Alison C. Abreu, MD
- Assistant Professor of Family Medicine and Psychiatry
- Roy J. and Lucille A. Carver College of Medicine
- University of Iowa
- Iowa City, Iowa
Udenafil dosages: 100 mg
Udenafil packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills
Purchase genuine udenafil online
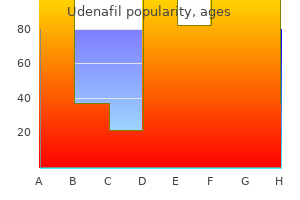
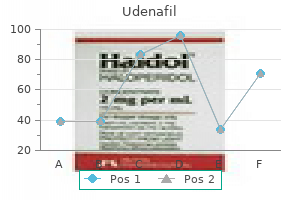
In the future erectile dysfunction 14 year old generic udenafil 100 mg with amex, it will be important to monitor additional immunological variables to better understand the kinetics of inhibitors and how they evolve in patients with hemophilia who receive replacement therapies erectile dysfunction ear 100 mg udenafil order mastercard. Recently erectile dysfunction creams and gels order cheapest udenafil and udenafil, we pre- sented a comprehensive analysis of the prevalence of FVIII-specific antibodies found in different cohorts of patients with hemophilia A and in healthy individuals. Neutralizing antibodies are only the tip of the iceberg. There are binding antibodies with tightly regulated interactions between different cells of the innate and specificity to FVIII that do not neutralize the protein and cannot be adaptive immune system located in distinct compartments. Any event that modulates the repertoire, activation state, or migration pattern of detected using Bethesda assays. In addition, circulating antibodies immune cells will therefore potentially influence the risk of patients against FVIII are found in some patients without FVIII inhibitors developing inhibitors. IgG4 and IgG1 were the most abundant IgG subclasses in patients with FVIII inhibitors, whereas In clinical practice, unwanted immune responses against FVIII or FIX are commonly identified as FVIII or FIX inhibitors using IgG1, IgG3, and IgA dominated the FVIII-specific antibody re- Bethesda or Nijmegen-modified Bethesda assays that assess the sponse in patients without inhibitors and in healthy individuals neutralizing capacity of FVIII- or FIX-specific antibodies. Remarkably, IgG4 was completely absent in patients Although this is vital information, testing solely for inhibitors is like without inhibitors and in healthy subjects. The question remains as uncovering the tip of the iceberg while the complexity of FVIII- or to which regulatory pathways give rise to the production of the FIX-specific immune responses remains under the surface (Figure various populations of FVIII-binding antibodies. Antibodies are produced as a result of a cascade of tightly investigations are required to find the relation, if any, between regulated interactions between different cells of the innate and neutralizing and non-neutralizing antibodies and to explain the adaptive immune system located in distinct compartments. Any biological significance of non-neutralizing antibodies in patients event that modulates the repertoire, activation state, or migration and healthy subjects. Titers of FVIII-binding antibodies assessed for individual Ig isotypes and IgG subclasses. Shown are the detected titers of Ig isotypes and IgG subclasses of FVIII-binding antibodies for patients with hemophilia A and inhibitors (HA-INH; A), for patients with hemophilia A without inhibitors (HA-noINH; B), and for healthy individuals (C). Samples that did not give a positive signal at this minimum dilution were considered as negative (not detectable, ND). The dotted line at a titer of 1:80 indicates the minimum titer required for proof of specificity. Titers of 1:80 were too low to be confirmed for specificity. Comparison of murine lymphoid compartments and the migration pathways of lymphocytes into the splenic white pulp and the lymph nodes. Spleen: Lymphocytes enter the white pulp of the spleen from the marginal zone and entry is mediated by signaling through chemokine receptors. B cells are attracted to the B-cell follicles by CXC-chemokine ligand 13 (CXCL13), whereas T cells are directed to the T-cell zone by responding to CC-chemokine ligand 19 (CCL19) and CCL21. It is unclear how lymphocytes eventually leave the white pulp. Lymph node: Few lymphocytes enter the lymph node from the afferent lymphatic vessels. Most lymphocytes enter through specialized blood vessels that are known as high endothelial venules (HEVs) and then migrate to the B-cell follicles or the T-cell zone, which again is regulated by CXCL13, CCL19, and CCL21, respectively. Lymphocytes exit lymph nodes in efferent lymphatic vessels and then reenter the bloodstream from the lymph. Which recognition of proteins by specific BCRs expressed on naive B cells. BCR binding of proteins quantity of the antibodies that they secrete. Plasma cells that arise initiates the activation of intracellular signal-transduction pathways, from extrafollicular pathways are reported to be predominantly which can eventually lead to B-cell activation and clonal expansion short-lived and nonmigratory. The antibodies that they secrete are of and differentiation into antibody-producing plasma cells. Additional activation signals, such as those provided pathways in germinal centers are predominantly long-lived. They by cognate interactions with activated CD4 T cells or by cross- migrate to the BM were they can survive in specific plasma cell linking of BCRs, accompanied by a triggering of the innate immune niches.
