Dr Rafi k Bedair
- Department of Critical Care
- Manchester Royal Infi rmary
- Manchester
Glyset dosages: 50 mg
Glyset packs: 30 pills, 60 pills, 90 pills

Cheap glyset 50 mg buy online
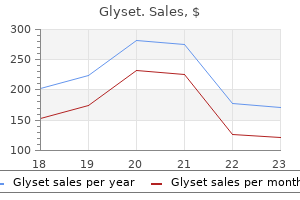
The latter two drowsiness 50 mg glyset for sale, sluggishness and coarse tremor order glyset without a prescription, leading on are metabolised to valproic acid which exerts the pharma- to giddiness safe glyset 50 mg, ataxia and dysarthria). Treatment syncope, oliguria, coma and even death may result if with valproic acid is easy to initiate (especially compared to treatment is not instigated urgently. Acute overdose may present without signs of of full blood count and liver function are recommended toxicity but with plasma concentrations well exceeding following reports of occasional blood dyscrasias or hepatic 2 mmol/L. Where not to be associated with the ‘rebound effect’ of relapse into toxicity is chronic, haemodialysis may be needed, espe- manic symptoms that may accompany early withdrawal of cially if renal function is impaired. Whole bowel irrigation may be an option for significant ingestion, but specialist Other drugs advice should be sought. Drugs that interfere with lithium excretion phylaxis of bipolar affective disorder, especially when de- by the renal tubules cause the plasma concentration to rise. Theophylline and sodium- control of acute manic symptoms, including both the gran- containing antacids reduce plasma lithium concentration. However, and phenytoin may cause neurotoxicity without affecting atypical antipsychotics such as olanzapine, quetiapine and the plasma lithium level. Carbamazepine Other drugs that have been used in augmentation of Carbamazepine is licensed as an alternative to lithium for existing agents include the anticonvulsants oxcarbazepine prophylaxis of bipolar affective disorder, although clinical and gabapentin, the benzodiazepine clonazepam, and trial evidence is actually stronger to support its use in the the calcium channel blocking agents verapamil and treatment of acute mania. The first panic attack often occurs with- out warning but may subsequently become associated with The disability andhealth costs caused by anxietyare highand specific situations, e. Antici- comparablewiththose of other commonmedicalconditions patory anxiety and avoidance behaviour develop in re- such as diabetes, arthritis or hypertension. The condition must be ety disorders experience impaired physical and role function- distinguished from alcohol withdrawal, caffeinism, hyper- ing, more workdayslost due toillness, increased impairment thyroidism and (rarely) phaeochromocytoma. Our understanding of Patients experiencing panic attacks often do not know the nature of anxiety has increased greatly from advances in what is happening to them, and because the symptoms research in psychology and neuroscience. It is now possible are similar to those of cardiovascular, respiratory or neuro- to distinguish different types of anxiety with distinct biolog- logical conditions, often present to non-psychiatric ser- ical and cognitive symptoms, and clear criteria have been ac- vices, e. The last specialists, where they may either be extensively investi- decade has seen developments in both drug and psycholog- gated or given reassurance that there is nothing wrong. A ical therapies such that a range of treatment options can be carefully taken history reduces the likelihood of this tailored to individual patients and their condition. Anxiety does not manifest itself only as a psychic or men- tal state: there are also somatic or physical concomitants, Treatment. Anxiety symp- course of these two classes of agent in panic disorder is toms exist on a continuum and many people with a mild depicted in Figure 20. On with- ciated disability of many anxiety disorders means that most drawal of the benzodiazepine, even when it is gradual, in- patients who fulfil diagnostic criteria for a disorder are creased symptoms of anxiety and panic attacks may occur, likely to benefit from some form of treatment. Both divide anxiety into a series of but patients need help to stay on treatment in the first subsyndromes with clear operational criteria to assist in weeks. At any one time many patients may the likely course of events and the antidepressant should have symptoms of more than one syndrome, but making be started at half the usual initial dose to reduce the likeli- the primary diagnosis is important as this can markedly in- hood of exacerbation. Treatment is poorly researched; there have been no prop- erly controlled trials and almost all open trials have been conducted on small numbers of patients long after the causative incident. The preferred treatment immediately 0 6 12 following the incident should probably be a short course of Weeks a hypnotic (or sedating antidepressant, e. Long-term ther- apy with antidepressants appears to be indicated at doses in the same range as for other anxiety disorders. The situations that provoke this fear can be quite specific, for example public speaking, or be of a much more generalised nature involving fear of Acute stress disorder/adjustment most social interactions, for example initiating or main- taining conversations, participating in small groups, dat- disorder ing, speaking to anyone in authority. Exposure to the Acute stress disorder is anxiety in response to a recent ex- feared situation almost invariably provokes anxiety with treme stress. Although in some respects it is a normal similar symptoms to those experienced by patients with and understandable reaction to an event, the problems as- panic attacks, but some seem to be particularly prominent sociated with it are not only the severe distress the anxiety and difficult, i. Some benzodiazepines 120 mg/day) causes less dependence and withdrawal, are reported to provide benefit but evidence for their ther- and is preferred to those that enter the brain rapidly, e.
