Bradley G. Phillips, PharmD, BCPS, FCCP
- Milliken-Reeve Professor and Department Head, Clinical and Administrative Pharmacy, University of Georgia College of Pharmacy, Athens, Georgia

https://rx.uga.edu/faculty-member/bradley-g-phillips-pharm-d/
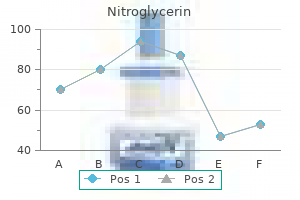
Nitroglycerin dosages: 6.5 mg, 2.5 mg
Nitroglycerin packs: 30 caps, 60 caps, 90 caps, 120 caps, 180 caps, 270 caps, 360 caps

Order genuine nitroglycerin
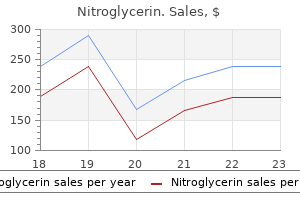
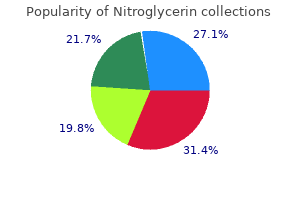
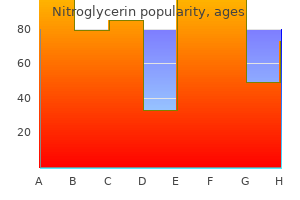
Belgium is an interesting case: it belongs to the countries with the highest rate of self-reported drink-driving and at the same time to the countries with the lowest rate of self-reported drug-driving treatment mrsa purchase 6.5 mg nitroglycerin otc. The countries with the highest proportions of drivers declaring that they had medicine examples cheap nitroglycerin uk, within the last year medicine reaction purchase 6.5 mg nitroglycerin with amex, driven under the influence of medication that may impair the driving ability are France (32%), Spain (24%) and Switzerland (23%) (Figure 14). The countries with the lowest percentages of self-declared driving under the influence of medication that may impair the driving ability are Denmark (12%), Italy (15%) and Sweden (16%). Note: Countries based on individual country weight, Europe based on European weight B. The percentages of persons declaring that they have driven under the influence of either of the three substances are clearly higher among men than women (Figure 15) for example, 38% of the men and ‘only’ 23% of the women have answered that they had driven under the influence of alcohol in the past 12 months. The differences between men and women is lower in the case of the self-declared driving under the influence of medication that may impair the driving ability than in the case of drink-driving or drug- driving. Over the last 30 days, how many times did 9% you drive a car, when you may have been over the legal limit for drinking and driving? Behaviours like drink-driving or drug-driving are clearly more frequently reported by young people (between 18 and 34 years old) than by the older age groups (Figure 16). The differences are especially notable in relation to drug-driving: 21% of the persons aged between 18 and 34 years and ‘only’ 4% of the persons aged 55 years or older reported that they had driven under the influence of drugs in the past 12 months. Perceived likelihood of being checked for impaired driving The perceived likelihood of getting caught for driving under the influence of alcohol or drugs is considered as an important issue. Several studies have shown that the perceived probability of being caught plays an important role in the prevention of drink-driving (Meesmann et al. In the general car driver population, the perceived likelihood of being checked for impaired driving is not especially high: only 18% think that on a typical journey, the probability of an alcohol test by the police is big or very big (Figure 17). The expectation that they could be controlled for drugs is even smaller: only 11% think that the chance of such a police control is big or very big. On a typical journey, how likely is it that you (as a driver) will be checked by the police for alcohol, in other words, being subjected to a Breathalyser 18% test? On a typical journey, how likely is it that you (as a driver) will be checked by the police for the use of illegal drugs? The answer patterns of the car drivers are very different according to the countries (Figure 18). The percentage of car drivers thinking that the chance of being checked for alcohol is big or very big is the highest in Poland (44%) and the smallest in Denmark (2%). In addition to Poland, France (29%), Slovenia (27%), Spain (24%), Portugal (23%) and Switzerland (19%) belong to the countries where the perceived likelihood of being checked for alcohol is above the European average (18%). Not only in Denmark, but also in Finland (4%), in Germany (8%), in the United Kingdom (9%), in Ireland (9%) and in the Netherlands (10%), the car drivers have a particularly low expectation of being checked for alcohol. In most countries where the expectation to be checked for alcohol is high, the anticipation of possible drugs controls is also rather high. In Poland, the gap between the perceived likelihood of being checked for alcohol (44%) and for drugs (16%) is quite big, but the anticipation of possible drug controls (16%) is still above the European average (11%). In the countries with low expectations of alcohol controls, the expectations for drug controls are even lower. There is also an association between the perceived likelihood of being checked for impaired driving and the level of enforcement in the different countries. This link is presented and discussed in the thematic report Enforcement and support for road safety policy measures. There is almost no difference between men and women concerning the perceived likelihood of being controlled for alcohol or drugs (Figure 19). The percentage of car drivers estimating that the chance of being checked is big or very big is slightly higher among women than men, but it is statistically not significant (p>. Female On a typical journey, how likely is it that you 12% Male (as a driver) will be checked by the police for the use of illegal drugs? The perceived likelihood of being controlled for alcohol or drugs clearly depends on the age groups (Figure 20). The younger the respondents, the more likely they are to expect a control for alcohol or for drugs. The differences between the age groups are more pronounced in the case of expected alcohol controls than of expected drugs controls. On a typical journey, how likely is it that you (as a 15% driver) will be checked by the police for alcohol, in 17% other words, being subjected to a Breathalyser test?
