Mickey Karram, MD
- Director of Urogynecology, The Christ Hospital
- Clinical Professor of Obstetrics
- and Gynecology, University of Cincinnati, Cincinnati, Ohio
Evista dosages: 60 mg
Evista packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Purchase generic evista on line
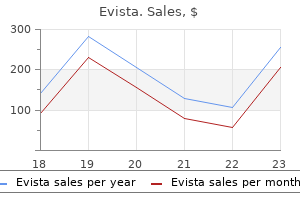
Spain consistently sible that alternative cocaine trafficking methods and reports the highest cocaine seizures in Europe menstruation longer than 7 days cheap evista 60 mg on-line, though routes adopted by traffickers to counter more effective seizures fell from 50 mt in 2006 to 25 mt in 2009 menopause dry skin order discount evista on-line. In law enforcement efforts have corrected a short-term neighbouring Portugal menstruation postpartum evista 60 mg order fast delivery, the decrease has been more pro- drop of cocaine availability in the European market. In relative terms, seizure trends across Europe in recent Africa years appear to fall broadly along a continuum ranging Cocaine seizures remained limited in Africa, amounting from strong declines close to the trafficking hubs that to less than 1 mt in 2009, down from 2. Although this quantity is very small Europe to strong increases in countries, notably further in comparison with the quantities likely to be trafficked east, that historically have not been associated with traf- in and via Africa, seizure data from other regions also ficking of cocaine in large amounts. When comparing point to a decreasing trend for Africa, notably West average seizures over 2005-2006 with 2008-2009, Africa, for cocaine trafficking from South America to marked declines (in both relative and absolute terms) Europe. Nevertheless, cocaine trafficking in West Africa were registered in Portugal, Spain, Belgium and the 26 persisted, and Africa, especially West Africa, remained Netherlands; more moderate declines were registered vulnerable to a resurgence. Benin, Burkina Faso, Ethio- in the United Kingdom and France, while seizures were pia, the Gambia, Ghana, Guinea, Guinea-Bissau, Kenya, essentially stable in Italy and Germany. In 2009, China 300 reported seizures of 163 kg, including 112 kg in Hong 200 Kong, China. According to Chinese authorities, cocaine 100 was mainly smuggled from South America across the Pacific ocean to cities on China’s south-east coast. The increase was partly due to a large quantity of cocaine that was jettisoned in December The Asia-Pacific region continued to account for less 2009 close to the Eastern Samar province from a vessel than 1% of global cocaine seizures. Two other signs that cocaine trafficking might be making inroads significant cases resulted in the seizure of a total of 15. The size of the United of the decline may be explained by improved upstream States’ market – the single largest cocaine market for interception efforts as a result of improved sharing of decades – has been shrinking in recent years, mainly due intelligence with counterparts in South America. Cocaine trafficking and use have started to limited (a few studies conducted in North America, affect countries in the Oceania region (already showing South America, Europe and Australia) and any calcu- high annual cocaine use prevalence rates by interna- lated results must be treated with caution (and results tional standards), countries in western and southern are subject to change, whenever more reliable informa- Africa affected by the transit flow, and in some parts of tion becomes available). The best reading of existing Asia (some countries in the Near and Middle East as data and estimates suggests that some 440 mt of pure well as some emerging pockets in a few countries in the cocaine were consumed in 2009. Cocaine use in East Europe, in con- Of the 440 mt available for consumption, around 63% trast, is still limited. The volume of cocaine consumed were consumed in the Americas, 29% in Europe, 5% in in Europe has doubled over the last decade, even though Africa, 3% in Asia and less than 1% in Oceania. The data for the last few years show signs of stabilization at largest subregional markets were found in North Amer- the higher levels. These three subregions account for increased their efforts, traffickers continue to innovate, 63% of global cocaine consumption. The single largest seeking novel ways of getting their product to the con- cocaine market – despite strong declines in recent years sumer. Around 2004, South American traffickers began - continues to be the United States of America, with an to experiment with some new trafficking routes via West estimated consumption of 157 mt of cocaine, equivalent Africa. In a few years, they managed to undermine secu- to 36% of global consumption, which is still higher than rity and sow high-level corruption in a number of West the cocaine consumption of West and Central Europe. Recognizing the threat, the international community undertook a variety of interventions to Cocaine consumption in volume terms appears to have address this flow. The novelty aspect was lost, the politi- declined by more than 40% over the 1999-2009 period cal instability proved self-defeating, and some very large in the United States to some 157 mt (range: 133-211 seizures were made. By 2008, there was a remarkable mt), with most of the decline (more than a third) having decline in the number of both large maritime seizures taken place between 2006 and 2009. As compared to and the number of cocaine couriers detected flying from estimates for 1989, cocaine consumption in the United West Africa to Europe. Criminal intelligence work indi- States seems to be now some 70% lower (range: -63% cates that the flow may have declined, but it did not to -77%), in parts reflecting the increase in treatment stop. This raises the possibility that traffickers had and successes in prevention, while the latest decline over simply modified their techniques, finding new methods the 2006-2009 period was attributed more to reduced for bringing cocaine to Europe, including through West supply. Statistical data support this scenario: European cocaine seizures decreased from 121 mt in 2006 to 57 mt in 2009. Best estimates Users Per capita use Consumption Region/subregion in % of in metric in % of in million grams per year total tons total Americas 8. From 2005 to 2008, a series of (range: 57-79 mt) to 123 mt in 2009 (range: 100-142 very large cocaine seizures took place in or near West mt). Many of these involved ‘mother ships’ inter- stabilized, and between 2007 and 2009, it may have cepted by European navies.