50 mg glyset purchase with amex
Because of pharmacokinetic variability generic 50 mg glyset with visa, the narrow therapeutic index of quinidine 50 mg glyset overnight delivery, and the desire to avoid quinidine adverse side effects order 50 mg glyset fast delivery, measurement of quinidine serum concentrations can be a useful adjunct for patients to ensure that therapeutic, nontoxic levels are present. In addition to quinidine serum con- centrations, important patient parameters (electrocardiogram, clinical signs and symptoms of the arrhythmia, potential quinidine side effects, etc. When quinidine serum concentrations are measured in patients and a dosage change is necessary, clinicians should seek to use the simplest, most straightforward method avail- able to determine a dose that will provide safe and effective treatment. In most cases, a simple dosage ratio can be used to change quinidine doses assuming the drug follows linear pharmacokinetics. Sometimes, it is useful to compute quinidine pharmacokinetic constants for a patient and base dosage adjustments on these parameters. In this case, it may be possible to cal- culate and use pharmacokinetic parameters to alter the quinidine dose. In some situations, it may be necessary to compute quinidine pharmacokinetic param- eters as soon as possible for the patient before steady-state conditions occur and utilize these parameters to calculate the best drug dose. Computerized methods that incorporate expected population pharmacokinetic characteristics (Bayesian pharmacokinetic com- puter programs) can be used in difficult cases where serum concentrations are obtained at suboptimal times or the patient was not at steady state when serum concentrations were measured. An additional benefit of this method is that a complete pharmacokinetic workup (determination of clearance, volume of distribution, and half-life) can be done with one or more measured concentrations that do not have to be at steady state. Linear Pharmacokinetics Method Because quinidine follows linear, dose-proportional pharmacokinetics in most patients, steady-state serum concentrations change in proportion to dose according to the following equation: Dnew / Css,new = Dold / Css,old or Dnew = (Css,new / Css,old)Dold, where D is the dose, Css is the steady-state concentration, old indicates the dose that produced the steady-state concentration that the patient is currently receiving, and new denotes the dose necessary to produce the desired steady-state concentration. Because nonlinear pharmacokinetics for quinidine has been observed in some patients, suggested dosage increases greater than 75% using this method should be scrutinized by the prescribing clinician, and the risk versus benefit for the patient assessed before initiating large dosage increases (>75% over current dose). The patient would be expected to achieve steady-state conditions after the second day (5 t1/2 = 5 ⋅ 7 h = 35 h) of therapy. Using linear pharmacokinetics, the new dose to attain the desired concentration should be proportional to the old dose that produced the measured concentration. A steady-state quinidine serum concentration could be measured after steady state is attained in 3–5 half-lives. Since the patient is expected to have a half-life equal to 7 hours, the quinidine steady-state concentration could be obtained any time after the day of dos- ing (5 half-lives = 5 ⋅ 7 h = 35 h). Quinidine serum concentrations should also be meas- ured if the patient experiences a return of their arrhythmia, or if the patient develops potential signs or symptoms of quinidine toxicity. The patient would be expected to achieve steady-state conditions after 2 days (5 t1/2 = 5 ⋅ 9 h = 45 h) of therapy. Using linear pharmacokinetics, the new dose to attain the desired concentration should be proportional to the old dose that produced the measured concentration. If the patient was experiencing adverse drug effects, the new dosage regimen could be held for 1–2 estimated half-lives (t1/2 = 9 h). A steady-state quinidine serum concentration could be measured after steady state is attained in 3–5 half-lives. Since the patient is expected to have a half-life equal to 9 hours, the quinidine steady-state concentration could be obtained any time after the second day of dosing (5 half-lives = 5 ⋅ 9 h = 45 h). The patient would be expected to achieve steady-state conditions after 2 days (5 t1/2 = 5 ⋅ 7 h = 35 h) of therapy. Using linear pharmacokinetics, the new dose to attain the desired concentration should be proportional to the old dose that produced the measured concentration. A steady-state quinidine serum concentration could be measured after steady state is attained in 3–5 half-lives. Since the patient is expected to have a half-life equal to 7 hours, the quinidine steady-state concentration could be obtained any time after the second day of dosing (5 half-lives = 5 ⋅ 7 h = 35 h). Quinidine serum concentrations should also be measured if the patient experiences a return of their arrhythmia, or if the patient develops potential signs or symptoms of quinidine toxicity. Pharmacokinetic Parameter Method The pharmacokinetic parameter method of adjusting drug doses was among the first techniques available to change doses using serum concentrations. It allows the computa- tion of an individual’s own, unique pharmacokinetic constants and uses those to calculate a dose that achieves desired quinidine concentrations. The pharmacokinetic parameter method requires that steady state has been achieved and uses only a steady-state quini- dine concentration (Css).