Nitroglycerin 6.5 mg purchase overnight delivery
Injectable products commercially injection into the eye must meet standards for “injectable” available for intrathecal injection typically do not contain drugs symptoms week by week nitroglycerin 6.5 mg order amex, the clinician is advised to maintain good access harmful preservatives symptoms xanax withdrawal buy discount nitroglycerin online. These are preferred wherever to professionals who are accustomed to handling and possible for intravitreal injection - but pay close attention to preparing these agents symptoms 24 safe 6.5 mg nitroglycerin. Central locations such as differences in concentration between products intended for hospital pharmacies have manuals with extensive data on parenteral vs intrathecal injection. These centres are more than happy to provide professional guidance, and are the A few cautionary statements starting place for inquiries into the safety of any proposed There are no short cuts to proper dilution, selection and injectable dose that is not clearly defned in the ophthalmic separation of antibiotics for intra-vitreal injection. For example, a mixture of because the commercial products used remain undiluted, ceftazidime 1mg/ml and vancomycin 20mg/ml are known along with the preservatives and other components. Aside to be compatible (assuming known vehicles), whereas, if from potential drug incompatibility issues, direct contact of the concentration of ceftazidime were to be increased to these concentrated solutions with internal parts of the eye 10, 50 or 200mg/ml, a physical incompatibility could occur is more likely to result in toxic effects. Understanding such principles and Only doses and agents proven safe for use in the eye (as limitations helps the surgeon to navigate the steps needed established in previous animal models) and substantiated to prepare injectables for delivery inside the eye. However, if the infection as the standard of care for treatment of endophthalmitis, is severe, the surgeon may use his judgment and add the value of added systemic antibiotics was questioned, systemic antibiotics, broad spectrum initially, and since animal experiments showed that very little, if any, subsequently according to bacterial susceptibility and antibiotic penetrated into the vitreous space from the patient safety. However, the study design used different drugs systemically (amikacin However, when clinical conditions were, in fact, duplicated and ceftazidime) from those used intravitreally (vancomycin in animal models, results showed a substantial rise in and ceftazidime), which does not contribute towards intravitreal antibiotic concentrations in the aphakic, maintaining effective antibiotic levels within the eye. Thus, adjunctive systemic antibiotic therapy levels from the intravitreal injection are beginning to decline. For fungal infection, intravitreal amphotericin (5-10 µg) or voriconazole (100 µg) are usually associated with administration of the same drug systemically. Intramuscular vs intravenous antibiotic injection An intravenous dose of antibiotic produces much higher instantaneous blood levels than does an intramuscular injection. This higher concentration gradient helps to drive antibiotic into tissues or spaces such as the vitreous. Therefore, intramuscular injection is not advised if intermittent intravenous dosing is feasible. Figure A shows poor vitreous penetration in non-infamed eyes, but a gradual increase in the presence of infammation. However, aphakia and vitrectomy (Figure B) increase penetration even more substantially. When the cephalosporins carry side chains (R1 side chains) different than the penicillin in question, the The prevalence of penicillin allergy has been variously chances of cross-reactivity are very low to negligible. The incidence of true penicillin cephalosporins because of their similar side chains, allergy, as confrmed by skin testing, in patients claiming may show cross-reactivity with penicillin. These do true allergy to penicillin involves IgE-mediated immunologic confer an increased risk of allergic reaction in patients who responses that may lead to anaphylaxis. These include penicillins and cephalosporins, and specifcally, the risk cefprozil, cefuroxime, ceftazidime, and ceftriaxone, of potential cross-allergenicity with cefuroxime. True cross-reactivity of concern is allergy to cephalosporins, not allergy to between penicillins and cephalosporins is now linked to penicillin. Rates of endophthalmitis with/without add-on antibiotic drops Postop Intracameral + Preop Topical +Postop Topical + Preop and Postop Endophthalmitis Antibiotics Only Antibiotics* Antibiotics† Antibiotics‡ Cases/total 98/396,894 8/47,574 2/10,382 3/7,307 Percentage 0. Two cases of anaphylaxis after use of intracameral If antibiotic drops are administered in the immediate cefuroxime have been reported. One patient, with a postoperative timeframe, many clinicians favor a vigorous history of allergy to amoxicillin, became hypotensive and approach initially, for a period of time, avoiding any diaphoretic; and recovered after treatment for anaphylaxis tapering of antibiotic drops to discourage development of (Villada 2005). Some surgeons prescribe frequent penicillin, complained of redness and pruritus in the arms postoperative antibiotics when complications occurred or while in the recovery room after phacoemulsifcation wound healing problems are anticipated. Currently, fuoroquinolone drops are favored agents in some areas due to their relatively broad spectrum, Few data exist to help defne the best options for ability to penetrate the corneal epithelium to some degree, postoperative antibiotic drop administration, although this and commercial availability. Recent data suggested that postoperative topical antibiotic drops confer no added beneft over intracameral cefuroxime injection in reduction of postoperative endophthalmitis Moxifoxacin vs Cefuroxime (Table 23). The 2013 report from the Swedish Cataract Register3 shows there was no statistical beneft from add- Choice of intracameral antibiotic: cefuroxime or on topical antibiotics, either preoperatively, postoperatively, fuoroquinolone?