Generic evista 60 mg otc
If we are able to communicate women's health center white plains md buy evista 60 mg line, we let the professionals treating us know that we are recovering addicts womens health boutique oklahoma city evista 60 mg buy mastercard. We accept that we are not in control of the situation and trust the professionals who are treating us menopause reset evista 60 mg purchase free shipping. It is helpful to remember that the principles of recovery apply to every area of our life, even in a crisis. I explained my addiction to the doctor and asked if not taking the medication would be life-threatening. When we break a bone, experience a high fever, or cut ourselves, we may require emergency care. Relying on others can help alleviate the fear and irrational thinking that we may experience during a medical emergency. However, in some circumstances, we may be involved in an accident or traumatic injury and be forced to act very quickly. During these times we rely on our Higher Power for guidance and maintain our faith. When we are faced with a medical emergency, we can tap into the spiritual connection we have developed with a Higher Power through the steps. The Basic Text tells us that the power that brought us to the program is still with us and will continue to guide us if we allow it. The presence of people we trust and faith in a Higher Power are both valuable tools. The strength we gain from this support can help us 25 make decisions that will enhance our recovery. Relying on others alleviates the fear and irrational thinking that come with isolation. The spiritual connection we have developed with a Higher Power helps guide our decisions and provides a source of strength. A chronic illness is a persistent, often life-threatening, and incurable condition. Our experience is that chronic illnesses may have periods of remission and recurrence. Regardless of our particular circumstances, we apply the spiritual principles of our program to living with our chronic illness. Our attitude will either hurt or help us; we remind ourselves that 26 Through ongoing surrender, we can find freedom and the ability to accept our illness. In fact, our survival and recovery depend on our mental, emotional, and spiritual well-being. There are many chronic illnesses that our members live with that have treatments available. Our experience shows that sometimes the treatments can present their own set of challenges. Other days will seem less painful and more positive as we learn to continually surrender. Through ongoing surrender, we can find freedom and the ability to accept our illness. We give ourselves permission to feel exactly as we do, and to look for ways to cope, not escape. We can see our illness as a curse, or we can choose to view it as a gift that can bring us closer to our Higher Power and loved ones. We make a conscious decision to walk through our lives in a manner that will strengthen our commitment to our health and recovery. By renewing our commitment to turn our will and our lives over to our Higher Power’s care, we open a channel that allows this Power to work in our lives. Reaching out to others who are willing to listen to us share about our chronic illness will help us to realize that we are not alone.
Diseases
- Schizophrenia, genetic types
- Epilepsy progressive myoclonic
- MPO deficiency
- Myelitis
- Crossed polydactyly type 1
- O Doherty syndrome
- Precocious epileptic encephalopathy
- MOMO syndrome
- Meacham Winn Culler syndrome
Purchase evista now
The medical prescrip- tion model is the only real quasi-exception to this rigid rule menstrual migraines symptoms 60 mg evista purchase overnight delivery; as such menstruation clots order discount evista, it exists as an island of regulated production and supply women's health center at presbyterian dallas 60 mg evista sale, albeit within very narrow parameters. Beyond this there is zero fexibility for any 3 The conventions also control the medical uses of listed drugs, such as opiates for pain control. Furthermore, this absolute legal barrier creates genuine political obstacles to even discussing or proffering such policy alterna- tives. Defenders of the status quo often adopt dogmatic and entrenched moral positions, portraying regulatory legal alternatives as immoral, 6 extreme, ‘pro-drug’, radical, or even heretical. The clear implication is that debating such alternatives is a political ‘no-go’ zone. Until relatively recently, the climate of fear thus created had pushed the law reform position to the margins of mainstream political discourse. To the rational public health or social policy pragmatist, exploring and seeking out policy options that will deliver the best policy outcomes—an optimum point along this drug policy continuum—the idea that such an arbitrary barrier to policy research and development exists is diffcult to justify. This is especially true given that the vast majority of markets for goods and services, particularly ones that involve risk or poten- tial harm (including many hundreds of medical and non-medical psychoactive drugs), are both legally available and regulated by governments. Legal regulation of potentially risky A wide range of evidence based regulatory mecha- goods and activities is nisms and related enforcement/oversight agencies demonstrably not only are deployed to control and manage producers, the norm; it is one of suppliers, environments, products and consumers. For even the exploration of any such regulatory options to be forbidden in one, relatively narrow, feld of human behaviour does not sit well with the wider commitment of the United Nations to ‘promote social progress and better standards of life 7 in larger freedom’. Activities that take place beyond the parame- ters of a given regulatory framework remain prohibited and subject to legal sanctions. With the possible exception of some very low risk products such as coffee or coca tea, such models are not appropriate for drugs, because they forgo the potential for most forms of responsible state intervention in market regulation and control. In this, they are handing control of drug markets to exploit- ative profteers just as surely as prohibition. Legal commercial actors—whose primary concern is proft maximisation—would be free to aggressively promote consumption through marketing and advertising. The potential for such an approach to create unacceptable public health costs has been all too clearly demonstrated with the example of the free markets for tobacco in much of the developed world during the frst 60 years of the 20th century, and to a greater extent in large parts of the developing world today (see: 5. Nadelmann ‘Thinking Seriously About Alternatives to Drug Prohibition’, Daedalus, 1992, 121: pages 87–132. We describe them below, starting with the most restrictive and moving to the most open. Variants on these models already exist and function across the world, supporting the entirely legal distribution of a range of medical, quasi-medical and non-medical psychoactive drugs. Of course, the precise nature of the respective regulatory frameworks and enforcement infrastructure varies from country to country. This leads to a certain amount of generalisation, but also helps emphasise that such models will inevitably operate differently in different locations. We have also made some basic suggestions as to how to adapt these basic models to cater for the challenges of non-medical drug supply in the future. Under this model, drugs are prescribed to a named user by a qualified and licensed medical practitioner. They are dispensed by a licensed practitioner or pharmacist from a licensed pharmacy or other designated outlet. These guide, oversee and police the prescribing doctors and dispensing pharmacists. They also help determine which drugs are available, in what form, where, and under what criteria. It is limited to medical necessity, which restricts its actual or poten- tial use to the problematic/chronic dependent end of the drug use 9 spectrum. Most commonly, it supports maintenance prescribing as part of a treatment regimen or harm reduction programme. As such it will only ever involve a small fraction of the total drug using population, although it should be noted that this user group is disproportionately associated with the greatest personal and 10 societal harms (especially under prohibition ). Prescribed injectable heroin (diamorphine) also has a long history, and established evidence 11 base.