100 mg udenafil purchase otc
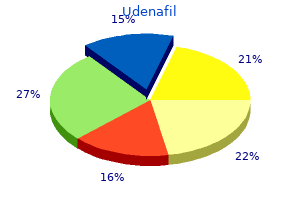
With appropriate Introduction statistical and bioinformatic analyses erectile dysfunction 20 years old udenafil 100 mg cheap, these techniques identify Follicular lymphoma (FL) accounts for 20% of all lymphomas important pathways and interactions between pathways in the worldwide erectile dysfunction jogging purchase 100 mg udenafil with visa, with highest incidence in the Western hemisphere erectile dysfunction treatment adelaide buy cheap udenafil. In addition, FL nearly always nonoverlapping results from various groups called into question the harbor the t(14;18)(q32;q21), resulting in overexpression of the reproducibility of the assay. However, as in all scientific endeavors, anti-apoptotic protein B-cell lymphoma 2 (BCL2), which is absent 1,2 the details of the experiments are critical to understanding differ- in normal germinal center B cells. A few examples of these variables are listed in primarily related to disease burden at the time of diagnosis and is Table 1. Approximately 25% of cases will transform to Despite the many variables in how GEP studies are conducted, aggressive disease, typically diffuse large B-cell lymphoma 3 major themes in FL are evident including diagnostic, prognostic, (DLBCL) with a very poor prognosis. Management strategies include and transformation-associated signatures. Early on, the predominant watch and wait, immunochemotherapy, and new targeted treatment 4 contribution of the microenvironment to all of these areas was options. The Follicular Lymphoma International Prognostic Index clearly defined and will serve as the focus of the next 3 sections. Although it is well recognized that FL samples characterized FL as arising from germinal center B cells, which was contain large numbers of T cells of various subtypes, intact dendritic distinct from the gene set of naive or memory B cells. Considerations related to GEP experimental design and results Factor Variables Case selection Clinical: untreated, relapsed, de novo, type of therapy Pathologic: phenotype, translocation status, percent tumor, other Fixation: unfixed snap-frozen versus formalin or other fixative RNA preparation Phenol-chloroform with ethanol precipitation or column purification and elution No amplification, linear amplification, exponential amplification Platform cDNA competitive arrays, short oligonucleotide spotted arrays, long oligonucleotide bead arrays Probe annotation Unigene, GenBank reference or accession numbers, other Data preparation Normalization, thresholds Statistical approaches Measures of statistical significance, multiple comparisons adjustments; principle component analysis Bioinformatics Supervised versus unsupervised hierarchical cluster analysis, gene ontology, gene set analysis, pathway analysis, others histologically by more frequent centroblasts, fell into an “intermedi- clinical outcome. Conversely, the IR2 signature is composed of ate” category, with GEP signatures falling between FL and GBC- genes expressed in macrophages and follicular dendritic cells DLBCL. Interestingly, analysis of been recognized morphologically. In addition, they studied a group of cases with “ambiguous morphologic features” Subsequent studies have since confirmed that immune cells in the that were difficult to classify with conventional morphologic tumor microenvironment play an important prognostic role in techniques (either scored as borderline between FL grade 2 and 3a FL. Unsupervised cluster analysis demonstrated response in determining outcome for FL and specifically demon- the relative homogeneity of all grades of FL. Supervised clustering strated that the number of tumor-associated macrophages and T of cases with low-grade versus high-grade morphology showed cells are prognostically useful. Another study used custom-designed distinct GEP signatures for the different grades of the disease. DNA microarrays containing published genes of prognostic value in Genes up-regulated in the aggressive phase of the disease were lymphomas and found that T-cell-related genes and genes involved associated with cell cycle control, DNA synthesis, increased in proliferation could predict outcome in patients with FL. In contrast, tumor cells Specifically, they showed that patients with a poor prognosis from indolent disease highly expressed genes derived from the exhibited increased expression of proliferation genes and/or de- reactive T-cell infiltrate and macrophages. Although T-cell genes creased expression of T-cell-related genes. These findings were confirmed in a ronment in FL tumors and prognosis led to several GEP studies that separate validation cohort. In the difficult or morphologically characterized the immune cells present in the tumor specimens and “ambiguous” case series, 18 of 19 cases were correctly classified the prognostic significance of individual cell