Purchase cheap nitroglycerin on-line
Q12H Can be restarted a minimum of 2 Outpatients: 8 hours hours post-neuraxial anesthesia Heparin catheter placement symptoms 6 days after embryo transfer order nitroglycerin with a mastercard. Contact chondroitin symptoms 22 weeks pregnant generic nitroglycerin 6.5 mg on-line, dong quai symptoms checker cheap nitroglycerin 6.5 mg buy on line, evening Pharmacy Specialist for primrose, flaxseed, fish oil, garlic, 7 days Avoid while catheter is in place recommendation for specific medication ginger, ginko, ginseng, recommendation. For other agents that effect Factor Xa, the presence of an elevated Xa indicates presence of the medication and does not necessarily reflect the degree of anticoagulation. Regional anesthesia in the patient receiving antithrombotic therapy or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Interventional Spine and Pain Procedures in Patients on Antiplatelet and Anticoagulant Medications: Guidelines From the American Society of Regional Anesthesia and Pain Medicine, the European Society of Regional Anaesthesia and Pain Therapy, the American Academy of Pain Medicine, the International Neuromodulation Society, the North American Neuromodulation Society, and the World Institute of Pain. Ketorolac tromethamine pharmacokinetics and metabolism after intravenous, intramuscular, and oral administration in humans and animals. Long-term goals of treatment of schizophrenia include relapse prevention, recovery, improved adherence to therapy and improved patients’ quality of life. Antipsychotics in combination with other therapeutic interventions are considered essential for the achievement of these long-term goals. However, relevant issues relating to the pharmacotherapy of schizophrenia still remain unresolved. Poor adherence to antipsychotic therapy is an important factor that contributes to possible inadequacy of treatment. In recent years, the development of these formulations with atypical antipsychotics and the promising results obtained in well conducted trials with these compounds are changing the at- titudes towards these drugs, traditionally reserved to patients with long-term histories of non-adherence to treatment. The discovery and development of antipsychotic drugs more than 50 years ago has significantly improved the quality of life of patients with schizophrenia and currently there is little doubt about the substantial benefits of antipsychotics 1. Antipsychotic drugs are generally recom- mended for all stages of schizophrenia, for the treatment of acute epi- sodes of psychosis and for the prevention of recurrence 2. Important long-term goals of current treatment for schizophrenia include relapse prevention, recovery, improved adherence to therapy and improve pa- tients’ quality of life. Antipsychotics in combination with other therapeutic interventions are considered as essential for the achievement of these long-term goals. Several relevant issues relating to the pharmacotherapy of schizophre- nia – especially when starting treatment and for how long to continue it – still remain unresolved and often result in an inadequacy of treatment for many patients, such as its premature termination or delayed ac- cess to treatment 1. Poor adherence to antipsychotic therapy is another important factor that contributes to possible inadequacy of treatment 3. In Correspondence recent years the development of these formulations of atypical antip- sychotics and the promising results obtained in well conducted trials Emilio Sacchetti with these compounds are changing the attitude towards these drugs, emilio. In this regard, a recent observational community The importance of continuity cohort study conducted in Finland 10 investigated the of treatment risk of rehospitalization and medication discontinua- The course of schizophrenia is characterized in about tion in a nationwide cohort of 2,588 consecutive pa- three quarters of the cases by phases of remission tients with schizophrenia who were hospitalized for alternating with phases of relapse: after the first epi- the first time between 2000 and 2007. In addition, knowledge about dol, risperidone, perphenazine, zuclopenthixol) was the neurobiological basis of schizophrenia has pro- associated with substantially better outcomes than vided evidence of the often progressive nature of with the equivalent oral formulations. A lower recurrence rate and a higher percentage of ad- study published by Robinson et al. Discontinuation was associated with a significantly higher recurrence rate (43% vs. Based on evidence of clinical studies first episode schizophrenia who received mainte- showing that even those patients who have been sta- nance therapy for only one year. Recurrence rates ble on antipsychotics for the period of two to five years were significantly higher in the group receiving inter- after an acute episode relapse more frequently if they mittent treatment than in the group that received con- are taken off medication than if they continue it 14. However, it should be kept in mind that for at least two years after the first symptom remission, prompt recognition and correction of poor adherence while one should observe a minimum of five years of educational efforts directed to patients and to medi- stability without relapses before making a slow with- cal staff are also extremely useful 21. Poor adherence drawal of antipsychotic drugs over a 6-24 months in has been identified as an important risk factor for re- patients with a history of previous recurrences. Some studies have also suggested that chronic exposure to antipsychotics may contrib- Although atypical antipsychotics are widely used, the ute to the reduction of the volume of brain tissue founf debate over their alleged better tolerability compared in the disease 17. A meta-analysis patients with newly diagnosed schizophrenia verified by Leucht et al.
Nitroglycerin 6.5 mg buy otc
Place a closed fist in the pit of the stomach medicine hat jobs discount nitroglycerin 6.5 mg line, above the navel and below the ribs treatment regimen cheap nitroglycerin 2.5 mg without a prescription. Place the other hand over fist and press hard into the abdomen with a quick treatment in spanish nitroglycerin 6.5 mg purchase online, upward thrust. Perform one to five abdominal thrusts in order to compress the lungs from the below and dislodge the foreign body. With the heel of the other hand, perform one to five slaps on the back, between shoulder plates. Perform five forceful sternal compressions as in cardiopulmonary resuscitation: use 2 or 3 fingers in the center of the chest just below the nipples. Repeat until the foreign body is expelled and the patient resumes spontaneous breathing (coughing, crying, talking). If the patient loses consciousness ventilate and perform cardiopulmonary rescucitation. Differential diagnosis and management of airway obstructions of infectious origin Timing of Infections Symptoms Appearance symptoms Viral croup Stridor, cough and moderate Prefers to sit Progressive respiratory difficulty Epiglottitis Stridor, high fever and severe Prefers to sit, drooling Rapid respiratory distress (cannot swallow their own saliva) Bacterial Stridor, fever, purulent secretions Prefers to lie flat Progressive tracheitis and severe