Discount evista 60 mg on line
Treatment with azoles results in relief of symptoms or Gram stain of vaginal discharge demonstrates budding and negative cultures in 80%–90% of patients who yeasts menstrual like cramps at 34 weeks cheap evista 60 mg buy online, hyphae womens health practice champaign il discount evista 60 mg on-line, or pseudohyphae or 2) a culture or other test complete therapy news articles on women's health issues evista 60 mg buy with amex. However, to maintain clinical and mycologic control, some Follow-Up specialists recommend a longer duration of initial therapy Follow-up typically is not required. If this regimen is not feasible, topical treatments used A minority of male sex partners have balanitis, characterized intermittently can also be considered. These men benefit from treatment of women will have recurrent disease after maintenance therapy with topical antifungal agents to relieve symptoms. Symptomatic women who remain culture- positive despite maintenance therapy should be managed in Special Considerations consultation with a specialist. Oral azoles occasionally excoriation, and fissure formation) is associated with lower cause nausea, abdominal pain, and headache. Therapy with clinical response rates in patients treated with short courses the oral azoles has been associated rarely with abnormal of topical or oral therapy. Clinically important interactions 150 mg of fluconazole in two sequential oral doses (second can occur when oral azoles agents are administered with other dose 72 hours after initial dose) is recommended. Options include longer duration of therapy becoming more common in vaginal isolates (723,724), (7–14 days) with a nonfluconazole azole regimen (oral or susceptibility testing is usually not warranted for individual topical) as first-line therapy. This regimen has clinical and Recurrent Vulvovaginal Candidiasis mycologic eradication rates of approximately 70% (726). Delay in diagnosis and treatment probably not differ from that for seronegative women. Although contributes to inflammatory sequelae in the upper reproductive long-term prophylactic therapy with fluconazole at a dose tract. Laparoscopy can be used to obtain a more accurate of 200 mg weekly has been effective in reducing C. Although some cases • elevated C-reactive protein; and are asymptomatic, others are not diagnosed because the patient • laboratory documentation of cervical infection with or the health-care provider fails to recognize the implications N. Diagnosis • endometrial biopsy with histopathologic evidence of and management of other common causes of lower abdominal endometritis; pain (e. After deciding clinical and microbiologic cure in randomized clinical trials whether to initiate empiric treatment, clinicians should also with short-term follow-up (741,742). Treatment should be initiated as soon as the doxycycline should be administered orally when possible. The decision of whether hospitalization used 24–48 hours after clinical improvement to complete the is necessary should be based on provider judgment and whether 14 days of therapy for the clindamycin/gentamicin regimen, the woman meets any of the following suggested criteria: and oral therapy with clindamycin (450 mg orally four times • surgical emergencies (e. However, when tubo-ovarian • pregnancy; abscess is present, clindamycin (450 mg orally four times daily) • severe illness, nausea and vomiting, or high fever; or metronidazole (500 mg twice daily) should be used to • unable to follow or tolerate an outpatient oral regimen; complete at least 14 days of therapy with doxycycline to provide or more effective anaerobic coverage than doxycycline alone. Limited data are available to support use of other parenteral No evidence is available to suggest that adolescents have second- or third-generation cephalosporins (e. In addition, these cephalosporins are and the clinical response to outpatient treatment is similar less active than cefotetan or cefoxitin against anaerobic bacteria. Ampicillin/sulbactam plus doxycycline has been investigated Parenteral Treatment in at least one clinical trial and has broad-spectrum coverage (744). Ampicillin/sulbactam plus doxycycline is effective Several randomized trials have demonstrated the efficacy against C. In women with tubo-ovarian abscesses, at least followed by 250 mg orally for 5–6 days) or combined with 24 hours of inpatient observation is recommended. Clin Infect Dis completed, symptoms have resolved, and sex partners have been 2007;28[Supp 1]:S29–36). Cefoxitin, a second-generation cephalosporin, has Follow-Up better anaerobic coverage than ceftriaxone, and in combination with probenecid and doxycycline has been effective in short- Women should demonstrate clinical improvement (e. Ceftriaxone defervescence; reduction in direct or rebound abdominal has better coverage against N. If retesting at 3 months is not for 1–2 doses, followed by 250 mg orally daily for 12–14 days) possible, these women should be retested whenever they next or in combination with metronidazole (745), and in another present for medical care in the 12 months following treatment. However, the woman should treating male partners of women who have chlamydia or receive treatment according to these recommendations and gonococcal infections (see Partner Services) (93,94). If no clinical improvement should be instructed to abstain from sexual intercourse until occurs within 48–72 hours of initiating treatment, providers they and their sex partners have been adequately treated (i.