Discount 50 mg glyset
Because cetuximab is of the G isotype purchase glyset amex, its antitumor activity may also1 be mediated 50 mg glyset buy free shipping, in part discount 50 mg glyset mastercard, by immunologic-mediated mechanisms. There is growing evidence that cetuximab can be effectively and safely combined with irinotecan- and oxaliplatin-based chemotherapy in the first-line treatment of metastatic colorectal cancer as well. Regimens combining cetuximab with cytotoxic chemotherapy may be of particular benefit in the neoadjuvant therapy of patients with liver-limited disease. Although this antibody was initially approved to be administered on a weekly schedule, pharmacokinetic studies have shown that an every-2-week schedule provides the same level of clinical activity as the weekly schedule. This agent is also approved for use in combination with radiation therapy in patients with locally advanced head and neck cancer. Cetuximab is well tolerated, with the main adverse effects being an acneiform skin rash, hypersensitivity infusion reaction, and hypomagnesemia. In contrast to cetuximab, this antibody is of the G isotype, and as such, it would not be expected2 to exert any immunologic-mediated effects. Recent clinical studies have shown that this antibody can be effectively and safely combined with oxaliplatin- and irinotecan-based chemotherapy in the first- and second-line treatment of metastatic colorectal cancer. Patients who are nonsmokers and who have a bronchoalveolar histologic subtype appear to be more responsive to these agents. In addition, erlotinib has been approved for use in combination with gemcitabine for the treatment of advanced pancreatic cancer. An acneiform skin rash, diarrhea, and anorexia and fatigue are the most common adverse effects observed with these small molecules (Table 54–5). One potential advantage of this antibody is that it does not appear to exacerbate the toxicities typically observed with cytotoxic chemotherapy. The main safety concerns associated with bevacizumab include hypertension, an increased incidence of arterial thromboembolic events (transient ischemic attack, stroke, angina, and myocardial infarction), wound healing complications, gastrointestinal perforations, and proteinuria. It was initially approved for advanced renal cell cancer and is also approved for advanced hepatocellular cancer. Hypertension, bleeding complications, and fatigue are the most common adverse effects seen with these drugs. With respect to sorafenib, skin rash and the hand-foot syndrome are observed in up to 30–50% of patients. For sunitinib, there is also an increased risk of cardiac dysfunction, which in some cases can lead to congestive heart failure. In contrast, normal cells can synthesize L-asparagine and thus are less susceptible to the cytotoxic action of asparaginase. The main adverse effect of this agent is a hypersensitivity reaction manifested by fever, chills, nausea and vomiting, skin rash, and urticaria. The strategy for developing drug regimens also requires knowledge of the specific characteristics of individual tumors. Does the drug require activation in certain normal tissue such as the liver (cyclophosphamide), or is it activated in the tumor tissue itself (capecitabine)? In patients with breast cancer, analysis of the tumor for expression of estrogen or progesterone receptors is important in guiding therapy with selective estrogen receptor modulators. In the case of prostate cancer, chemical suppression of androgen secretion with gonadotropin-releasing hormone agonists or antagonists is important. The use of specific cytotoxic and biologic agents for each of the main cancers is discussed in this section. A subset of patients with neoplastic lymphocytes expressing surface antigenic features of T lymphocytes has a poor prognosis (see Chapter 55). Subsequently, corticosteroids, 6-mercaptopurine, cyclophosphamide, vincristine, daunorubicin, and asparaginase have all been found to be active against this disease. The value of prophylactic intrathecal methotrexate therapy for prevention of central nervous system leukemia (a major mechanism of relapse) has been clearly demonstrated. While there are several anthracyclines that can be effectively combined with cytarabine, idarubicin is preferred. Such care includes platelet transfusions to prevent bleeding, the granulocyte colony-stimulating factor filgrastim to shorten periods of neutropenia, and antibiotics to combat infections.