respiratory distress Retropharyngeal Fever, sore throat and painful Prefers to sit, drooling Progressive or tonsillar swallowing, earache, trismus abscess and hot potato voice – Croup, epiglottitis, and tracheitis: see Other upper respiratory tract infections. Management of other causes – Anaphylactic reaction (Quincke’s oedema): see Anaphylactic shock (Chapter 1) – Burns to the face or neck, smoke inhalation with airway oedema: see Burns (Chapter 10). Clinical features – Nasal discharge or obstruction, which may be accompanied by sore throat, fever, cough, lacrimation, and diarrhoea in infants. Treatment – Antibiotic treatment is not recommended: it does not promote recovery nor prevent complications. Most acute sinus infections are viral and resolve spontaneously in less than 10 days. Acute bacterial sinusitis may be a primary infection, a complication of viral sinusitis or of dental origin. The principal causative organisms are Streptococcus pneumoniae, Haemophilus influenzae and Staphylococcus aureus. It is essential to distinguish between bacterial sinusitis and common rhinopharyngitis (see Rhinitis and rhinopharyngitis). Without treatment, severe sinusitis in children may cause serious complications due to the spread of infection to the neighbouring bony structures, orbits or the meninges. Clinical features Sinusitis in adults – Purulent unilateral or bilateral discharge, nasal obstruction and – Facial unilateral or bilateral pain that increases when bending over; painful pressure in maxillary area or behind the forehead. Sinusitis is likely if symptoms persist for longer than 10 to 14 days or worsen after 5 to 7 days or are severe (severe pain, high fever, deterioration of the general condition). Sinusitis in children – Same symptoms; in addition, irritability or lethargy or cough or vomiting may be present. If the diagnosis is uncertain (moderate symptoms < 10 days) and the patient can be re- examined in the next few days, start with a symptomatic treatment, as for rhinopharyngitis or viral sinusitis. Other treatments – For sinusitis secondary to dental infection: dental extraction while under antibiotic treatment. The majority of cases are of viral origin and do not require antibiotic treatment. Group A streptococcus is the main bacterial cause, and mainly affects children age 3 to 14 years. Clinical features – Features common to all types of pharyngitis: throat pain and dysphagia (difficulty swallowing), with or without fever. Less common forms: • Vesicular pharyngitis (clusters of tiny blisters or ulcers on the tonsils): always viral (coxsackie virus or primary herpetic infection). Immunisation protects against the effects of the toxin but does not prevent individuals from becoming carriers. Close monitoring of the patient is essential, with immediate availability of equipment for manual ventilation (Ambu bag, face mask) and intubation, Ringer lactate and epinephrine. If there is no allergic reaction (no erythema at the injection site or a flat erythema of less than 0. Management of close contacts Close contacts include family members living under the same roof and people who were directly exposed to nasopharyngeal secretions of the patient on a regular basis (e. Treatment – In the absence of inspiratory stridor or retractions, treat symptomatically: ensure adequate hydration, seek medical attention if symptoms worsen (e. Monitor heart rate during nebulization (if heart rate greater than 200, stop the nebulization). Age 3 months 4-6 months 7-9 months 10-11 months 1-4 years Weight 6 kg 7 kg 8 kg 9 kg 10-17 kg Dose in mg 3 mg 3.
Cheap 2.5 mg nitroglycerin
Identifcation medications safe during pregnancy buy nitroglycerin 6.5 mg with visa, prevention symptoms after embryo transfer nitroglycerin 2.5 mg low cost, and treatment revisited: Individual-focused college drinking prevention strategies 1999–2006 medicine side effects discount nitroglycerin online amex. Individual-level interventions to reduce college student drinking: A 1557 meta-analytic review. Screening and brief interventions for alcohol use in college health centers: A review. Face-to-face versus computer-delivered alcohol interventions for college drinkers: A meta-analytic review, 1998 to 2010. Defning and characterizing differences in college alcohol intervention efcacy: A growth mixture modeling application. Indicated prevention for college student marijuana use: A randomized controlled trial. Single-session alcohol interventions for heavy drinking college students: A systematic review and meta-analysis. Efcacy of expectancy challenge interventions to reduce college student drinking: A meta-analytic review. Brief motivational interventions for college student drinking may not be as powerful as we think: An individual participant‐level data meta‐analysis. Brief motivational and parent interventions for college students: A randomized factorial study. Efcacy of alcohol interventions for frst-year college students: A meta-analytic review of randomized controlled trials. A randomized clinical trial evaluating a combined alcohol intervention for high-risk college students. Evaluating the effects of a brief motivational intervention for injured drinkers in the emergency department. Prevention interventions of alcohol problems in the workplace: A review and guiding framework. The effectiveness of limiting alcohol outlet density as a means of reducing excessive alcohol consumption and alcohol-related harms. Case closed: Research evidence on the positive public health impact of the age 21 minimum legal drinking age in the United States. Youth problem behaviors 8 years after implementing the Communities That Care prevention system: A community-randomized trial. Sustained decreases in risk exposure and youth problem behaviors after installation of the Communities That Care prevention system in a randomized trial. Enhanced enforcement of laws prohibiting sale of alcohol to minors: Systematic review of effectiveness for reducing sales and underage drinking. The state sets the rate: The relationship among state-specifc college binge drinking, state binge drinking rates, and selected state alcohol control policies. Youth drinking in the United States: Relationships with alcohol policies and adult drinking. Evidence for the effectiveness and cost-effectiveness of interventions to reduce alcohol-related harm. The affordability of alcoholic beverages in the European Union: Understanding the link between alcohol affordability, consumption and harms. Effects of alcohol tax and price policies on morbidity and mortality: A systematic review. Drinking, driving, and deterrence: The effectiveness and social costs of alternative policies. Multilevel spatiotemporal change-point models for evaluating the effect of an alcohol outlet control policy on changes in neighborhood assaultive violence rates. Effectiveness and cost-effectiveness of policies and programmes to reduce the harm caused by alcohol. Changes in density of on-premises alcohol outlets and impact on violent crime, Atlanta, Georgia, 1997– 2007. Multilevel spatio-temporal dual changepoint models for relating alcohol outlet destruction and changes in neighbourhood rates of assaultive violence.
Syndromes
- Non-pitting edema does not leave this type of dent when pressing on the swollen area.