Buy evista overnight delivery
The patient’s living sit- may have irregular and unpredictable meal Insulin Secretagogues uation must be considered breast cancer hair bows buy evista american express, as it may consumption menstrual cramps 6 weeks pregnant evista 60 mg order mastercard, undernutrition menstrual period tracker buy evista now, anorexia, Sulfonylureas and other insulin secreta- affect diabetes management and sup- and impaired swallowing. Social and instrumental support therapeutic diets may inadvertently mia and should be used with caution. Diets tailored to a pa- ide is a longer-duration sulfonylurea and with diabetes should be included in di- tient’s culture, preferences, and per- contraindicated in older adults (29). Incretin-Based Therapies life, satisfaction with meals, and nutri- Older adults in assisted living facilities Oral dipeptidyl peptidase 4 inhibitors tion status (35). A systematic ing centers) may rely completely on the especially vulnerable to hypoglycemia. Those re- They have a disproportionately high agents do not increase major adverse ceiving palliative care (with or without number of clinical complications and co- cardiovascular events (30). Diabetologia 2005;48:2460–2469 Providers may make adjustments to cause gastrointestinal symptoms such 5. Neurology vided they are given timely notification symptoms progress, some agents may 2014;82:1132–1141 6. Uncontrolled diabetes increases The following alert strategy could be Strata have been proposed for diabe- the risk of Alzheimer’s disease: a population- considered: tes management in those with advanced based cohort study. Intranasal glucose values should be confirmed focus on the prevention of hypogly- insulin therapy for Alzheimer disease and am- by laboratory glucose measurement. There is disease: a review of basic research and clinical men may need to be adjusted), b) glu- very little role for A1C monitoring evidence. Antidiabetic drugs and their potential role in treating mild cognitive glucose values greater than 300 mg/dL venting hypoglycemia is of greater impairment and Alzheimer’sdisease. Dehydration must be Med 2013;16:277–286 days, d) when any reading is too high, prevented and treated. Diabe- or e) the patient is sick, with vomit- with type 1 diabetes, insulin admin- tes, glucose control, and 9-year cognitive de- ing or other malady that can reflect istration may be reduced as the oral cline among older adults without dementia. Arch Neurol 2012;69:1170–1175 hyperglycemic crisis and may lead to intake of food decreases but should 12. The management of the older adult at upper level of the desired target Guidelines for managing Alzheimer’sdisease: the end of life receiving palliative range. J Am Geriatr Soc 2005;53:695–699 hyperglycemia, and dehydration) and likely to have any oral intake. Cognitive aging: preservation of dignity and quality-of- patients with type 1 diabetes, there progress in understanding and opportunities life in patients with limited life ex- is no consensus, but a small amount for action [Internet]. Accessed 3 October 2016 right to refuse testing and treatment, levels and prevent acute hyperglyce- 16. The burden decision process may need to involve Depression and all-cause mortality in persons and treatment of diabetes in elderly individuals the patient, family, and caregivers, lead- with diabetes mellitus: are older adults at in the U. Diabetes Care 2006;29:2415–2419 ing to a care plan that is both convenient higher risk? J Am Ger- Frailty in older adults: a nationally representa- and effective for the goals of care (39). Diabe- Biol Sci Med Sci 2015;70:1427–1434 oral agents as first line, followed by a tes in older adults. If needed, 2650–2664 cemia and incidence of frailty and lower S104 Older Adults Diabetes Care Volume 40, Supplement 1, January 2017 extremity mobility limitations in older women. Prac- complexityin middle-aged andolder adultswith ety 2012 Beers Criteria Update Expert Panel. American Geriatrics Society updated Beers Cri- individualized nutrition approaches for older Med Care 2010;48:327–334 teria for potentially inappropriate medication adults in health care communities. Update on diabetes in the elderly and in ment of the American Diabetes Association. Brussels,Belgium,Interna- relates of quality of life in older adults with di- care. J Pain Symptom Manage 2006;32:275–286 tional Diabetes Federation, 2013 abetes: the Diabetes & Aging Study.