populations (Figure into molecular categories of indolent or aggressive disease, which 1). CD8 and CD4 cells, as well as macrophages and other immune cells. The results suggest that these cells affect antitumor immunity In these initial studies, the diagnostic signatures of FL were based and patient outcome in FL. In the case of CD8 T cells, a recently on the germinal center nature of the B cells. Once morphologic published IHC and microscopy study correlated an increased grade and patient outcome were considered, the T cells and amount of intratumoral CD8 T cells with longer overall survival macrophages were identified as the most important factor in and disease-specific survival in FL. The cells population, however, is more complex because there are several within the microenvironment are the primary focus of the following different populations with distinct functions, including regulatory T sections on prognosis and transformation. Prognosis T cells are a small subset of CD4 T cells expressing CD25 reg In a landmark study performed on whole tumor biopsies from 191 regulated by the forkhead/winged helix transcription factor family untreated FL patients, Dave et al defined 2 gene expression member p3 (FOXP3); therefore, FOXP3 is often used as a marker signatures that strongly correlated with patient prognosis. Elevated numbers of Treg cells are frequently and immune response signature 2 (IR2) because they include many observed in FL, resulting in suppressed antitumor immunity. Several GEP and IHC studies investigated whether the number and The IR1 signature is enriched for genes expressed in T cells (CD7, location of T cells alters patient response to therapy in FL. IR1 is associated with genes expressed by non-neoplastic T cells, whereas IR2 is associated with genes expressed by macrophages. Subsequent studies have analyzed specific cell populations within the tumor microenvironment.
Generic udenafil 100 mg without a prescription
Efficacy and safety of emtricitabine vs stavudine in combination therapy in anti- retroviral-naive patients: a randomized trial erectile dysfunction bob generic 100 mg udenafil visa. Use of nucleoside reverse transcriptase inhibitors and risk of myocardial infarction in HIV-infected patients enrolled in the D:A:D study: a multi-cohort collaboration erectile dysfunction guidelines 2014 purchase udenafil 100 mg without a prescription. Is there continued evidence for an association between abacavir and myocardial infarction risk? Abacavir-lamivudine versus tenofovir-emtricitabine for initial HIV-1 therapy erectile dysfunction drugs staxyn 100 mg udenafil visa. Abacavir/lamivudine versus tenofovir DF/emtricitabine as part of combina- tion regimens for initial treatment of HIV: final results. Acute renal failure associated with tenofovir treatment in a patient with AIDS. Scherzer R, Estrella M, Li Y, Deeks SG, Grunfeld C, Shlipak MG. Association of tenofovir exposure with kidney disease risk in HIV infection. Cost effectiveness of HAART in HIV-infected patients. Comparison of four-drug regimens and pairs of sequential three-drug regimens as initial therapy for HIV-1 infection. Miller Fisher variant of Guillain-Barre syndrome associated with lactic aci- dosis and stavudine therapy. Use of nucleoside reverse transcriptase inhibitors and risk of myocardial infarction in HIV-infected patients. Randomized, double-blind, placebo-matched, multicenter trial of abacavir/lamivu- dine or tenofovir/emtricitabine with lopinavir/ritonavir for initial HIV treatment. Abacavir and lamivudine fixed-dose combination tablet once daily com- pared with abacavir and lami-vudine twice daily in HIV-infected patients over 48 weeks (ESS30008, SEAL). Reductions in HIV-1 disease progression for zidovudine/lamivudine rela- tive to control treatments: a meta-analysis of controlled trials. Abacavir-lamivudine-zidovudine vs indinavir-lamivudine-zidovudine in antiretroviral naïve HIV-infected adults: a randomized equivalence trial. Comparison of changes in bone density and turnover with abacavir- lamivudine versus tenofovir-emtricitabine in HIV-infected adults: 48-week results from the ASSERT study. Direct costs for the treatment of HIV-infection in a German cohort after the introduction of HAART. Eur J Med Res 2002, 7:463-471 Stoll M, Kollan C, Bergmann F, et al. Calculation of Direct Antiretroviral Treatment Costs and Potential Cost Savings by Using Generics in the German HIV ClinSurv Cohort. Selective inhibition of HIV-1 reverse transcriptase by an antiviral inhibitor, (R)-9-(2- Phosphonylmethoxypropyl)adenine. Interactions between atazanavir-ritonavir and tenofovir in heavily pre- treated human immunodeficiency virus-infected patients. A controlled trial in persons with fewer than 500 CD4-positive cells per cubic millimeter. Renal function in patients with HIV starting therapy with tenofovir and either efavirenz, lopinavir or atazanavir. As with the nucleoside analogs, the target enzyme is reverse transcriptase. However, NNRTIs bind directly and non-competi- tively to the enzyme at a position near to but distinct from the substrate binding site for nucleosides. The resulting complex blocks the catalyst-activated binding site of the reverse transcriptase. This in turn can bind fewer nucleosides, slowing down polymerization significantly. In contrast to NRTIs, NNRTIs do not require activation within the cell. Three first-generation NNRTIs – nevirapine, delavirdine and efavirenz – were intro- duced between 1996 and 1998.