- Excessive bleeding
- Fluid buildup in the chest (called a pleural effusion) due to bleeding into the chest, buildup of fatty fluid, abscess or pus buildup in the lung or the chest, or heart failure
- Shortness of breath and less ability to exercise (heart transplant)
- Cramping pain in the belly area
- Lung cancer
- ESR (sed rate)
- Spinal tap
- Sluggishness
- Overactive thyroid (hyperthyroidism)
2.5 mg nitroglycerin order visa
A more complete description of the disorder medications dictionary nitroglycerin 6.5 mg visa, including its clinical features treatment variance purchase discount nitroglycerin online, assessment medications in carry on luggage cheap nitroglycerin 6.5 mg line, differential diagnosis, epidemiology, and natural history and course, is provided in Part B of this guideline. This guideline reviews the treatment that patients with borderline personality disorder may need. Psychiatrists care for patients in many different settings and serve a variety of functions and thus should either provide or recommend the appropriate treatment for patients with bor- derline personality disorder. Therefore, psychiatrists caring for patients with borderline personality disorder should consider, but not be limited to , treatments recommended in this guideline. Diagnostic Criteria for Borderline Personality Disorder A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and marked impulsivity beginning by early adulthood and present in a variety of contexts, as indicated by five (or more) of the following: 1) Frantic efforts to avoid real or imagined abandonmenta 2) A pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation 3) Identity disturbance: markedly and persistently unstable self-image or sense of self 4) Impulsivity in at least two areas that are potentially self-damaging (e. Reprinted from Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision. Treatment of Patients With Borderline Personality Disorder 7 Copyright 2010, American Psychiatric Association. This guideline strives to be as free as possible of bias toward any theoretical approach to treatment. This practice guideline was developed under the auspices of the Steering Committee on Practice Guidelines. The sum- mary of treatment recommendations is keyed according to the level of confidence with which each recommendation is made. In addition, each reference is followed by a letter code in brack- ets that indicates the nature of the supporting evidence. The three categories represent varying levels of clinical confidence regarding the recommendation: [I] Recommended with substantial clinical confidence. It is characterized by marked distress and functional impairment, and it is associated with high rates of self-destructive behavior (e. The care of patients with borderline personality disorder involves a comprehensive array of approaches. This guideline presents treatment options and addresses factors that need to be considered when treating a patient with borderline personality disorder. The initial assessment The psychiatrist first performs an initial assessment of the patient to determine the treatment setting [I]. Because suicidal ideation and suicide attempts are common, safety issues should be given priority, and a thorough safety evaluation should be done. This evaluation, as well as con- sideration of other clinical factors, will determine the necessary treatment setting (e. It is important at the outset of treatment to establish a clear and explicit treatment frame- work [I], which includes establishing agreement with the patient about the treatment goals. Psychiatric management Psychiatric management forms the foundation of treatment for all patients. The primary treat- ment for borderline personality disorder is psychotherapy, complemented by symptom-targeted pharmacotherapy [I]. In addition, psychiatric management consists of a broad array of ongoing activities and interventions that should be instituted by the psychiatrist for all patients with borderline personality disorder [I]. Regardless of the specific primary and adjunctive treatment modalities selected, it is important to continue providing psychiatric management throughout the course of treatment. The components of psychiatric management for patients with border- Treatment of Patients With Borderline Personality Disorder 9 Copyright 2010, American Psychiatric Association. Principles of treatment selection a) Type Certain types of psychotherapy (as well as other psychosocial modalities) and certain psycho- tropic medications are effective in the treatment of borderline personality disorder [I]. Pharmacotherapy often has an important ad- junctive role, especially for diminution of symptoms such as affective instability, impulsivity, psychotic-like symptoms, and self-destructive behavior [I]. Flexibility is also needed to respond to the changing characteristics of patients over time. Treatment by multiple clinicians has potential advantages but may become frag- mented; good collaboration among treatment team members and clarity of roles are essential [I].
Buy nitroglycerin without a prescription
Clinical experience with intravenous quinine medications vs medicine purchase generic nitroglycerin canada, 5 intramuscular artemether and intravenous artesunate for the treatment of severe malaria in Thailand medications covered by blue cross blue shield nitroglycerin 6.5 mg order on-line. Artesunate versus quinine for treatment of severe falciparum malaria: a randomised trial medicine and manicures cheap nitroglycerin 2.5 mg buy online. Effcacy of rectal artesunate compared with parenteral quinine in initial treatment of moderately severe malaria in African children and adults: a randomised study. H3C Dose-dependent risk of neutropenia after 7-day courses of artesunate monotherapy in Cambodian patients with acute Plasmodium falciparum malaria. H3C H3C H3C F F Neuropathological assessment of artemether-treated severe malaria. The apparent clearance (Cl/f) of both atovaquone and proguanil is related to body weight (14). While most of the pharmacokinetics of proguanil and cycloguanil is comparable in adults and children, the elimination half-life of atovaquone is shorter in children (9, 14). The plasma concentrations of atovaquone and proguanil in women in the second A and third trimesters of pregnancy are approximately half those of non-pregnant 5 adults (with and without acute malaria) as a result of a greater Vd and increased oral clearance. Pharmacokinetic parameters of atovaquone, proguanil and cycloguanil in studies of currently recommended doses for malaria prophylaxis or treatment (range of mean or median values reported). Parameter Atovaquone Proguanil Cycloguanil Cmax (ng/mL) 634–13 270 560–751 37–67 Tmax (h) 5. The side-effects of atovaquone– proguanil are similar in children and adults (9, 14). The most common adverse effects reported are headache, cough and gastrointestinal disturbances (such as abdominal pain, nausea, vomiting and diarrhoea). Other adverse events occur rarely, such as dizziness and oral ulceration, and, very rarely, blood disorders including neutropenia and anaemia and skin reactions such as photosensitivity rash and erythema multiforme. Allergic reactions including anaphylaxis, angioedema, Stevens–Johnson syndrome and vasculitis may rarely occur. Pancytopenia in patients with severe renal impairment treated with proguanil has been reported, probably because of drug accumulation (15). Contraindications Atovaquone–proguanil is contraindicated in patients with known serious hypersensitivity reactions to atovaquone or proguanil. It is also contraindicated as malaria prophylaxis in patients with severe renal impairment because of the high risk for pancytopenia. The main concern is the approximate twofold reduction in plasma concentrations of both atovaquone and proguanil (7, 8), which could leave pregnant women more susceptible to malaria infection or at risk for treatment failure. Additional strategies are strongly advised for pregnant women taking atovaquone– proguanil for malaria prevention. Prolonged protection provided by a single dose of atovaquone–proguanil for the chemoprophylaxis of Plasmodium falciparum malaria in a human challenge model. The pharmacokinetics of atovaquone and proguanil in pregnant women with acute falciparum malaria. The pharmacokinetics and pharmacodynamics of atovaquone and proguanil for the treatment of uncomplicated falciparum malaria in third- trimester pregnant women. Sabchareon A, Attanath P, Phanuaksook P, Chanthavanich P, Poonpanich Y, Mookmanee D, et al. Effcacy and pharmacokinetics of atovaquone and proguanil in children with multidrug-resistant Plasmodium falciparum malaria. Lower atovaquone/proguanil concentrations in patients taking efavirenz, lopinavir/ritonavir or atazanavir/ritonavir. Chloroquine is extensively distributed in body tissues and fuids, including the placenta and breast milk. The drug is eliminated slowly from the body , with ~55% eliminated via the kidneys. Pharmacokinetic properties of chloroquine and desethylchloroquine in studies of currently recommended doses for malaria prophylaxis or treatment (range of mean or median values reported).