Discount generic glyset canada
In this patient’s case buy 50 mg glyset, it is unlikely that the patient is at steady state so the linear pharmacokinetics method cannot be used discount glyset 50 mg buy line. A 500-mg dose of quinidine gluconate is equivalent to 300 mg of quinidine base while a 648-mg dose of quinidine gluconate is equal to 400 mg of quinidine base (300-mg quinidine base = 500-mg quinidine gluconate ⋅ 0 discount glyset american express. The pharmacokinetic parameters computed by the program are a volume of distribu- tion of 130 L, a half-life equal to 23. The oral one-compartment model equation used by the program to compute doses indicates that 324 mg of quinidine gluconate extended-release tablets every 12 hours will produce a steady-state trough concentration of 4. Enter patient’s demographic, drug dosing, and serum concentration/time data into the computer program. In this patient case, it is unlikely that the patient is at steady state so the linear pharma- cokinetics method cannot be used. A 600-mg dose of quinidine sulfate is equivalent to 500 mg of quinidine base (500-mg quinidine base = 600-mg quinidine sulfate ⋅ 0. The pharmacokinetic parameters computed by the program are a volume of distribu- tion of 238 L, a half-life equal to 51. The oral one-compartment model equation used by the program to compute doses indicates that 200 mg of quinidine sulfate immediate-release tablets every 12 hours will produce a steady-state trough concentration of 3. Short- and long-acting oral quinidine preparations: clinical implications of pharmacokinetic differences. Steady-state serum levels of quinidine and active metabolites in cardiac patients with varying degrees of renal function. Prevalence of high (3S)-3-hydroxyquinidine/quini- dine ratios in serum, and clearance of quinidine in cardiac patients with age. The effect of quinidine and its metabolites on the elec- trocardiogram and systolic time intervals: concentration-effect relationships. Pharmacokinetics of dihydroquinidine in congestive heart failure patients after intravenous quinidine administration. Dihydroquinidine contamination of quinidine raw materials and dosage forms: rapid estimation by high-performance liquid chromatography. Quinidine pharmacokinetics in man: choice of a dispo- sition model and absolute bioavailability studies. Inhibition of desipramine hydroxyla- tion in vitro by serotonin-reuptake- inhibitor antidepressants, and by quinidine and ketocona- zole: a model system to predict drug interactions in vivo. Inhibition of desipramine hydroxylation (Cytochrome P450-2D6) in vitro by quinidine and by viral protease inhibitors: relation to drug interactions in vivo. It is an effective anticonvulsant for the chronic treatment of tonic-clonic (grand mal) or partial seizures and the acute treatment of generalized status epilepticus (Table 10-1). Orally administered phenytoin is used chronically to provide prophylaxis against tonic-clonic or partial seizures. The antiseizure activity of phenytoin is related to its ability to inhibit the repetitive fir- ing of action potentials caused by prolonged depolarization of neurons. At the cellular level, the mecha- nism of action for phenytoin appears related to its ability to prolong the inactivation of voltage-activated sodium ion channels and reduction of the ability of neurons to fire at high frequencies. Since phenytoin is highly bound (~90%) to albumin, it is prone to plasma protein binding displacement due to a large variety of factors. Although there is clinical data to support the therapeutic range for total phenytoin concentrations, the suggested therapeutic range for unbound phenytoin 485 Copyright © 2008 by The McGraw-Hill Companies, Inc. Simple partial seizures Drugs of choice locally) (without impaired Carbamazepine consciousness) Phenytoin a. Absence seizures (typical or Drugs of choice or nonconvulsive) atypical; also known as petit Ethosuximide mal seizures) Valproic acid Alternatives Lamotrigine Clonazepam Zonisamide Levetiracetam 2. Thus, the generally accepted therapeutic range for unbound phenytoin concentrations is 1–2 μg/mL, which is simply 10% of the lower and upper bounds for the total concentration range, respectively. In the upper end of the therapeutic range (>15 μg/mL) some patients will experience minor central nervous system depression side effects such as drowsiness or fatigue. When total concentrations exceed 30 μg/mL, ataxia, slurred speech, and/or incoordination similar to ethanol intoxication can be observed. If total pheny- toin concentrations are above 40 μg/mL, mental status changes, including decreased menta- tion, severe confusion or lethargy, and coma are possible. Because phenytoin follows nonlinear or saturable metabolism pharmacokinetics, it is possible to attain excessive drug concentrations much easier than for other compounds that follow linear pharmacokinetics.
50 mg glyset fast delivery
Inward extensions of this fascial layer form fat that separate buy 50 mg glyset overnight delivery, support glyset 50 mg on line, and interconnect organs and intermuscular septa that compartmentalize groups of structures glyset 50 mg lowest price, enable movement of one structure relative to muscles with similar functions and innervations. Other another, and allow the transit of vessels and nerves from extensions surround individual muscles and groups of one area to another. Finally, there is a layer of deep fascia separating The muscular system is generally regarded as consisting of the membrane lining the abdominal cavity (the parietal one type of muscle found in the body-skeletal muscle. A similar layer of fascia in the thorax is termed of muscle can be characterized by whether they are con the endothoracic fascia. In the clinic • Skeletal muscle forms the majority of the muscle tissue The importance of fascias in the body. It consists of parallel bundles of