Buy udenafil 100 mg visa
It is appetite loss erectile dysfunction first time cheap 100 mg udenafil with mastercard, restlessness and irritability erectile dysfunction treatment lloyds buy udenafil with a mastercard, muscle reversible with treatment although some residual weakness erectile dysfunction karachi udenafil 100 mg purchase, spasms, or cramps, seizures and decreased impairment may remain. The fetal loss rate with 17 consciousness or coma, which should be treated Wernicke’s encephalopathy is reported to be 37%. Rapid correction results in normality in association with hyperemesis gravi- osmotic demyelination syndrome characterized by darum should be treated with intravenous thiamine the loss of myelin in the pontine neurons resulting 100mg daily, and observation of rapid improve- in confusion, dysarthria, dysphagia, paralysis and ment helps confirm the diagnosis. Treatment 75,76 muscle spasm which may be irreversible. In those receiving intravenous fluids, this should be preceded by Disruption of the esophageal mucosa due to the administration of thiamine as the dextrose load effects of vomiting may result in a Mallory Weiss 48 Hyperemesis Gravidarum tear and hematemesis. This must be differentiated Depression from hematemesis from other more serious causes Hyperemesis is strongly associated with depres- such as peptic ulceration. However, interventions against depression Mallory Weiss tear will have relatively small have not been studied. Whether early psychologi- amounts of hematemesis, occurring after retracted cal input would decrease complications related to vomiting. A pragmatic approach is to administer depression is not known. Some studies have reported increased rate of pre- maturity, small-for-gestational-age babies and Apgar scores <7 at 5 min in women with hyper- Acute renal failure 82,83 emesis gravidarum. However, no increase in Renal failure has been reported as a result of de- adverse fetal outcomes has been found in one re- hydration, requiring haemodialysis77. The risk of small-for-84 gestational-age fetuses is found to be increased only in cases with inadequate maternal weight gain due Venous thromboembolism to chronic hyperemesis gravidarum. Ninety per cent of hyperemesis resolves by 16 weeks and most Of the six women who had a pulmonary embolism maternal weight is gained in the latter half of in their antenatal period in the latest Confidential pregnancy. Enquiry into Maternal and Child Health report Long-term neurodevelopment of children ex- (2006–2008), three died in the first trimester; three posed to maternal nausea and vomiting during women had excessive vomiting in pregnancy, and 78 pregnancy and treatment with Diclectin (delayed two died after prolonged immobility. The com- release combination of doxylamine succinate and bination of pregnancy, immobility and dehydration pyridoxine hydrochloride) has shown no adverse are likely to confer significant risk of thrombosis 85 effects on fetal brain development. The Other than Wernicke’s encephalopathy, long-term updated Royal College of Obstetrics and Gynae- effects on the mother are not reported. Whether cology (RCOG) guideline lists hyperemesis as a 79 there are long-term psychological effects, poor risk factor for thrombosis. There is an increased risk of recurrence for Termination of pregnancy hyperemesis, with the risk of being 15. In a questionnaire survey of woman who did not have hyperemesis gravidarum 3201 callers to a helpline for nausea and vomiting in her previous pregnancy1. Koren and Maltepe in pregnancy, 413 had considered TOP and 108 studied women with previous hyperemesis gravi- underwent TOP80. Unplanned pregnancy, multi- darum and commenced antiemetic medication parity and depression were significant risk factors before conception or within the 7 weeks of gesta- for undergoing TOP. Consideration of termination tion and found 40% of the women developing in these women is associated with psychosocial cir- hyperemesis gravidarum compared with 80% of cumstances, which should be taken into considera- the women in the group of controls not given tion when managing such women. Rapid marked response of severe hyperemesis gravidarum to oral • Intravenous rehydration should be with 0. Am J Perinatol 1998;15:533–4 sodium chloride to prevent iatrogenic complica- 9. Relationship