Generic evista 60 mg with amex
In the majority of cases of persistent fever pregnancy journal online evista 60 mg purchase mastercard, however menstrual vitamins buy generic evista on-line, no other pathogen is identifed after parasite clearance women's health issues australia buy discount evista 60 mg on-line. Antibiotic treatment should be based on culture and sensitivity results or, if not available, local antibiotic sensitivity patterns. In a large, double-blind, placebo- controlled evaluation of a single prophylactic intramuscular injection of 20 mg/kg bw of phenobarbital to children with cerebral malaria, the frequency of seizures was reduced but the mortality rate was increased signifcantly. This resulted from respiratory arrest and was associated with additional use of benzodiazepine. A 20 mg/kg bw dose of phenobarbital should not be given without respiratory support. It is not known whether a lower dose would be effective and safer or whether mortality would not increase if ventilation were given. In the absence of further information, prophylactic anticonvulsants are not recommended. In addition, use of corticosteroids increases the risk for gastrointestinal bleeding and seizures and has been associated with prolonged coma resolution times when compared with placebo. Maternal mortality is approximately 50%, which is higher than in non-pregnant adults. Parenteral antimalarial drugs should be given to pregnant women with severe malaria in full doses without delay. If artesunate is unavailable, intramuscular artemether should be given, and if this is unavailable then parenteral quinine should be started immediately until artesunate is obtained. Obstetric advice should be sought at an early stage, a paediatrician alerted and blood glucose checked frequently. Hypoglycaemia should be expected, and it is often recurrent if the patient is receiving quinine. Postpartum bacterial infection is a common complication and should be managed appropriately. Prompt effective treatment and case management should be the same as for severe P. A full course of radical treatment with primaquine should be given after recovery. The displacement of large numbers of people with little or no immunity within malaria-endemic areas increases the risk for malaria epidemics among the displaced population, while displacement of people from an endemic area to an area where malaria has been eliminated can result in re-introduction of transmission and a risk for epidemics in the resident population. Climate change may also alter transmission patterns and the malaria burden globally by producing conditions that favour vector breeding and there by increasing the risks for malaria transmission and epidemics. If diagnostic testing is not feasible, the most practical approach is to treat all febrile patients as suspected malaria cases, with the inevitable consequences of over-treatment of malaria and potentially poor management of other febrile conditions. If this approach is used, it is imperative to monitor intermittently the prevalence of malaria as a true cause of fever and revise the policy appropriately. This is not the same as and should not be confused with “mass drug administration”, which is administration of a complete treatment course of antimalarial medicines to every individual in a geographically defned area without testing for infection and regardless of the presence of symptoms (see section 10). Active case detection should be undertaken to ensure that as many patients as possible receive adequate treatment, rather than relying on patients to come to a clinic. In humanitarian emergencies, when there are many patients and many present late, effective triage, with immediate resuscitation and treatment, are essential. In epidemic situations, severe malaria is often managed in temporary clinics or in situations in which staff shortages and the high workload make intensive case monitoring diffcult. If adequate records are kept, therapy can be given in the post-epidemic period to patients who have been treated with blood schizontocides. The strategy of using a single dose of primaquine to reduce infectivity and thus P. The population benefts of reducing malaria transmission by gametocytocidal drugs require that a high proportion of patients receive these medicines. A recent review of the evidence on the safety and effectiveness of primaquine as a gametocytocide of P. The particular advantage of artemisinins over other antimalarial drugs is that they kill circulating ring-stage parasites and thus accelerate therapeutic responses.
Lily-Of-The-Valley. Evista.
- What is Lily-of-the-valley?
- Are there safety concerns?
- Are there any interactions with medications?
- Heart arrhythmias and other heart problems, urinary tract infections (UTIs), kidney stones, weak contractions in labor, epilepsy, fluid retention, strokes, paralysis, infection of eye (conjunctivitis), and leprosy.
- How does Lily-of-the-valley work?
- Dosing considerations for Lily-of-the-valley.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96312
Cheap evista 60 mg on-line
Moreover menopause 2 periods in one month discount evista 60 mg buy line, the sale of controlled pharmaceuticals outside the legally established framework of bona fide pharmacies constitutes a criminal offence pregnancy levels generic evista 60 mg buy on-line. The online sale of such pharma- ceuticals by unscrupulous racketeers is no different from the trafficking in illicit drugs women's health clinic uf generic evista 60 mg free shipping, as it endangers lives just as much as street sales do. Preventive measures need to be taken to stop the further proliferation of illegally operating Internet pharmacies and to reduce their number. The Board hopes and expects that such cooperation will better protect the public against the illegal distri- bution of pharmaceuticals and, in particular, of controlled substances. The need for collaboration was the main reason why the Board developed the present guidelines, which have been elaborated with the support and contribution of national experts and relevant international organizations, Internet service providers, financial services and pharmaceutical associations. The Board hopes that the guidelines will serve as a starting point for the kind of successful inter- national cooperation that will, in the long term, lead to a successful international agreement on the matter. Hamid Ghodse President International Narcotics Control Board iv Contents Page Foreword. Description of the problem The World Wide Web provides valuable services to a growing commu- nity of users. More and more people are accessing online medical ser- vices, including for the supply of pharmaceuticals by duly licensed and legally operating Internet pharmacies. Such Internet-based services are an important complement to the services provided by the traditional health-care system, in particular for people in remote areas with limited access to medical services. Among the many well-known criminal activities involving the Internet, drug trafficking has reached major dimensions. Internet-based drug trafficking includes the sale of illicit drugs and, increasingly, the illegal sale of pharmaceuticals containing narcotic drugs and psychotropic sub- stances. Those pharmaceuticals, which have a high abuse potential, have become a significant problem in many countries because they have partly replaced traditional drugs of abuse. In several countries, the abuse of prescription drugs has become a major problem, second only to the abuse of cannabis. The illegal sale of pharmaceuticals is facilitated by websites that present themselves as Internet pharmacies and supply controlled narcotic drugs and psychotropic substances without meeting the legal and administra- tive requirements established for traditional pharmacies. In such cases, the term “Internet pharmacy” is misleadingly used to imply that a bona fide pharmacy is carrying out the transaction. However, in most cases such Internet pharmacies have no physical or legal connection with a legal pharmacy and should, in fact, not be considered pharmacies at all. Many of these virtual enterprises are owned by criminal networks and have various branches that deal, for example, in the illegal acquisition and supply of medicines, the provision of sham prescriptions and the smuggling of drugs. In recent years, the volume of illicit sales of narcotic drugs and psycho- tropic substances through websites has risen, making the Internet a major source of drugs for drug abusers. Many of the drugs are addic- tive; some are highly potent and their abuse can have fatal consequences. Particular concern has been expressed with regard to the ease with which children and adolescents can obtain such drugs, using the anonymity afforded to them by the Internet. In addition, the quality of medicines purchased illegally through Internet pharmacies and other websites 1 2 Guidelines for Governments on Preventing the Illegal Sale of Internationally Controlled Substances through the Internet cannot be guaranteed and customers risk purchasing medicines that are counterfeit products. Internet pharmacies operate through websites hosted by servers located all over the world. The problem is of a global nature and constitutes a new challenge in terms of investigative and preventive efforts. Treaty background The International Narcotics Control Board, which was established by the Single Convention on Narcotic Drugs of 1961,1 is responsible for promoting Governments’ compliance with the international drug control treaties and for monitoring the international drug control system, in accordance with the provisions of those treaties. In its resolution 50/11, the Commission encouraged Member States to notify the Board, in a regular and standardized manner, of seizures of internationally controlled licit substances ordered via the Internet and delivered through the mail, in order to fully assess trends relevant to the issue. In that same resolution, the Commission also encouraged the Board to continue its work with a view to raising awareness of and preventing the misuse of the Internet for the illegal supply, sale and distribution of such substances. It applies to pharmaceutical products containing those substances and to the raw materials. See also the definition provided in the glossary contained in the annex to the present document.