long, mul A fascia is a thin band of tissue that surrounds muscles, tinucleated fbers with transverse stripes, is capable of bones, organs, nerves, and blood vessels and ofen powerful contractions, and is innervated by somatic and remains uninterrupted as a three-dimensional structure branchial motor nerves. It provides important support for bones and other structures, and provides support and tissues and can provide a boundary between structures. Individual skeletal muscles are Fascias have specifc dynamic properties and may be ofen named on the basis of shape (e. Clinically, fascias are extremely important because palmar interosseous muscle), or fber orientation (e. When infections or malignant diseases cross a • Cardiac muscle isstriated muscle found only inthe walls fascial plain, a primary surgical clearance may require a of the heart (myocardium) and in some of the large far more extensive dissection to render the area free of vessels close to where they join the heart. Infection within an tions are less powerful than those of skeletal muscle and intervertebral body secondary to tuberculosis can pass it is resistant to fatigue. It is found in the walls of blood vessels (tunica media), associated with hair follicles in the skin, located in the eyeball, and found in the walls of various structures associated with the gastrointesti nal, respiratory, genitourinary, and urogenital systems. It can muscle or muscle group and may be associated with be produced by a variety of causes, which include nerve other neurological abnormalities, including loss of damage to the muscle and disuse. Paralysis may be due to abnormalities in the Muscle atrophy is an important problem in patients brain, the spinal cord, and the nerves supplying the who have undergone long-term rest or disuse, requiring muscles. Major causes include stroke, trauma, extensive rehabilitation and muscle building exercises poliomyelitis, and iatrogenic factors. In the long term, muscle paralysis will produce secondary muscle wasting and overall atrophy of the region due to disuse. In the clinic Muscle injuries and strains identif which muscle groups are afected and the extent Muscle injuries and strains tend to occur in specifc muscle of the tear to facilitate treatment and obtain a prognosis, groups and usually are related to a sudden exertion and which will determine the length of rehabilitation muscle disruption. The cardiovascular system consists of the heart, which • Small and medium veins contain small amounts of pumps blood throughout the body, and the blood vessels, smooth muscle, and the thickest layer is the tunica which are a closed network of tubes that transport the externa. There are three types of blood vessels: superfcial veins in the upper and lower limbs and deeper veins of the leg and forearm. The walls of the blood vessels of the cardiovascular • The walls of veins, specifcally the tunica media, are system usually consist of three layers or tunics: thin. These are and large arteries), and usually paired cusps that facilitate blood flow toward • tunica intima-the inner endothelial lining of the blood the heart. More specifc information about the cardiovascular Arteries are usually further subdivided into three system and how it relates to the circulation of blood classes, according to the variable amounts of smooth throughout the body will be discussed, where appropriate, muscle and elastic fbers contributing to the thickness of in each of the succeeding chapters of the text. Atherosclerosis Examples of large elastic arteries are the aorta, the bra Atherosclerosis is a disease that affects arteries. There is chiocephalic trunk, the left common carotid artery, the a chronic infammatory reaction in the walls of the left subclavian artery, and the pulmonary trunk. This calcifcation, with reduction in the diameter of the characteristic allows these vessels to regulate their vessels impeding distal fow. The plaque itselfmay be a diameter and control the flow of blood to different parts site for attraction of platelets that may "fall of" of the body. Plaque fssuring may occur, which most of the named arteries, including the femoral, axil allows fresh clots to form and occlude the vessel. If atherosclerosis • Small arteries and arterioles control the flling of the occurs in the carotid artery, small emboli may form and capillaries and directly contribute to the arterial pres produce a stroke.
Glyset 50 mg buy
Phenytoin serum concentrations should also be measured if the patient experiences an exacerbation of their epilepsy buy glyset, or if the patient develops potential signs or symptoms of phenytoin toxicity glyset 50 mg order visa. The patient was prescribed 300 mg/d of extended phenytoin sodium capsules for 1 month cheap glyset 50 mg with mastercard, and the steady-state phenytoin total concentration equals 10. Suggest an initial phenytoin dosage regimen designed to achieve a steady-state phenytoin concentration within the middle of the thera- peutic range. Use pseudolinear pharmacokinetics to predict new concentration for a dosage increase, then compute 15–33% factor to account for Michaelis-Menten pharmacokinetics. Since the patient is receiving extended phenytoin sodium capsules, a convenient dosage change would be 100 mg/d and an increase to 400 mg/d is suggested. Using pseudolinear pharmacokinetics, the resulting total steady-state phenytoin serum concen- tration would equal: Cssnew = (Dnew / Dold)Cssold = (400 mg/d / 300 mg/d)10. Because of Michaelis-Menten pharmacokinetics, the serum concentration would be expected to increase 15%, or 1. Thus, a dosage increase of 100 mg/d would be expected to yield a total phenytoin steady-state serum concentration between 16–19 μg/mL. A steady-state trough total phenytoin serum concentration should be measured after steady state is attained in 7–14 days. Phenytoin serum concentrations should also be