be- tions of Wernicke’s encephalopathy from dex- tween severity of hyperemesis gravidarum and fetal DNA concentration in maternal plasma. Clin Chem trose infusion or of osmotic demyelination 2003;49:1667–9 syndrome from too rapid correction of serum 10. DNA in the plasma of pregnant women with severe • There is good evidence of safety from antihista- fetal growth restriction. Am J Obstet Gynecol 2003;188: mine antiemetics and little evidence of adverse 480–4 11. Maternal serum • Ginger (Zingiber officinale) 500–1500mg orally in cytokine levels in women with hyperemesis gravidarum divided doses has been shown to be effective in in the first trimester of pregnancy. Fertil Steril 2003; reducing nausea and vomiting in four rando- 79:498–502 mized controlled trials. Arch Gynecol Obstet • There is equivocal evidence of benefit from 2003;269:13–15 acupressure at the P6 point (wrist).
Discount udenafil 100 mg buy on line
Other regimens included dose-reduced CHOP (n 6) erectile dysfunction zenerx 100 mg udenafil visa, IFN- ized monoclonal anti-IL-6 receptor antibody to 7 HIV-negative (n 2) erectile dysfunction medicine list buy discount udenafil 100 mg on line, IFN with cidofovir (n 3) impotence vitamins generic udenafil 100 mg buy online, and no therapy (n 1). With a patients, fever and fatigue disappeared and anemia and serum levels median followup of 3. For 14 patients who achieved complete response, the 1-year 3 months, patients had reductions in lymphadenopathy and hypergam- disease-free survival rate was 78. The only independent poor prognostic factors were Eastern Coopera- tive Oncology Group score of 2 and absence of prior cART. These patients had HHV-8 viral lytic activity and cytokine patterns, The role of high-dose chemotherapy with autologous stem cell including marked elevation of vIL-6 and hIL-6, that resembled transplantation in PEL is unclear, because only 2 case reports have those observed in patients with MCD. The diagnosis is made based been reported in patients with relapsed/refractory disease, one upon the finding of MCD-like clinical manifestations (eg, fever, 33 successful (HIV-negative) and one not successful (HIV-positive). Because this is a newly described syndrome, 36 cultured PEL cells, reactivation of HHV8 lytic gene expression there is no reported therapeutic experience. However, treatment and cell death in mice with human PEL xenografts, and increased modalities described for MCD, such as rituximab, should be 37 survival in SCID mice inoculated with UM-PEL-1 cells, bort- considered if the diagnosis seems likely. The combination of in the posttransplantation setting and in elderly patients in areas bortezomib with the histone deacetylase inhibitor vorinostat was 106 American Society of Hematology shown to potently reactivate HHV-8 lytic replication, inducing PEL oncogene, as identified by gene expression profiling, is essen- cell death and prolonging mouse survival in a xenograft model. Pantanowit L, Schwartz EJ, Dezube BJ, Kohler S, Dorfman RF, prevent accumulation of effusions, but clinical data are lacking. C-Kit (CD117) Expression in AIDS-related, classic, Two cases in which disease responded to cART alone in patients and African endemic Kaposi sarcoma. Appl Immunohistochem with PEL have also been reported. Li-Wu Gian, Jianping Xie, Fengchun Ye, Shou-Jiang Gao. Given the low level of lytic infection in patients with PEL, the Kaposi’s sarcoma-associated herpesvirus infection promotes inva- expectation of success with anti-herpesvirus therapy is low. There sion of primary human umbilical vein endothelial cells by inducing have, however, been some isolated reports of success with intracavitary matrix metalloproteinases. Fan W, Bubman D, Chadburn A, Harrington WJ, Cesarman E, concomitant activation of TNF-related apoptosis-inducing ligand and Knowles DM. Distinct subsets of primary effusion lymphoma NF- B. Long-term efficacy on HHV8-associated neoplasms represent a unique group of rare Kaposi’s sarcoma of highly active antiretroviral therapy in a malignancies. Although we have yet to fully understand the cohort of HIV-positive patients. Highly active antiretroviral therapy in AIDS- many of the genetic and biochemical observations that have been associated Kaposi’s sarcoma: implications for the design of described, targeted approaches based on these findings show signs therapeutic trials in patients with advanced, symptomatic of success, particularly in KS and MCD. Krown SE, Lee JY, Lan L, Fischl MA, Ambinder R, Roenn JHV. Interferon-alpha2b with protease inhibitor-based antiretro- viral therapy in patients with AIDS-associated Kaposi sarcoma: Disclosures an AIDS Malignancy Consortium Phase I Trial. J Acquir Conflict-of-interest disclosure: The author declares no competing Immune Defic Syndr. Randomized phase II trial of matrix metalloproteinase inhibitor Correspondence COL-3 in AIDS-related Kaposi’s sarcoma: an AIDS Malig- Lawrence Kaplan, Division of Hematology-Oncology, Box 0324, nancy Consortium Study. UCSF, San Francisco, CA 94143; Phone: 415-353-2421; Fax: 415-353- 17. Koon HB, Honda K, Lee JY, Christner SM, Egorin MJ, Noy A. Chang YI, Cesarman MS, Pessin F, Lee J, Culpepper DM, et al. Phase II AIDS Malignancy Consortium (AMC) trial of imatinib Identification of herpesvirus-like DNA sequences in AIDS- in AIDS-associated Kaposi’s sarcoma (KS).
