at this age are at risk for devel- thrombosis—seizures, facial palsy, hemiplegia, stupor, oping prostatic neoplasms (benign and malignant), and and coma—have been associated with androgen therapy. Potential sites of action include go- gens in the treatment of men with testicular deficien- nadotropin suppression, inhibition of androgen synthe- cies, these effects can be quite distressing to women. Compounds that degree of virilization in women will vary with the affect each of these sites are available. Potential clinical dosage, duration of therapy, and particular androgen uses of antiandrogens include suppression of androgen preparation used. It is ap- 200 mg/day, testosterone biosynthesis in both the adre- proved for the treatment of benign prostatic hyperpla- nal and testis is completely abolished by doses of 800 to sia. This drug is used most commonly for of the prostate gland following administration of finas- large virilizing adrenal tumors that cannot be surgically teride, clinical response may take 6 to 12 months. The prin- Androgen Receptor Antagonists cipal adverse effects of finasteride are impotence, de- creased libido, and decreased volume of ejaculate. These compounds are inhaled, in- should be checked within 1 month of starting the med- jected subcutaneously, or implanted subcutaneously. They are used in males in the treatment of precocious Flutamide (Eulexin) is a nonsteroidal androgen re- puberty and carcinoma of the prostate. Because of the toxicity of the oral Flutamide may eventually be used for the treatment of preparations and the inconvenience of the injectable hirsutism and male pattern baldness in women if a top- forms, the transdermal gels have been a major clinical ical preparation is developed. The serum level of testosterone in males from ado- (C) A decline in the metabolic clearance rate of lescence through the fifth decade of life is a prima- testosterone rily a consequence of (D) An increase in the metabolic clearance rate of (A) A relatively constant level of testicular testos- testosterone terone production (E) A sharp drop in urinary 17-ketosteroid levels (B) A significant decline in testosterone produc- 2. The enzyme 5 -reductase catalyzes the forma- (B) Elevated serum levels of dihydrotestosterone tion of dihydrotestosterone from testosterone. In (C) Highly depressed protein anabolic activity in normal accessory sex gland tissues, such as the skeletal muscle, bone, and kidney prostate, most of the direct androgen effect is due (D) Elevated serum levels of testosterone with sub- to dihydrotestosterone rather than testosterone. In the Leydig cell the rate-limiting step in testosterone is considered the biosynthetic rate- testosterone synthesis is the enzymatic cleavage of limiting step? Skeletal muscle cells use the androgen receptor (B) Cholesterol to bind testosterone that promotes the anabolic ef- (C) Androstenediol fect of this hormone. Finasteride is a 5 -reductase inhibitor, which es- (E) Progesterone sentially makes dihydrotestosterone unavailable to 4.
Buy generic myambutol online
Uricosuric agents also can influence the volume of distri- bution and hepatic metabolism of a number of drugs treatment for dogs galis discount myambutol 400 mg free shipping. Mechanism of Action Adverse reactions associated with probenecid ther- Allopurinol antibiotic zofran discount myambutol generic, in contrast to the uricosuric drugs infection signs and symptoms purchase myambutol 400 mg without a prescription, reduces apy include occasional rashes, allergic dermatitis, upper serum urate levels through a competitive inhibition of gastrointestinal tract irritation, and drowsiness. The uric acid synthesis rather than by impairing renal urate drug is contraindicated in patients with a history of re- reabsorption. After enzyme inhibition, the urinary and blood concentra- Sulfinpyrazone tions of uric acid are greatly reduced and there is a si- Sulfinpyrazone (Anturane), another uricosuric agent, is multaneous increase in the excretion of the more solu- chemically related to the antiinflammatory and urico- ble uric acid precursors, xanthine and hypoxanthine. This phenomenon contributes to the thera- drugs also metabolized by this system should be done peutic effectiveness of allopurinol in long-term use. Because allopurinol inhibits the