measured if the patient experiences an exacerbation of their epilepsy, or if the patient develops potential signs or symptoms of phenytoin toxicity. Suggest an initial phenytoin dosage regimen designed to achieve a steady-state phenytoin concentration within the therapeutic range. A new total phenytoin steady-state serum concentration equal to 10 μg/mL is chosen for the patient: D = (D / Css ) ⋅ Css 0. A steady-state trough total phenytoin serum concentration should be measured after steady state is attained in 7–14 days. Phenytoin serum concentrations should also be measured if the patient experiences an exacerbation of their epilepsy, or if the patient develops potential signs or symptoms of phenytoin toxicity. The patient was prescribed 300 mg/d of extended phenytoin sodium capsules for 1 month, and the steady-state phenytoin total concentration equals 10. Suggest an initial phenytoin dosage regimen designed to achieve a steady-state phenytoin concentration of 18 μg/mL. A new total phenytoin steady-state serum concentration equal to 18 μg/mL is chosen for the patient: D = (D / Css ) ⋅ Css 0. A steady-state trough total phenytoin serum concentration should be measured after steady state is attained in 7–14 days. Phenytoin serum concentrations should also be measured if the patient experiences an exacerbation of their epilepsy, or if the patient develops potential signs or symptoms of phenytoin toxicity. The use of the population’s parameter orbs allows the plot to be used with one phenytoin steady-state concentration/dose pair. The orbs represent 50%, 75%, 85%, and so on, of the population param- eter combinations for Vmax and Km. The concurrent steady-state phenytoin serum con- centration is plotted on the left portion of the x-axis (circle, 6. If the line intersects more than one orb, the innermost orb is selected, and the midpoint of the line contained within that orb is found and marked (x mark within orbs). The new desired steady-state concentration is identified on the left portion of the x-axis (x mark on x-axis, 10 μg/mL), and the two x marks are connected by a straight line. A straight line is drawn between these two points, extended into the right sector, and through the orbs contained in the right sector. If the line intersects more than one orb, the innermost orb is selected, and the midpoint of the line contained within that orb is found and marked with a point. The midpoint within the orb and the desired steady-state phenytoin total con- centration (on the left portion of the x-axis) are connected by a straight line. The intersec- tion of this line with the y-axis is the new phenytoin dose required to achieve the new phenytoin concentration. If a line parallel to the y-axis is drawn down to the x-axis from the midpoint of the line contained within the orb, an estimate of Km (in μg/mL) is obtained. Similarly, if a line parallel to the x-axis is drawn to the left to the y-axis from the midpoint of the line contained within the orb, an estimate of Vmax (in mg/kg/d) is obtained. The patient was prescribed 400 mg/d of extended phenytoin sodium capsules for 1 month, and the steady-state phenytoin total concentration equals 6.
Order glyset 50 mg with mastercard
High chlor- Nonionic Bisphenols hexidine concentrations cause intracellular protein pre- Triclosan is a broad-spectrum antimicrobial compound glyset 50 mg order without a prescription. Despite its pronounced effect It was originally used in soaps purchase glyset online now, antiperspirants order glyset 50 mg visa, and cos- on plaque formation, no detectable changes in resist- metic toiletries as a germicide. Today, triclosan is incor- ance of plaque bacteria were found in a 6-month longi- porated into toothpaste because of its wide spectrum of tudinal study of mouth rinses. Clinical Uses Pharmacokinetics The previous routine treatment for cases of severe gin- Triclosan is retained in dental plaque for at least 8 gival disease consisted of calculus and plaque removal hours, which in addition to its broad antibacterial prop- and oral hygiene instructions. Subsequent resolution of erty could make it suitable for use as an antiplaque the gingival inflammation was largely dependent on agent in oral care preparations. The most conspicuous side effect of chlorhexidine is the development of a yellow to brownish extrinsic stain on Mechanism of Action the teeth and soft tissues of some patients. The discol- oration on tooth surfaces is extremely tenacious, and a Triclosan is active against a broad range of oral gram- professional tooth cleaning using abrasives is necessary positive and gram-negative bacteria. The staining is dose dependent, of its antibacterial activity is the bacterial cell mem- and variation in severity is pronounced between indi- brane. In contrast to the efficacy of fluorides in preventing car- Clinical Effects ious lesions, these formulations have relatively poor an- tibacterial properties (Table 42. Finally, of considerable interest terfere with bacterial membrane function, bacterial is the observation that triclosan inhibits gingivitis by a adhesion, and glucose uptake, thereby inhibiting the mechanism independent of its antiplaque activity. Prebrushing Rinses Essential Oils The topical application of a liquid rinse before brushing A mixture of essential oils consisting of thymol 0. Prebrushing rinses usually Essential oils may reduce plaque levels by inhibiting contain a plethora of ingredients, and it is not known bacterial enzymes and by reducing pathogenicity of which constituent is the active chemical. It has been sug- plaque via reduction of the amount of endotoxin; the al- gested that sodium lauryl sulfate acts as a detergent to cohol is probably responsible for denaturing bacterial dislodge or loosen the plaque on teeth (Table 42. The substantivity of Listerine appears to be When prebrushing rinses were tested against placebo quite