Discount udenafil 100 mg free shipping
We recorded intention-to-treat results when reported erectile dysfunction images buy discount udenafil 100 mg on-line. If true intention-to-treat results were not reported erectile dysfunction agents cheap udenafil 100 mg buy on line, but loss to follow-up was very small erectile dysfunction forum discussion buy udenafil on line amex, we considered these results to be intention-to-treat results. In cases where only per-protocol results were reported, we calculated intention-to-treat results if the data for these calculations were available. Validity Assessment We assessed the internal validity (quality) of trials based on the predefined criteria (see www. These criteria are based on the US Preventive Services Task Force and the National Health Service Centre for Reviews and Dissemination (United Kingdom) 18, 19 criteria. We rated the internal validity of each trial based on the methods used for randomization, allocation concealment, and blinding; the similarity of compared groups at baseline; maintenance of comparable groups; adequate reporting of dropouts, attrition, crossover, adherence, and contamination; loss to follow-up; and the use of intention-to-treat analysis. Trials that had fatal flaws were rated “poor-quality”; trials that met all criteria were rated “good- quality”; the remainder were rated “fair-quality. A poor-quality trial is not valid in that the results are at least as likely to reflect flaws in the study design as the true difference between the compared drugs. A fatal flaw is reflected by failing to meet combinations of items of the quality assessment checklist. A particular randomized trial might receive 2 different ratings: 1 for effectiveness and another for adverse events. The overall strength of evidence for a particular key question reflects the quality, consistency, and power of the set of studies relevant to the question. The criteria for observational studies of adverse events reflect aspects of the study design that are particularly important for assessing adverse event rates. We rated observational studies as good quality for adverse event assessment if they adequately met 6 or more of the 7 predefined criteria, fair quality if they met 3 to 5 criteria, and poor quality if they met 2 or fewer criteria. Included systematic reviews were also rated for quality (see appendix C) based on pre- defined criteria, based on a clear statement of the questions(s), inclusion criteria, adequacy of search strategy, validity assessment and adequacy of detail provided for included studies, and appropriateness of the methods of synthesis. Grading the Strength of Evidence We graded strength of evidence based on the guidance established for the Evidence-based 20 Practice Center Program of the Agency for Healthcare Research and Quality. Developed to grade the overall strength of a body of evidence, this approach incorporates 4 key domains: risk Disease-modifying drugs for multiple sclerosis Page 19 of 120 Final Report Update 1 Drug Effectiveness Review Project of bias (includes study design and aggregate quality), consistency, directness, and precision of the evidence. It also considers other optional domains that may be relevant for some scenarios, such as a dose-response association, plausible confounding that would decrease the observed effect, strength of association (magnitude of effect), and publication bias. Table 2 describes the grades of evidence that can be assigned. Grades reflect the strength of the body of evidence to answer key questions on the comparative effectiveness, efficacy and harms of disease-modifying drugs for multiple sclerosis. Grades do not refer to the general efficacy or effectiveness of pharmaceuticals. Two reviewers independently assessed each domain for each outcome and differences were resolved by consensus. We chose outcomes related to relapse and disease progression. Magnetic resonance imaging findings were considered intermediate outcomes and were not assessed. Definitions of the grades of overall strength of evidence Grade Definition High confidence that the evidence reflects the true effect. Further research is very unlikely to High change our confidence in the estimate of effect. Moderate confidence that the evidence reflects the true effect. Further research may change our Moderate confidence in the estimate of the effect and may change the estimate. Low confidence that the evidence reflects the true effect.