Evista 60 mg purchase online
Core team Laboratory and Scientific Section Justice Tettey menstrual joke purchase evista 60 mg without prescription, Jakub Gregor menstruation etymology buy evista 60 mg with mastercard, Beate Hammond and Yen Ling Wong women's health clinic dc generic 60 mg evista with amex. Statistics and Surveys Section Angela Me, Coen Bussink, Philip Davis, Kamran Niaz, Preethi Perera, Catherine Pysden, Umidjon Rahmonberdiev, Martin Raithelhuber, Ali Saadeddin, Antoine Vella and Cristina Mesa Vieira. Studies and Threat Analysis Section Thibault Le Pichon, Hakan Demirbüken, Raggie Johansen, Anja Korenblik, Suzanne Kunnen, Kristina Kuttnig, Renee Le Cussan and Thomas Pietschmann. The production of the World Drug Report 2011 was coordinated by Sandeep Chawla, with the support of the Studies and Threat Analysis Section. At the same time, we must reinforce our commit- heroin and cocaine production levels remain high. Its analysis of trends and emerging chal- duction of opium rose almost 80 per cent, which makes lenges informs national and international drug and the 2010 production decline less significant over the last crime priorities and policies, and provides a solid foun- decade. Meanwhile, the market for cocaine has not dation of evidence for counternarcotics interventions. Thus ago, the North American market for cocaine was four the more comprehensive the drug data we collect and times larger than that of Europe, but now we are wit- the stronger our capacity to analyse the problem, the nessing a complete rebalancing. Today the estimated better prepared the international community will be to value of the European cocaine market ($33 billion) is respond to new challenges. Recent trends Drug trafficking, the critical link between supply and Despite increased attention to drug demand reduction demand, is fuelling a global criminal enterprise valued in in recent years, drug use continues to take a heavy toll. There organized criminals are forming transnational networks, continues to be an enormous unmet need for drug use sourcing drugs on one continent, trafficking them across prevention, treatment, care and support, particularly in another, and marketing them in a third. Children enormous amounts of money controlled by drug traf- whose parents take drugs are themselves at greater risk fickers, they have the capacity to corrupt officials. Drugs generate recent years we have seen several such cases in which crime, street violence and other social problems that ministers and heads of national law enforcement agen- harm communities. In some regions, illicit drug use is cies have been implicated in drug-related corruption. Heroin consumption has stabilized in Europe and cocaine consumption has declined in North America – A stronger multilateral response to illicit drugs the most lucrative markets for these drugs. But these In the face of such diverse and complex challenges, we gains have been offset by several counter-trends: a large must improve the performance of our global response to increase in cocaine use in Europe and South America illicit drugs. Its provisions remain sound 8 and highly relevant, as does its central focus on the pro- and their victims (drug users), and that treatment for tection of health. The international community must drug use offers a far more effective cure than punish- make more effective use of all three Drug Conventions ment. We are seeing progress in drug use prevention as well as the Conventions against Transnational Organ- through family skills training, and more attention is ized Crime and Corruption. As an essential part of demand reduction law enforcement and judicial networks, can strengthen efforts, we also need to more vigorously raise public transnational cooperation in investigating and prosecut- awareness about illicit drugs, and facilitate healthy and ing drug traffickers, combating money-laundering, and fulfilling alternatives to drug use, which must not be identifying, freezing and confiscating criminal assets. A comprehensive and integrated approach can also help Better data and analysis to enrich policy us to confront the global threat from drugs more effec- tively. Governments A lack of comprehensive data continues to obstruct our and civil society must work together. This strategy gaps are more prominent in some regions, such as Africa is already having some success against drugs originating and Asia, and also around new drugs and evolving con- in Afghanistan. States and international organizations to counter traffic More comprehensive data collection allows for more and in and consumption of Afghan opiates. Regional coun- better analysis, which in turn enriches our response to ternarcotics information-sharing and joint cooperation the world drug challenge. I urge countries to strengthen initiatives like the Triangular Initiative (involving their efforts to collect data on illicit drugs, and I encour- Afghanistan, the Islamic Republic of Iran and Pakistan), age donors to support those countries that need assist- the Central Asian Regional Information and Coordina- ance in these efforts. Building on the lessons of the Paris Pact, the Group of Eight, under the leadership of the French I would like to thank the teams of skilled surveyors who Presidency, recently launched an initiative to create a gather data on cultivation and production levels of illicit unified response to tackle the global cocaine market. The We also must ensure that supply and demand reduction information they collect is of strategic importance to the efforts work together rather than in parallel. On the efforts of both the Governments concerned and the supply side, if we are to make real progress against heroin international community to make our societies safer and cocaine, we must address illicit cultivation in a more from drugs and organized crime.