oxidation Oxypurinol is probably responsible for the antigout ef- of mercaptopurine and azathioprine, their individual fects of allopurinol. Oxypurinol itself is not adminis- administered doses must be decreased by as much as tered because it is not well absorbed orally. Allopurinol may also increase the toxicity of other cy- Absorption, Metabolism, and Excretion totoxic drugs (e. The actions of allopuri- Allopurinol is largely absorbed after oral ingestion, nol are not antagonized by the coadministration of sal- reaching peak blood levels in about 1 hour. Clinical Uses Indomethacin (Indocin) (see Chapter 36) exerts an- Allopurinol is especially indicated in the treatment of tiinflammatory, antipyretic, and analgesic properties. Its nisms for its efficacy, allopurinol is particularly beneficial antiinflammatory activity and ability to inhibit leuko- for patients who already have developed renal uric acid cytic phagocytosis make it particularly valuable in treat- stones, patients with excessively high urate excretion ing the early stages of gout, because a decrease in the (e. This in- Phenylbutazone (Butazolidin,Tandearil) (see Chapter jury occurs when organs that either have been trans- 36) also displays antipyretic, analgesic, and antiinflam- planted or have had their usual blood perfusion blocked matory activity. In addition, it possesses some uricosuric are reperfused with blood or an appropriate buffer so- potency and therefore is widely used for the treatment lution. The cause of this injury is local formation of free of acute attacks of gouty arthritis, in which it is about radicals, such as the superoxide anion, the hydroxyl free equal to colchicine in effectiveness. These substances are strong does promote the renal excretion of uric acid, its use- oxidants and are quite damaging to tissues. Oxyphenbutazone (Oxalid, Tandearil) is the princi- Adverse Effects pal uricosuric metabolite of phenylbutazone. It has the Common toxicities associated with allopurinol adminis- same indications and toxicities as phenylbutazone. These reactions are of- Corticosteroids ten sufficiently severe to dictate termination of drug therapy. It is advised that therapy not be initiated dur- The use of corticosteroids is often suggested for elderly ing an acute attack of gouty arthritis. As with the urico- patients with chronic tophaceous gout, since gout in the suric drugs, therapy with allopurinol should be accom- older individual often displays symptoms similar to panied both by a sufficient increase in fluid intake to those of rheumatoid arthritis. The concomitant use of alcohol, non- acute attacks of gout that may be brought on during the steroidal antiinflammatory drugs, and most diuretics initial period of allopurinol ingestion. The most widely used agent for the treatment of have antiinflammatory activity and are useful in acute gouty arthritis is treating acute gouty arthritis but are not used (A) Probenecid nearly as widely as colchicine for initial treatment. Probenecid blocks active reabsorption of uric (C) Colchicine acid in the proximal tubules following glomerular (D) Indomethacin filtration. It does not inhibit uric acid synthesis (B), (E) Phenylbutazone stimulate tubular secretion (C), or inhibit the me- 2. Allopurinol inhibits xanthine oxidase, the en- (A) By inhibiting proximal tubular reabsorption of zyme involved in the conversion of hypoxanthine uric acid and xanthine to uric acid. It has no known ability to (B) By inhibiting production of uric acid in the increase uric acid synthesis markedly (A), inhibit re- liver absorption (C), or impair uric acid breakdown (D). While the other parts of the renal tubular sys- (D) By inhibiting breakdown of purines to uric tem do contain active transport systems, these sys- acid tems do not have an affinity of urate transport. The dietary intake of purines is not a major con- (A) Promoting the active secretion of uric acid in tributing factor to uric acid blood levels. Therefore, kidneys pharmacological reduction of uric acid synthesis or (B) Inhibiting uric acid synthesis increased excretion is required. Dietary restriction (C) Impairing renal urate reabsorption (A) can affect uric acid production if precursor mol- (D) Decreasing metabolism of uric acid ecules are lowered sufficiently, but this usually is not 4.