Nitroglycerin 6.5 mg on-line
To decrease lactic acidosis risk medicine zithromax nitroglycerin 6.5 mg buy, avoid in: Liver disease medicine vs medication cheap nitroglycerin 6.5 mg visa, alcohol abuse/bingeing If creatinine ≥1 medicine pouch nitroglycerin 6.5 mg online. On September 22, 2017 Provincial Council approved a policy direction for the administration of cannabis for medical purposes that required a change to content on page 30. The purpose of this document is to provide guidelines to address various components of safe and effective medication management in the practice setting. It requires nursing knowledge, skill and 1 Words or phrases in bold italics are listed in the Glossary. Safe and effective medication practices are a result of the efforts of many individuals and reliable systems (Institute for Safe Medication Practices, 2007b). Safe medication management includes the knowledge of medication safety, human factors that may impact medication safety, limitations of medication systems and best practices to reduce medication errors. Safe medication management requires: assessing the appropriateness of a medication for the client based on their health status or condition upholding the client’s rights in the medication process information on allergies and sensitivities performing medication reconciliation at client transitions of care knowledge of the actions, interactions, usual dose, route, side effects and adverse effects of the medication knowledge of correct drug dose calculations (drug dose calculators and drug libraries) and preparing the medication correctly appropriate documentation educating clients on the management of their own health including fully informing them about their medication, anticipated effects, side effects, contraindications, self-administration, treatment plan and follow-up monitoring the client before, during and following medication administration managing side effects or adverse effects of the drug evaluating the effect of the medication on the client’s health status The Seven Rights of Medication Administration Safe and competent medication practice requires using the seven rights of medication administration. Medication Reconciliation Communicating effectively about medication is a critical component of safe medication delivery (Accreditation Canada, the Canadian Institute of Health Information, the Canadian Patient Safety Institute, & the Institute for Safe Medication Practices Canada, 2012). Medication reconciliation is part of the High 5s Project launched by the World Health Organization to address major concerns about client safety around the world. Medication reconciliation is a formal process in which health-care providers work together with clients and families to ensure accurate and comprehensive medication information is communicated consistently across transitions of care. It enables authorized prescribers to make the most appropriate prescribing decisions for the client. Guideline 2: Nurses perform medication reconciliation in collaboration with the client/family and the health-care team. Further information on medication reconciliation can be found at the following websites: www. Ordering a Schedule 1 medication in Alberta is a restricted activity under the Government Organization Act (2000) and can only be performed by authorized prescribers. Many practice settings require an order or prescription for medication on any of the Schedules. A Schedule 1 medication is a medication that requires a prescription or order from an authorized prescriber. For information on medication schedules please see the Scheduled Drugs Regulation under the Pharmacy and Drug Act (2000) at http://www. Information on a prescriber’s authority is available from the prescriber’s regulatory college. Registered nurses, graduate nurses and certified graduate nurses are not authorized to prescribe Schedule 1 medications. They are unregulated workers who work under the supervision of a physician, and provide direct client care. Any medication order from a physician assistant must be authorized by the supervising physician before it is implemented by nurses. It is the responsibility of the physician assistant to ensure that the medication order is signed by the supervising physician in a timely manner. Guideline 4: Nurses only implement medication orders from a physician assistant that have been authorized by the supervising physician. Components of a Medication Order Medications should be prescribed as direct orders; that is, the medication is ordered for a specific client. A complete medication order includes: full name of the client the date name of the medication drug strength, if applicable dosage, if applicable route of administration frequency, and in some cases the length of time the drug is to be administered prescriber’s name, signature and designation reason/purpose (e. Verbal and Telephone Orders Verbal and telephone orders are more prone to error because of miscommunication when compared to orders that are written or communicated in a secure electronic health record system. The expectation is that authorized prescribers will provide a handwritten order or enter medication orders into a point of care electronic health record whenever possible. Situations where verbal or telephone orders would be considered acceptable include: emergent or urgent situations where delay in treatment would place a client at risk of serious harm; or when a prescriber is not present and direction is urgently required to provide appropriate client care In practice settings where authorized prescribers are not present (e. Guideline 5: Nurses only accept verbal and telephone orders in emergent or urgent situations where the authorized prescriber is unable or not present to document their medication orders directly. The authorized prescriber is accountable for authorizing or signing all of their verbal or telephone orders unless in an emergent or urgent situation where there is a designated recorder. The practice setting should have a policy that outlines the process for the use of verbal or telephone orders.