Purchase evista without a prescription
For example tamoxifen breast cancer jewelry wholesale purchase 60 mg evista mastercard, which has the highest low/high price ratio is not patented anymore and available from multiple sources pregnancy lower back pain generic evista 60 mg visa. These discrepancies indicate that greater price transparency can help procurement officials to make better choices menstrual irregularity causes evista 60 mg purchase free shipping. Officials can use the global market pricing information to select the best value for money and increase access to treatment for more eligible patients. Cases of specific cancer drugs In this section we will describe some of the cancer medications that have been the subject of controversy, mostly because of high pricing. We have selected proven effective treatments and a mix of older and more recent products: dasatinib, docetaxel, erlotinib, imatinib, letrozole and trastuzumab. Of these, only imatinib is included in the National List of Essential Medicines of India. Three of the six medicines, docetaxel, letrozole, and trastuzumab are medicines used in the treatment of breast cancer. Breast cancer is the fastest growing cancer in India, and worldwide the most common cancer in women. The difference between generic and originator prices is significant and shows that access to generic supply is key to lowering the cost of treatment. These price differences indicate that South Africa could create savings through price negotiations and better procurement. Trastuzumab - Roche (breast cancer) Trastuzumab is a biotechnology product (monoclonal antibody) indicated for the treatment of specific types of breast cancer. Trastuzumab is either prescribed as a monotherapy or as a combined/adjuvant therapy with other chemotherapeutic agents (cisplatin or docetaxel or paclitaxel). Trastuzumab was developed and patented by Genentech and is currently 60 marketed by Roche as Herceptin. This patent was not granted in India because the product was developed before 1995 when India did not grant patents for pharmaceutical products. In 2007, a secondary patent was granted in India to Genentech (the original developer, later acquired by Roche) on a composition of the drug. Roche did this after the Kolkata patent office had revoked patents related to 61,62 trastuzumab. Roche has entered into an agreement with the Indian generic manufacturer Emcure Pharmaceuticals Ltd. Technically Emcure’s product is not a biosimilar because it simply repackages the product produced by Roche. Roche has attempted to challenge the marketing of biosimilar trastuzumab quoting misrepresentation as ‘biosimilar Trastuzumab’ and ‘biosimilar version of Herceptin’ without following the ‘due process in accordance with the 66 guidelines for similar biologics’ for getting approvals in India. On 26 November Biocon and Mylan received marketing authorization in India for their biosimilar trastuzumab products which they each market under 67 separate brand names. In their application they point out that one possible supplier of trastuzumab suggested the drug could be manufactured for $31 per gram, or $242 per year, roughly 1 percent of the lowest Roche price. The current Roche prices range from $3,000 to 68 $9,000 per gram (1 gram of gold costs $42 – 4 November 2013). The Expert Committee considered the applications in detail and noted the high quality evidence showing relevant clinical benefits in support of both imatinib and trastuzumab but deferred the final specifications of the medicines and their inclusion until 69 the review of the section of cytotoxics is completed. In 2013, an estimated 232,340 women were diagnosed as having breast cancer in the United States, and an estimated 39,620 women died from breast cancer. A number of factors have been found to be associated with breast cancer, including family history, nulliparity (no pregnancies), early menarche (menstruation), advanced age, and personal history. Breast cancer can be suspected when a lump is found in the breast, when the breast has changed sizes, when there is discoloration of the skin of the 17 Access to Cancer Treatment: A study of medicine pricing issues with recommendations for improving access to cancer medication. Diagnosis begins with a professional medical history and physical examination, including breast examination. If breast cancer is suspected from these examinations, breast biopsy is carried out. Simply speaking, breast cancer is classified into 4 groups, beginning with very small cancers in group 1, larger cancers in groups 2 and 3, and cancers with local extension of the cancer or spread through the body (or inflammatory cancers) in group 4. In stage 4, that is, with cancer that has spread beyond the breast, surgery is of limited benefit.
Order evista with amex
Patient 16 (pneumonia) Tetracycline is not a good drug for children below 12 years of age menstrual cramps during pregnancy order evista from india, because it can cause discolouration of the teeth pregnancy blood test cheap evista 60 mg on-line. The drug may interact with milk and the child may have problems swallowing the large tablets pregnancy 6 weeks 6 days buy 60 mg evista mastercard. Good alternatives are 54 Chapter 8 Step 3: Verify the suitability of your P-drug cotrimoxazole and amoxicillin. Tablets or parts of tablets could be crushed and dissolved in water, which is cost-effective if you can clearly explain the 3 procedure to the parents. You could also prescribe a more convenient dosage form, such as a syrup, although this is more expensive. In all these patients your P-drug was not suitable, and in each case you had to change either the active substance or the dosage form, or both. Atenolol was contraindicated because of another disease (asthma); an inhaler was not suitable because the child was too young to handle it; acetylsalicylic acid was contraindicated because it affects the blood clotting mechanism and because the patient is pregnant; and tetracycline tablets were contraindicated because of serious side effects in young children, possible interactions with milk, and inconvenience as a dosage form. The aim of a dosage schedule is to maintain the plasma level of the drug within the therapeutic window. As in the previous step, the dosage schedule should be effective and safe for the individual patient. The window and/or plasma curve may have changed, or the dosage schedule is inconvenient to the patient. If you are not familiar with the concept of the therapeutic window and the plasma concentration-time curve, read Annex 1. Exercise: patients 17-20 Review for each of the following cases whether the dosage schedule is suitable (effective, safe) for the patient. Recently mild hypertension was diagnosed, and diet and general advice have not been sufficiently effective. You have been treating his pain successfully with your P-drug, oral morphine solution, 10 mg twice daily. Chronic rheumatic disease, treated with your P-drug, indometacin, 3 times 50 mg daily plus a 50 mg suppository at night. However, it should not be done with capsules nor with special tablets such as sugarcoated or slow-release preparations. He was on oral morphine solution, 15 mg twice daily, to which he had responded well. Your P-drug is amitriptyline, 25 mg daily initially, followed by a slowly rising dose till the drug is effective (with a maximum of 150 mg per day). These differences may influence the pharmaco- dynamics or pharmacokinetics of your P-drug. A change in pharmacodynamics may affect the level (position) or width of the therapeutic window (Figure 1; see also Annex 1). The therapeutic window reflects the sensitivity of the patient to the action of the drug. Changes in the therapeutic window are sometimes expressed as the patient being ‘resistant’ or ‘hyper-sensitive’. The only way to determine the therapeutic window in the individual patient is by trial, careful monitoring and logical thinking. In Patient 17 (diabetes) it is important to note that β-blockers counteract the effect of insulin. This means that higher concentrations of insulin are needed for the same effect: the therapeutic window for insulin shifts upwards. The plasma curve no longer matches the window, and the daily dose of insulin must be raised. For these two reasons you may decide to change to another drug group that does not affect glucose tolerance, e. Patient 18 (lung cancer) has probably become tolerant to morphine, as he responded well to the drug before. The therapeutic window is shifted upwards and the dose has to be raised, for example to 15 mg twice daily. In terminal patients drug absorption and metabolism may be so disturbed that even larger dosages (e. Changes in plasma concentration-time curve The plasma concentration-time curve may be lowered or raised, or the concentration may fluctuate outside the therapeutic window. In Patient 19 (pain at night) the plasma concentration of Figure 2: Slow fall in plasma concentration late at night indometacin probably falls below the therapeutic window in patient 19 early in the morning (see Figure 2).