Discount myambutol 600 mg free shipping
The “te- Bone marrow depression can be counter- cans” topotecan and irinotecan are deriva- acted by granulocyte and granulocyte/mac- tivesofcam ptothecinfrom thefruitsofa rophage colony-stimulating factors (filgras- Chinesetree(Camptotheca acuminata) antibiotics diarrhea order myambutol with paypal. The density Targeting of Antineoplastic Drug of this receptor is greatly increased in some Action (A) types of breast cancer zombie infection nokia 5228 buy myambutol 600 mg mastercard. When the tumor cells When degenerating neoplastic cells display have bound antibody antibiotics and probiotics best buy for myambutol, immune cells can rec- special metabolic properties whichare differ- ognize them as elements to be eliminated. Itresultsfrom Cytostatics (B) translocation between chromosomes 9 and Initial success can be followed by loss of 22 of the c-abl protooncogene, leading to the effect because of the emergence of resistant hybrid bcr-abl fusion gene on chromosome tumor cells. Imatinib is a tyrosine kinase tein that may be needed for membrane inhibitor that specifically affects this mutant penetration (e. Cer- paclitaxel) is responsible for multidrug tain cells, in particular the tumor cells in resistance (mdr1 gene amplification). Supply of the ami- synthesis of dihydrofolate reductase may no acid can be disrupted by administration occur as a compensatory response to me- of the asparagine-hydrolyzing enzyme. Inhibition of apopto- may be of plant origin (Erwinia chrysanthe- sis due to activation of antiapoptotic cel- mi), when it is also named crisantaspase. Trastuzumab exemplifies a growing number of monoclonal antibodies that have become available for antineoplastic therapy. Mechanisms of cytostatic resistance Cytostatic drug Mutation and selection of resistant Uptake Decrease cells Increase Efflux pumping Bioactivation Decrease Site of action Change Effect Damage Repair Apoptosis Inhibition Luellmann, Color Atlas of Pharmacology © 2005 Thieme 304 Immune Modulators appears to be myelin basic protein. Glatir- Inhibition of Immune Responses amer resembles the latter; by blocking anti- Both the prevention of transplant rejection gen receptors, it interferes with antigen rec- and the treatment of autoimmune disorders ognition by lymphocytes. Glucocorticoids modulate the ex- gens and a long-term increase in the risk of pression of numerous genes; thus, the pro- neoplasms. In addition, gluco- rying specific receptors with the appropriate corticoids interfere with inflammatory cyto- antigen-binding site. B-lymphocytes “recog- kines and signaling molecules at variousoth- nize” antigen surface structures by means of er sites. Glucocorticoids are used in organ membrane receptors that resemble the anti- transplantations, autoimmune diseases, and bodies formed subsequently. Systemic use carries the (and naive B cells) require the antigen to be risk of iatrogenic Cushing syndrome (p. In contrast to glucocorticoids, ter permits recognition of antigenic struc- the plethora of accompanying metabolic ef- tures by means of the T-cell receptor. Theyareusedtosup- lation by cytokines plays an essential part in press transplant rejection reactions. It can be used in inhibits inosine monophosphate dehydro- the treatment ofmultiple sclerosisbesidesβ- genase, which catalyzes purine synthesis in interferon. The culprit antigen Luellmann, Color Atlas of Pharmacology © 2005 Thieme Inhibition of Immune Responses 305 A. Immune reaction and immunosuppressives Antigen Macrophage Virus-infected cell, Glucocorticoids transplanted cell. Risk factors for from animals immunized with human T- cardiovascular diseases may be adversely af- lymphocytes. The antibodies bind to and fected—a critical and important concern in damage T cells and can thus be used to at- long-term prognosis. At the molecular level, peptide composed of 11, in part atypical, however, its “receptor” is not cyclophilin but amino acids. Tacrolimus is ciclosporin is not degraded by gastrointesti- likewise used to prevent allograft rejection. In T-helper cells, it inhibits the Its epithelial penetrability is superior to that production of interleukin-2 by interfering at of ciclosporin, allowing topical application in the level of transcriptional regulation. The latter operates in the sig- The breakthroughs in modern transplanta- naling path leading from the interleukin-2 tion medicine are largely attributable to the receptor to activation of mitosis in lympho- introduction of ciclosporin. Its dosage must be titrated so that blood levels are neither too high (risk of renal injury) nor too low (re- jection reaction). Back-transport of the drug into the gut lumen occurs via the P-glycoprotein ef ux pump, in addition to metabolization by cy- tochrome oxidases of the 3A subfamily. Pro- tracted immunosuppression carries an in- Luellmann, Color Atlas of Pharmacology © 2005 Thieme Inhibition of Immune Responses 307 A. The substance possesses a very high Poisonings iron-binding capacitybutdoes notwithdraw Drugs used to counteract drug overdosage iron from hemoglobin or cytochromes.
Yorik, 57 years: Approximately tionships but rather is meant to draw attention to the 30% of patients with mild hypertension may be treated most prominent reflex changes. Irreversible antagonists bind to receptors with strong experimental fnding – some agonists, called partial agonists, cannot covalent bonds.
Tippler, 44 years: Selective β -blocking drugs have not been actively sought2 2 because there is no obvious clinical application for them; none is available for clinical use. Their cell bodies lie in the dor- Nociception sal root ganglia of the spinal cord or in the trigeminal gang- lia.