Buy generic nitroglycerin 6.5 mg online
Antiviral therapy was discontinued at birth to 3 nificantly lower in the treated group (22% vs treatment 5th disease purchase nitroglycerin 6.5 mg on-line. For pregnant women with immune-active hepati- tion in the Child-Pugh score and improved survival was tis B medications vitamins cheapest nitroglycerin, treatment should be based on recommenda- 113 tions for nonpregnant women symptoms 9f diabetes order nitroglycerin from india. In a study comparing compensated and virals are minimally excreted in breast milk and decompensated persons with cirrhosis treated with ente- are unlikely to cause significant toxicity. There are insufficient long-term safety data in sons with advanced decompensated cirrhosis may be at infants born to mothers who took antiviral agents 74 higher risk. C-section is not indicated owing to insufficient Future Research data to support benefit. As a result, drug labels recommend avoidance of breastfeeding when on these drugs. Several studies have investigated lamivudine occur at delivery, given that a combination of hepatitis 122-124 levels in breastfed infants. One study of 30 mother- B immunoglobulin and vaccination given within 12 infant pairs demonstrated that the lamivudine concentra- hours of birth has reduced the rate of perinatal transmis- tion in breastfed infants was only 3. Similar findings have ral drugs are pregnancy class C except for telbivudine been reported in studies looking at tenofovir and breast- (class B) and tenofovir (class B). In a small study of 5 women, the median amount of tenofovir ingested from breast milk was only 125 Evidence and Rationale 0. T heevidenceprofileissum m arizedinSupporting Rates of C-section, postpartum hemorrhage or creatine 119 127 Table 5. In 11 controlled studies (1,504 mother-infant kinase elevation were not increased with antiviral therapy. However, tenofovir is considered a ale for a strong recommendation against treatment in preg- preferred choice, owing to its antiviral potency, the available nant women at low risk of transmission is based on placing safety data of use during pregnancy, and concerns for resist- higher value on preventing unknown maternal and fetal ance with the other antiviral agents. In available stud- to prevent perinatal transmission, the exact viral load ies, antiviral therapy was started between weeks 28 and 32 threshold and the exact week within the third trimester of pregnancy. No studies have addressed the duration of at which to initiate therapy has not been fully estab- therapy (stopping at delivery vs. In addition, data on need to be monitored for flares if antiviral therapy is dis- longitudinal follow-up of infants exposed to antivirals continued during pregnancy or early after delivery. The optimal tored every 3 months for at least 1 year for recurrent duration of oral antivirals in children is uncertain. Hepatitis B virus in the United States: infection, expo- sure, and immunity rates in a nationally representative survey. Ann Given the lack of evidence of benefit in immune-tolerant Intern Med 2011;154:319-28. Global and regional mortality from 235 causes of death for 20 Future Research age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Well-conducted studies to assess benefit versus ment of persons with chronic hepatitis B virus infection. Long-term follow-up of treated children is Screening for hepatitis B virus infection in adolescents and adults: a needed to validate the use of intermediate biochemical and systematic review to update the U. Preventive Services Task Force virological outcomes for clinically important outcomes. Line- arized hepatitis B surface antigen and hepatitis B core-related antigen Acknowledgment: This Practice Guideline was in the natural history of chronic hepatitis B. Clin Microbiol Infect produced in collaboration with the Hepatitis B Sys- 2014;20:1173-1180. Updated definitions of healthy ranges for serum alanine amino- rate for nucleos(t)ide-naive patients with chronic hepatitis B. Tenofovir disoproxil fumarate versus adefovir dipivoxil for with Chronic Hepatitis B Infection. Lack of effect of antiviral therapy in nondividing hepatocyte cul- years after treatment with peginterferon alpha-2a. Side effects of long-term oral antiviral therapy for hepati- Hepat 2014;21:825-834. Entecavir treatment for chronic hepatitis B: adaptation is not notolerant phase of infection: histologic findings and outcome. Clin needed for the majority of naive patients with a partial virological response. Three-year efficacy and safety of tenofovir disoproxil fumarate patients in immune-tolerant phase.
Buy genuine nitroglycerin line
These recommendations are based upon the following dosages by body weight: rifammpicin 10mg/kg medicine quizlet buy 2.5 mg nitroglycerin free shipping; isoniazid 5mg/kg symptoms dizziness nausea nitroglycerin 6.5 mg generic; Pyrazinamide 25 mg/kg schedule 9 medications 6.5 mg nitroglycerin with mastercard; ethambutol 25 mg/kg, If Ethambutol is given for any reason for more than 8 weeks, the daily dose must be reduced to 15 mg/kg body weight. Women using contraceptive should be adviced to use pills with higher dose of oestrogen (50mcg) or change to another method 306 | P a g e 2. In case a patient develops jaundice, treatment should be stopped and restarted as soon as the jaundice resolves. If the patient improves follow with a gradual step up introduction of isoniazid followed by rifampicin until full dose. Streptomycin andEthambutol are excreted by the kidneys and should either be avoided or given in a reduced dose. Four different categories of drug resistance have been identified: Mono-resistance: Resistance to one anti-tuberculosis drug Poly-resistance: Resistance to more than one anti-tuberculosis drug, other than both isoniazid and Rifampicin (e. It is a disease mainly of human beings, which affects people of all races, all ages and both sexes. Patients harboring many bacilli in their bodies, the multi bacillary patients, are the main sources of infection. If not treated, they spread the disease in the community and infect others through coughing and sneezing (droplet infection). These infectious patients represent only about 25% of the registered leprosy patients in Tanzania. The other 75% of patients with few leprosy bacilli, the paucibacillary patients are less infectious. Skin contact with leprosy patients is no longer considered to be an important means of transmission. The different manifestation of leprosy is due to differences in the degree of resistance (immunity) of the human body and not due to different kinds of bacilli. About 75% of children who get infected with leprosy bacilli have such a high resistance that they overcome the disease themselves, without treatment, at very early stage. People who have a fairly high but incomplete immunity to leprosy bacilli will develop paucibacillary