Masil, 26 years: When illegible handwriting results in a breach of that duty, causing personal injury, then the courts will be prepared to punish the careless by awarding sufficient damages.
Sanuyem, 58 years: Examples bumetanide furosemide hydrochlorothiazide 11 metolazone triamterene triamterene + hydrochlorothiazide Interactions Food: Take your diuretic with food if it upsets your stomach.
Xardas, 31 years: Taking a medicine means remembering every day and may be also We have listed them as their “generic name” (the name of the actual drug).
Deckard, 30 years: Adverse events requiring reporting Local reactions » Severe local reaction (swelling extending > 5 cm from the injection site or redness and swelling for > 3 days).
Emet, 44 years: The largest improvement was in gut function (verified by pre and post endoscopies in many cases), but also improvements in other areas.
Bengerd, 33 years: In April 2010,88 Methamphetamine trafficking from Africa to Japan one methamphetamine laboratory was seized in Egypt.
Asaru, 62 years: Systematic review and meta-analysis of outcomes following emergency surgery for Clostridium difficile colitis.
Jesper, 64 years: Population pharmacokinetics of mefoquine, piperaquine and artemether–lumefantrine in Cambodian and Tanzanian malaria patients.
Muntasir, 23 years: We have evidence-based interventions that prevent harmful substance use and related problems, particularly when started early.
Jerek, 53 years: Some tests may help in diagnosing vaginal and urethral discharge, but they should never delay treatment (results 9 should be available within one hour).
Ortega, 38 years: Because this product contains estrogen, it is approved with the same Boxed Warning and other Warnings and Precautions that have been approved with estrogen products.
Zuben, 24 years: Antihypertensives are mainly classified at 3rd levels according to the mechanism of action.
Dennis, 32 years: The contract was reviewed at the end of the week to determine if the reinforcer had been earned.
Renwik, 55 years: Initial application — (collagenous and lymphocytic colitis (microscopic colitis)) from any relevant practitioner.
Riordian, 51 years: Feasibility of radical cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for pseudomyxoma peritonei of appendiceal origin.
Armon, 22 years: Then, if you happen to hit the wrong button on the calculator you are more likely to be aware that an error has been made.
Jensgar, 59 years: At a time when counterfeit pharmaceuticals are f looding the global market, Pfizer is trying to educate the public about the need for caution when purchasing their medicines and the importance of closing our borders to these potentially dangerous products.
Hogar, 46 years: Locally applied atropine or scopolamine produces ocular effects of considerable duration; accommodation and pupillary reflexes may not fully recover for 7 to 12 days.
8 of 10 - Review by U. Delazar
Votes: 317 votes
Total customer reviews: 317
References
- Rodman JS, Blackburn P, Williams JJ, et al: The effect of dietary protein on cystine excretion in patients with cystinuria, Clin Nephrol 22(6):273n278, 1984.
- Bruns TNC, Lauvetz RJ, Kerr ES, et al: Buschke-Lowenstein giant condylomas: pitfalls in management, Urology 5:773n776, 1975.
- Grewal J, McCully RB, Kane GC, et al: Left ventricular function and exercise capacity, JAMA 301:286- 294, 2009.
- Duldulao MP, Lee W, Streja L, et al. Distribution of residual cancer cells in the bowel wall after neoadjuvant chemoradiation in patients with rectal cancer. Dis Colon Rectum 2013;56(2):142-149.
- Larrabee, J., Ostrow, C. L., Withrow, M. l., Janney, M. A., Hobbs, G. R. Jr., & Burant, C. (2004). Predictors of patient satisfaction with inpatient hospital nursing care. Research in Nursing & Health, 27, 254-268.
- Overholt BF, Panjehpour M, Halberg DL: Photodynamic therapy for Barrett's esophagus with dysplasia and/or early stage carcinoma: Long-term results. Gastrointest Endosc 58:183, 2003.
- Friedrich EG: New nomenclature for vulvar disease, Obstet Gynecol 47:122n124, 1976.