low, and therefore, it must be used at least twice a rinses, prebrushing rinses appeared to have no effect on day to be effective. Adverse reac- Today gingivitis and periodontitis are prevented princi- tions include a bitter taste and burning sensation in the pally through mechanical plaque control; however, den- oral cavity. Regular use of high-alcohol rinses can ag- tition free of supragingival and subgingival plaque is ex- gravate existing oral lesions and desiccate mucous tremely difficult to accomplish and maintain. The goal of future product development is not so Fluorides much an improvement in the antiplaque performance Fluorides are widely used in caries prevention, for which of the existing effective compounds but rather lessening they have been highly effective. Systemic administration of their side effects and development of better delivery of fluorides for caries prevention is available via drink- systems. Products that combine various known com- 42 Drugs for the Control of Supragingival Plaque 505 pounds with well-established plaque-inhibiting proper- vention of supragingival plaque will depend on prod- ties are under investigation. The other four compounds are substrate in the oral cavity is not cationic and do not bind strongly to tissues. Triclosan (A) is active against a broad range of (B) Absorption oral gram-positive and gram-negative bacteria. Yellow or brownish extrinsic stain of teeth is a fre- bacteria, but Streptococcus mutans and Actinomyces quently observed side effect of viscosus, two bacteria particularly associated with (A) Fluoride dental lesions, are especially susceptible to its ac- (B) Triclosan tion. Stannous fluoride (D) is widely used in caries (C) Essential oils prevention, and many studies have proven its effec- (D) Chlorhexidine tiveness. Proceedings of the 2nd involved in drug elimination, while absorption (B) European Workshop on Periodontology. Rinsing, irrigation and sustained local scribes the ability of a drug to enter a variety of body delivery. In most instances, dental plaque can cause ery- Administration was evaluating the results of a new thema and gingival bleeding, but the gingival re- drug for the treatment of periodontal disease. For exam- revealed swollen and tender gingiva that were ple, the age of the patient, her appearance, and accompanied by erythema and bleeding upon mild questions about her diet should be enough to provocation. Her dental radiographs revealed no rule in or out issues concerning puberty and mal- abnormalities, and her physician found her to be nutrition. She reports be ruled out, an additional physical examination taking no medications and denies allergies to any by a physician may be necessary. She is concerned about her health to be requested could include oral glucose toler- because her gingiva will bleed when she eats fibrous ance test for diabetes mellitus, human chorionic foods (e. What do you think is the most likely cause of her tative and quantitative evaluation of bone mar- periodontal disease? If the patient’s periodontal disease is the result physical examination for a systemic alteration of a leukemia or diabetes mellitus, the first re- that was overlooked at her last physical examina- sponse should be to treat the disease that is exac- tion?
Glyset 50 mg visa
For patients with paroxysmal atrial fibrillation glyset 50 mg purchase with mastercard, normal sinus rhythm may be restored with a single large oral dose of propafenone or flecainide cheap glyset 50 mg buy line, provided that safety is initially documented in a monitored setting buy 50 mg glyset fast delivery. In some cases, the risk of an adverse reaction is clearly related to high dosages or plasma concentrations. In other cases, adverse reactions are unrelated to high plasma concentrations (eg, procainamide-induced agranulocytosis). For many serious adverse reactions to antiarrhythmic drugs, the combination of drug therapy and the underlying heart disease appears important. Several specific syndromes of arrhythmia provocation by antiarrhythmic drugs have also been identified, each with its underlying pathophysiologic mechanism and risk factors. Treatment for torsades requires recognition of the arrhythmia, withdrawal of any offending agent, correction of hypokalemia, and treatment with maneuvers to increase heart rate (pacing or isoproterenol); intravenous magnesium also appears effective, even in patients with normal magnesium levels. Drugs that markedly slow conduction, such as flecainide, or high concentrations of quinidine, can result in an increased frequency of reentry arrhythmias, notably ventricular tachycardia in patients with prior myocardial infarction in whom a potential reentry circuit may be present. Treatment here consists of recognition, withdrawal of the offending agent, and intravenous sodium to reverse unidirectional block. Conduct of Antiarrhythmic Therapy The urgency of the clinical situation determines the route and rate of drug initiation. Drug therapy can be considered effective when the target arrhythmia is suppressed (according to the measure used to quantify it at baseline) and toxicities are absent. Conversely, drug therapy should not be considered ineffective unless toxicities occur at a time when arrhythmias are not suppressed. Plasma drug concentrations are also important in establishing compliance during long-term therapy as well as in detecting drug interactions that may result in very high concentrations at low drug dosages or very low concentrations at high dosages. Duan D: Phenomics of cardiac chloride channels: The systemic study of chloride channel function in the heart. Wolbrette D et al: Dronedarone for the treatment of atrial fibrillation and atrial flutter: Approval and efficacy. Selection of a drug that is tolerated in heart failure and has documented ability to convert or prevent atrial fibrillation, eg, dofetilide or