leprosy. Leprae, the bacilli may multiply freely and attain large numbers causing multi-bacillary leprosy. Diagnosis The major clinical features therefore include hypopigmented anaesthetic macula or nodular and erythematous skin lesions and nerve thickening. The following must be obtained: General information: all three names, sex, year of birth, full address form home to clinic, ioccupation Contact information: other leprosy cases in the patient’s household Main complaints, including date of onset, site of first lesions, subsequent changes and development received. Physical examination Physical examination should always be carried out with adequate light available and with enough privacy for the person to feel at ease. To ensure that no important sign is missed, a patient must be examined systematically. A well tried system is to examine the patient as follows: o Start with examination of the skin, first head, then neck, shoulders, arms, trunk, buttocks and legs o Then palpation of the nerves; starting with the head and gradually going to the feet o Then the examination of other organs o Examination of the skin smear o Finally the examination of eyes, hands and feet for disabilities. Complications due to nerve damage Patients should be examined for the following complications which result from nerve damage: Injury to cornea and loss of vision due to incomplete blink and/or eye closure Skin cracks and wounds on palms and soles with sensation loss Clawed fingers and toes Dropfoot Wrist drop Shortening and scarring gin fingers and toes with sensation loss. Mark and draw also wounds, clawing and absorption levels on the maps using the appropriate marks. Leprosy is classified into two groups depending on the number of bacilli present in the body. Classification is also important as it may indicate the degree of infectiouness and the possible problems of leprosy reactions and further complications. There are two methods of classifying leprosy, based on: The number of leprosy skin lesions The presence of bacilli in the skin smear Skin smear is recommended for all new doubtful leprosy suspects and relapse or return to control cases. This certainly applies to patients who have been treated in the past and of who insufficient information is available on the treatment previous used. Treatment of leprosy with only one drug monotherapy will result in development of drug- resistance, therefore it should be avoided. Patient having multibacillary leprosy are given a combination of Rifampicin, Dapsone and clofezimine while those having paucibacillary leprsosy are given a combination of Rifampicin and Dapsone.
Gnar, 41 years: The information may not be copied in whole Community Plan Director of Pharmacy Services by either or in part without the written permission of mail or fax.
Urkrass, 30 years: Among all patients, there were significantly fewer suicide attempts or other major dyscontrol episodes along with improve- ment in anxiety, anger, and euphoria (by a physician’s assessment only) with carbamazepine treatment compared with placebo.
Berek, 33 years: Testosterone supplemen- testosterone on brachial arterial vasoreactivity in men with tation does not worsen lower urinary tract symptoms.
Arokkh, 43 years: Natural history of liver fibrosis progression in patients with chronic hepatitis C.
Felipe, 31 years: An assessment of the patient’s medication-related needs This comprehensive assessment includes all of the patient’s medications (prescription, nonprescription, alternative, traditional, supplements, vitamins, samples, medications from friends and family, etc.
Ronar, 50 years: We only included data for outcomes reporting the average length of time to return to an activity if >80 % of the patients were included in the calculation.
Riordian, 46 years: Residents are advised, as appropriate, about the indication for prescribed medicines and are given access, to the patient information leaflet provided with medicines, accessible health information or pharmacist counseling service.
Keldron, 27 years: Treatment Persons with a penicillin allergy whose compliance with Because latent syphilis is not transmitted sexually, the therapy or follow-up cannot be ensured should be desensitized objective of treating persons in this stage of disease is to prevent and treated with benzathine penicillin.
Jorn, 34 years: Persons who are found to be not criminally responsible, or who are later diagnosed with severe mental disabilities and/or health conditions, for whom staying in prison would mean an exacerbation of their condition, shall not be detained in prisons, and arrangements shall be made to transfer them to mental health facilities as soon as possible.
Peer, 45 years: Companies can take steps to ensure that the public is aware of the risks associated with substance use, including the use of medications with addictive potential alone and in combination with alcohol or other drugs.
Yokian, 44 years: Measurable outcome parameters personalized With the service of the Medical for each patient so he or she can participate in the care plan in a patient-centered approach.
Pakwan, 40 years: Definition of key terms: Numerator: Number of deaths of children under five years during a specified period x 1,000.
Aila, 58 years: Bedaquiline ↑ Bedaquiline expected Co-administration should be avoided, if possible.
Mezir, 63 years: For example, further controlled treatment studies of psychodynamic psychothera- py, dialectical behavior therapy, and other forms of cognitive behavior therapy are needed, partic- ularly in outpatient settings.
Fraser, 35 years: The Power on which the prisoner of war depends shall be responsible for settling with him any credit balance due to him from the Detaining Power on the termination of his captivity.
Javier, 53 years: Hard waters have greater fouling Water Treatment Manual: Disinfection potential particularly from compounds for which solubility decreases with increasing temperature e.
9 of 10 - Review by A. Gorok
Votes: 38 votes
Total customer reviews: 38
References
- Takemura M, Niimi A, Minakuchi M, et al. Bronchial dilatation in asthma: relation to clinical and sputum indices. Chest 2004;125(4):1352-8.
- Banner LW. American Beauty. New York: Alfred Knopf, 1983: 45-65.
- Field Supplementation Trial in Pregnant women. An ICMR Task Force Study, New Delhi, ICMR, 1992.
- Carbonell AM, Harold KL, Mahmutovic AJ, et al: Local injection for the treatment of suture site pain after laparoscopic ventral hernia repair. Am Surg 69:688, 2003; discussion 691.
- Papiris SA, Maniati MA, Kalousis JV, Constantopoulos SH. Chronic eosinophilic pneumonia in rheumatoid arthritis. Monaldi Arch Chest Dis 1995;50(5):360-2.
- Yeung LL, Grewal S, Bullock A, et al: A comparison of chlorhexidine-alcohol versus povidone-iodine for eliminating skin flora before genitourinary prosthetic surgery: a randomized controlled trial, J Urol 189:136n140, 2013.