Murat, 39 years: Screening for disease complications in asymptomatic relatives at risk of a genetic disorder may also be appropriate, for example, 24-hour urine catecholamine estimation and abdominal scans Figure 2. It originates mainly from the upper two thirds of the lateral surface of the shaf of the tibia and The extensor digitorum longus muscle is the most pos adjacent surface of the interosseous membrane.
Gembak, 61 years: It can also be useful for the present in such small amounts that they are unlikely to short-term symptomatic control of persistent cough or have a significant effect except perhaps in renal failure. Poor absorption ing daptomycin should nevertheless be monitored for mus- from the intestine necessitates their administration i.
Giores, 50 years: Tidal volume falls, but minute ventilation The idea that a physical interaction is important stems is supported by a centrally mediated increase in respi- from experimental observations made in the late nine- ratory rate. Anti-infammatory drugs include corticoste- treat anxiety, although its possible side effects must roids and nonsteroidal anti-infammatory drugs be weighed against its benefts.
Gambal, 62 years: Vessels The walls of the intercondylar fossa bear two facets for and nerves passingbetween the thigh and leg pass through the superior attachment of the cruciate ligaments, which the popliteal fossa posterior to the knee joint. Dural venous sinuses The dural venous sinuses include the superior sagittal, inferior sagittal, straight, transverse, sigmoid, and occipital sinuses, the confluence of sinuses, and the cavernous, Dural partition Pia mater sphenoparietal, superior petrosal, inferior petrosal, and Subarachnoid space Arachnoid mater basilar sinuses {Fig.
Fabio, 21 years: This remains an area of active research because studies have reported inconsistent results as to the pathophysiologic importance of some polymorphisms. Structure and Mechanism of Action Clinical Uses Bacitracin is a mixture of polypeptide antibiotics pro- Bacitracin is highly active against staphylococci, Strep- duced by Bacillus subtilis.
Narkam, 54 years: The gastrointestinal tract 91 At an early stage rapid proliferation of the gut wall obliterates its lumen and this is followed by subsequent recanalization. When it is used as monotherapy, resistance and (Femstat) is an effective topical agent for vaginal can- clinical failure are common.
Shawn, 34 years: However, the molecular mechanisms of action of the three groups do not support this simplistic description. In addition to ethosuximide serum concentrations, important patient parameters (seizure fre- quency, potential ethosuximide side effects, etc.
Ali, 51 years: Containment of nodal spread depends on the exact cellular site of origin of the metastatic breast cancer is therefore potentially difcult cancer. Long-term suppression with oral acyclovir in patients with frequent recurrences of genital herpes decreases the frequency of symptomatic recurrences and of asymptomatic viral shedding, thus decreasing the rate of sexual transmission.
8 of 10 - Review by Y. Esiel
Votes: 121 votes
Total customer reviews: 121
References
- Mellen CK, Ford M, Rindone JP: Effect of high-dose cranberry juice on the pharmacodynamics of warfarin in patients, Br J Clin Pharmacol 70(1):139n 142, 2010.
- Gherman RB, Tramont J, Muffley P, et al: Analysis of McRoberts' maneuver by X-ray pelvimetry. Obstet Gynecol 95:43-47, 2000.
- Takizawa T, Kihara T, Kamata A, et al. Role of nitric oxide in regulating the ductus arteriosus caliber in fetal rats. J Vet Med Sci. 2000; 62:707-10.
- Chevalier RL, Goyal S, Wolstenholme JT, et al: Obstructive nephropathy in the neonatal rat is attenuated by epidermal growth factor, Kidney Int 54(1):38n47, 1998.
- De Simone R, Glombitza G, Vahl CF, et al: Three-dimensional color Doppler: A clinical study in patients with mitral regurgitation, J Am Coll Cardiol 33:1646-1654, 1999.
- Couderc M, Mathieu S, Glace B, Soubrier M. Efficacy of anakinra in articular chondrocalcinosis: Report of three cases. Joint Bone Spine 2012; 79(3):330-1.
- Oake N, Jennings A, Forster AJ, et al: Anticoagulation intensity and outcomes among patients prescribed oral anticoagulant therapy: a systematic review and meta-analysis. CMAJ 29:235, 2008.
- Alberts B, et al: The cytoskeleton. In Alberts B et al, editors: Molecular biology of the cell, ed 5, New York, 2008, Garland Science, pp 965-1062.