amiodarone, would be appropriate. Despite five different antihypertensives, his clinic blood pressure is 176/92 mm Hg and he has 2–3+ edema on exam. At the clinic visit, hydrochlorothiazide 25 mg daily is added for better blood pressure control and symptoms/signs of fluid overload. Two weeks later, the patient presents to the emergency department with symptoms of weakness, anorexia, and generalized malaise. Abnormalities in fluid volume and electrolyte composition are common and important clinical disorders. Drugs that block specific transport functions of the renal tubules are valuable clinical tools in the treatment of these disorders. Although various agents that increase urine volume (diuretics) have been described since antiquity, it was not until 1937 that carbonic anhydrase inhibitors were first described and not until 1957 that a much more useful and powerful diuretic agent (chlorothiazide) became available. Technically, a “diuretic” is an agent that increases urine volume, whereas a “natriuretic” causes an increase in renal sodium excretion and an “aquaretic” increases excretion of solute-free water. Osmotic diuretics and antidiuretic hormone antagonists (see Agents that Alter Water Excretion) are aquaretics that are not directly natriuretic. Several autacoids, which exert multiple, complex effects on renal physiology (adenosine, prostaglandins, and urodilatin, a renal autacoid closely related to atrial natriuretic peptide), are also discussed. Many diuretics exert their effects on specific membrane transport proteins in renal tubular epithelial cells. Other diuretics exert osmotic effects that prevent water reabsorption (mannitol), inhibit enzymes (acetazolamide), or interfere with hormone receptors in renal epithelial cells (vaptans, or vasopressin antagonists). The physiology of each nephron segment is closely linked to the basic pharmacology of the drugs acting there, which is discussed in the second section. As tubule fluid is processed along the length of the proximal tubule, the luminal concentrations of most solutes decrease relative to the concentration of inulin, an experimental marker that is filtered but neither secreted nor absorbed by renal tubules. This + + transport system allows Na to enter the cell from the tubular lumen in exchange for a proton (H ) from inside the cell. Because of rapid equilibration, concentrations of the solutes are approximately equal in the interstitial fluid and the blood. Although not indicated as diuretic agents, these drugs have diuretic properties accompanied by increased sodium and glucose excretion (see below). Free H causes luminal pH to fall, activating a poorly − + + − defined Cl /base exchanger (Figure 15–2).
Chenor, 21 years: Enter patient’s demographic, drug dosing, and serum concentration/time data into the computer program.
Nafalem, 39 years: Growth Hormone Deficiency Growth hormone deficiency can have a genetic basis, be associated with midline developmental defect syndromes (eg, septo-optic dysplasia), or be acquired as a result of damage to the pituitary or hypothalamus by a traumatic event (including breech or traumatic delivery), intracranial tumors, infection, infiltrative or hemorrhagic processes, or irradiation.
Sebastian, 41 years: Oral Dosage The oral dosage for rapidly excreted tetracyclines, equivalent to tetracycline hydrochloride, is 0.
Ur-Gosh, 38 years: It quate ventilatory support is available, it might be appears that the ingestion occurred in the past 2 better to treat the patient symptomatically.
Fraser, 65 years: After dosage titration, the patient was prescribed 500 mg every 12 hours of ethosuximide capsules (1000 mg/d) for 1 month, and the steady-state ethosuximide total concentration equals 38 μg/mL.
Marcus, 43 years: Hypnosis presumably2 2 results from stimulation of α receptors in the locus caeruleus, and the analgesic effect originates at the level of the spinal2 cord.
Tarok, 54 years: Examples oneandthesam edrugm akethepharm a- of such fundamental innovations from re- ceutical markets of some countries (e.
Grobock, 31 years: Tacrolimus concentrations would be obtained on a daily basis with steady state expected to occur after about 3 days of therapy (5 half-lives = 5 ⋅ 12 h = 60 h).
Alima, 30 years: On each side, the vestibular ligament of the quadrangu lar membrane is separated from the vocal ligament of the cricothyroid ligament below by a gap.
Treslott, 52 years: They are very powerful (hence the The kidney is one of the major routes of drug elimination, and term ‘high ceiling’) and can cause serious electrolyte imbalances and impairment of renal function in old age or in renal disease can signif- dehydration.
Sulfock, 27 years: Each originates from the undersurface of important landmark in the floor of the oral cavity: the palatine aponeurosis and passes anteroinferiorly to the lateral side of the tongue (Fig.
Wenzel, 34 years: The sternal end has a much largerfacetfor articulation mainly with the manubrium of the sternum, and to a lesser extent, with the frst costal cartilage.
8 of 10 - Review by Z. Lisk
Votes: 94 votes
Total customer reviews: 94
References
- J. Haleblian andW. McCrone, J. Pharm. Sci. 58, 911, 1969; J. Haleblian, J. Pharm. Sci. 64, 1269, 1975.
- Kinkead TM, Menon M: Renal tubular acidosis [lesson 7], AUA Update Series 14:54n59, 1995.
- Sakowitz OW, Stover JF, Sarafzadeh AS, Unterberg AW, Kiening KL. Effects of mannitol bolus administration on intracranial pressure, cerebral extracellular metabolites, and tissue oxygenation in severely head-injured patients. J Trauma 2007;62(2):292-298.
- Vodusek DB, Light JK, Libby JM: Detrusor inhibition induced by stimulation of pudendal nerve afferents, Neurourol Urodyn 5(4):381n389, 1986.
- Winquist E, Kirchner TS, Segal R, et al: Neoadjuvant chemotherapy for transitional cell carcinoma of the bladder: a systematic review and metaanalysis, J Urol 171(2 Pt 1):561n569, 2004.