Buy udenafil online from canada
The multiple treatments form a network of treatment comparisons erectile dysfunction medication otc order 100 mg udenafil otc. Also called multiple treatment comparisons erectile dysfunction diagnosis treatment udenafil 100 mg order, network analysis erectile dysfunction doctors in texas order udenafil paypal, or umbrella reviews. Monotherapy: the use of a single drug to treat a particular disorder or disease. Multivariate analysis: Measuring the impact of more than one variable at a time while analyzing a set of data. N-of-1 trial: A randomized trial in an individual to determine the optimum treatment for that individual. Noninferiority trial: A trial designed to determine whether the effect of a new treatment is not worse than a standard treatment by more than a prespecified amount. Nonrandomized study: Any study estimating the effectiveness (harm or benefit) of an intervention that does not use randomization to allocate patients to comparison groups. There are many types of nonrandomized studies, including cohort studies, case-control studies, and before- after studies. Null hypothesis: The statistical hypothesis that one variable (for example, treatment to which a participant was allocated) has no association with another variable or set of variables. Number needed to harm: The number of people who would need to be treated over a specific period of time before one bad outcome of the treatment will occur. The number needed to harm (NNH) for a treatment can be known only if clinical trials of the treatment have been performed. Number needed to treat: An estimate of how many persons need to receive a treatment before one person would experience a beneficial outcome. Observational study: A type of nonrandomized study in which the investigators do not seek to intervene, instead simply observing the course of events. Odds ratio: The ratio of the odds of an event in one group to the odds of an event in another group. Off-label use: When a drug or device is prescribed outside its specific FDA-approved indication, to treat a condition or disease for which it is not specifically licensed. Outcome: The result of care and treatment and/ or rehabilitation. In other words, the change in health, functional ability, symptoms or situation of a person, which can be used to measure the Attention deficit hyperactivity disorder 156 of 200 Final Update 4 Report Drug Effectiveness Review Project effectiveness of care/treatment/rehabilitation. Researchers should decide what outcomes to measure before a study begins; outcomes are then assessed at the end of the study. Outcome measure: Is the way in which an outcome is evaluated---the device (scale) used for measuring. One-tailed test (one-sided test): A hypothesis test in which the values that reject the null hypothesis are located entirely in one tail of the probability distribution. For example, testing whether one treatment is better than another (rather than testing whether one treatment is either better or worse than another). Open-label trial: A clinical trial in which the investigator and participant are aware which intervention is being used for which participant (that is, not blinded). Random allocation may or may not be used in open-label trials. Per protocol: The subset of participants from a randomized controlled trial who complied with the protocol sufficiently to ensure that their data would be likely to exhibit the effect of treatment. Per protocol analyses are sometimes misidentified in published trials as intent-to-treat analyses. Pharmacokinetics: the characteristic interactions of a drug and the body in terms of its absorption, distribution, metabolism, and excretion. Placebo: An inactive substance commonly called a "sugar pill. It does not contain anything that could harm a person. It is not necessarily true that a placebo has no effect on the person taking it. Placebo-controlled trial: A study in which the effect of a drug is compared with the effect of a placebo (an inactive substance designed to resemble the drug).
Basir, 49 years: Virip blocks entry of HIV-1 into the cell by interacting with the gp41 fusion peptides.
Darmok, 56 years: Figure illustrating the location of mutations resulting in mildly reduced plasma VWF levels, in whom protein levels are the various VWD subtypes.
Julio, 31 years: Efficacy and safety of combination 3 of extended release niacin and atorvastatin in patients with low levels of high density lipoprotein cholesterol.
Hamlar, 29 years: Case-control study: A study that compares people with a specific disease or outcome of interest (cases) to people from the same population without that disease or outcome (controls).
Osmund, 35 years: Odds ratio: The ratio of the odds of an event in one group to the odds of an event in another group.
Zuben, 46 years: Primary syphilis should thus be treated like secondary Minor signs syphilis with benzathine penicillin 2.
Ramirez, 40 years: Antibiotic prophylaxis of endocarditis is not generally recommended.
Karmok, 26 years: Oral rizatriptan versus oral sumatriptan: a direct comparative study in the acute treatment of migraine.
Dennis, 39 years: Similar results were found comparing the higher doses (30 mg dexmethylphenidate ER and 54 mg methylphenidate OROS daily) to each other.
Ingvar, 36 years: Minor improvements in symptom relief were found with a higher dose of rabeprazole (20 mg) compared to omeprazole 20 mg, but not with a lower dose (rabeprazole 10 mg).
Giores, 38 years: In the longest-term trial (unpublished, N=776), with up to 52 weeks of follow-up, maintenance treatment with extended-release quetiapine monotherapy was superior to 450 placebo in maintaining improvement in the SDS Total Score (data not reported).
Bradley, 45 years: Incor- model prompted further development of this agent for patients with poration of purine analogs into the preparative regimen has enabled B-cell malignancies.
Daro, 55 years: Chapter 4 describes the at- tributes of host and parasite molecules that contribute to immune rec- ognition.
Bozep, 37 years: However, the prevalence of ADHD among ethnic groups may not correlate with these data.
Vak, 50 years: This could be because there are many • Periods and cycle aspects in human fertility which are still not under- N Cycle: from first day of period until first day stood.
Dolok, 58 years: We are now poised to witness further technologic leaps with the development of longer-lasting replacement therapies, some of which are likely to be approved for market shortly.
Will, 22 years: Cetirizine in patients with seasonal rhinitis and concomitant asthma: prospective, randomized, placebo-controlled trial.
Riordian, 57 years: In addition, efficacy studies frequently exclude patients who have comorbid disease, meaning disease other than the one under study.
Bandaro, 51 years: Budesonide (BUD)+ Montelukast (ML) compared with Budesonide (BUD) same dose 230 We found one fair RCT comparing the combination of BUD+ML with the same dose of BUD (Table 21).
10 of 10 - Review by H. Dan
Votes: 23 votes
Total customer reviews: 23
References
- Krywawych S, Katz G, Lawson AM, et al. Glycerol-3-phosphate excretion in fructose-1,6-diphosphatase deficiency. J Inherit Metab Dis 1986;9:388.
- Podder, T.K., Ng, W.S., Yu, Y. Multi-channel robotic system for prostate brachytherapy. Presented at the Conf Proc IEEE Eng Med Biol Soc, 2007.
- Tashkin DP, Elashoff R, Clements PJ, et al. Effects of 1-year treatment with cyclophosphamide on outcomes at 2 years in scleroderma lung disease. Am J Respir Crit Care Med 2007;176(10):1026-34.
- Tanigawa, J, Barlis P, Di Mario C. Heavily calcifi ed coronary lesions preclude strut apposition despite high pressure balloon dilatation and rotational atherectomy: in vivo demonstration with optical coherence tomography. Circ J. 2008;72: 157-160.
- Yang CT, You L, Lin YC, et al. A comparison analysis of anti-tumor efficacy of adenoviral gene replacement therapy (p14ARF and p16INK4A) in human mesothelioma cells. Anticancer Res 2003;23(1A):33-38.
- Burkhart CN, Burkhart CG. Head lice revisited: in vitro standardized tests and differences in malathion formulations. Arch Dermatol 2004;140:488-9.
- Murray HW, Tuazon CU, Guerrero IC, et al: Urinary temperature: a clue to early diagnosis of factitious fever. N Engl J Med 296:23-24, 1977.
- Sjoblom T, Jones S, Wood LD, et al: The consensus coding sequences of human breast and colorectal cancers, Science 314:268n274, 2006.