Eric J. Topol, MD
- Professor of Genetics
- Department of Genetics
- Case Western Reserve University
- Cleveland, Ohio
Sominex dosages: 25 mg
Sominex packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Cheap sominex 25 mg
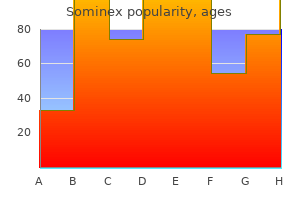
In certain cases where there are little or no other associated abnormalities insomnia yahoo sominex 25 mg buy on-line, higher levels of activity may be encouraged sleep aid zantac purchase genuine sominex on line. This decision should be based on preparticipation evaluations and exercise testing sleep aid diphenhydramine 25 mg sominex purchase with mastercard. Also, as with leisure activities, exceptions may be indicated in the rare patient with no significant associated abnormalities and normal ventricular and atrioventricular valve function. Frequent assessment of such patients is needed to assure safe participation in more vigorous activities. Single Ventricle Physiology Although patients with Fontan physiology have improved exercise tolerance compared to unoperated patients with single ventricles, their aerobic performance remains, in most cases, well below that of their age-matched peers and is also lower than that of most patients with other types of congenital heart defects. Diminished muscle bulk and function may also contribute to reduced exercise tolerance (167). Submaximal aerobic capacity appears to be somewhat better preserved in this population. This finding may reflect the limited ability of this physiology to maintain ventricular preload at higher heart rates (165). Energy loss through the Fontan circuitry due to turbulence may limit the ability to augment cardiac output with exercise (168,169). Heart block and the loss of sequential atrioventricular conduction and sinus node dysfunction may also affect performance. There are increasing data showing that aerobic capacity and exercise tolerance declines in this population as they progress through their second and third decade of life. A significant decline in aerobic performance has been associated with onset of symptomatic heart failure and cardiac death or need for heart transplantation (27). Evaluation Prior to Exercise and Sports Participation Prior to undertaking a regular physical activity or conditioning program, patients with stable Fontan physiology should have a thorough baseline evaluation. A graded exercise test is extremely useful to measure aerobic and physical working capacities. Evaluating pulmonary function at rest and exercise may be quite useful in unmasking associated pulmonary abnormalities that may impact on exercise performance. Leisure Activities and Activities of Daily Living Patients with stable Fontan physiology are typically able to engage in normal daily activities without impairment. Although exercise performance is quite limited in this group of patients, the variation in performance is great. On formal exercise testing, up to 25% to 30% of patients with Fontan physiology will have aerobic capacities within the range of normal for healthy age-matched peers. These patients can and often do keep up with their peers with all levels of recreational activity. At the other extreme is a significant portion of patients with Fontan physiology who have quite limited exercise performance. Patients should be allowed to rest when fatigued, maintain adequate hydration, and avoid bodily collision if taking antithrombotic medication. Principle for Recreational Activities a and Exercise Training in Children and Adolescents with Fontan Procedure F. Ordinary physical activity I does not cause undue dyspnea or fatigue, chest pain, or near syncope. Less than ordinary daily activities result in excessive dyspnea, fatigue, chest pain, or near syncope. Competitive Sports The issue of participation in competitive sports in this population is complex. For reasons stated above, most adolescents and young adults with Fontan physiology are unlikely to be able to successfully compete in sports with moderate or greater dynamic and static requirements (Fig. Therefore, the recommendations of the Bethesda Conference restricting them from those activities are a reasonable default position (82). Because there are exceptional patients in this age range with normal exercise capacity, a case-by-case evaluation should be made for these patients who may wish to compete at higher levels of intensity. The risks should be carefully evaluated and discussed with the patient and family. As previously mentioned, preadolescent patients with Fontan physiology may often have normal or near normal exercise capacity. Also, as discussed earlier in this chapter, the nature of competitive sports in this population is significantly different from that of adolescent and adult level sports.
Order generic sominex online
Careful quality control can help to avoid incidences of inaccurate or imprecise data collection sleep aid gels purchase cheap sominex, missing data sleep aid sominex 25 mg buy free shipping, or data falsification insomnia zippyshare 25 mg sominex buy with visa, all of which are likely to introduce error in the study results and undermine the strength of any conclusions drawn. The larger a clinical trial, the greater the importance of quality control—increasing numbers of investigators and primary sites of data collection P. Standardization measures are often implemented before the start of a study, and function to minimize variation in and absence of data through the systematization of study methods and practices. Study aspects often standardized include measurement procedures, working laboratory and clinical definitions, and data collection, storage, and analysis protocols. The most fundamental tool available for the standardization of a clinical trial is the operations manual, essentially an expanded protocol precisely detailing important methods to be used in implementing the study (see Table 81. The operations manual is meant to be readily available to all study personnel for the entire duration of the study, and consulted when any protocol uncertainties arise. Training and certifying all study personnel in proficiency for all study procedures is also a useful means of implementing standardization. Training and certification helps to reduce the inter- and intraobserver variability in any study measurements, as well as ensure clear understanding of all study protocols and definitions for all study personnel. Regular performance reviews of study personnel and whole trial centers help to maintain standardization measures throughout the duration of the trial, by auditing data collection and evaluating adherence to protocol as outlined in the operations manual. Such reviews are especially important in longer-term trials, where it may be difficult to maintain the rigor of standardization methods long after the study has begun. Adjudication is an especially important quality control measure where considerable variability may exist between investigators with respect to the ascertainment and reporting of events (Table 81. Particularly with outcomes requiring a complex and/or subjective judgment, adjudication plays a key role in confirming the reproducibility and reliability of any study findings. Quality control by repeated adjudication involves the replication of a given outcome measurement or diagnosis by multiple observers, and comparison of the individual results to assess the interobserver reliability. The implications of repeated adjudication vary depending on the type of outcome being ascertained. For nonnumerical outcomes, such as attribution of cause of death, comparison of multiple judgments helps assess the interobserver reliability of the measure and the most likely correct outcome. A high degree of disagreement between observers may indicate a high level of error and/or bias in the adjudication process, and requires that the outcome be subject to further assessment before a final decision is made. In the adjudication of a numerical outcome, multiple measurements can be averaged to reduce the variation in the reading. Allows all adjudication to be laboratory performed by a handful of individuals under highly standardized conditions. Staffed by a small number of highly trained, fully blinded Drastically reduces intra- and technicians. Receives collected data from separate trial center(s), is responsible for final adjudication and analysis of all outcomes. Responsible for verifying outcomes adjudicated and reported by Ensures final outcome results individual trial centers, by ensuring each decision meets a are unaffected by variability in specific set of protocol-specified criteria. May also fill other roles in quality control, such as organizing and monitoring adjudication procedures, undertaking performance reviews, and coordinating training and certification of study center staff. Central adjudication committees or core labs are a robust method of quality control in the adjudication process. A core lab is a centralized data collection and interpretation system, which acts to ensure that standardization is strictly maintained throughout the processes of outcome adjudication, reporting, and analysis. Core labs may take one of two forms in clinical trials: that of a physical laboratory site centralizing all laboratory-dependent data analysis, or that of an auxiliary review center charged with verifying outcomes adjudicated and reported by individual trial centers (Table 81. Although more costly, time and labor-intensive than repeated adjudication, core labs are a preferred method of standardization in clinical trials, especially those involving multiple separate study centers. Detection of missing data from final Performance of preliminary analyses, for: database i. Prevention of falsification of data stopping of the trial Data and Safety Monitoring Data monitoring describes the process of screening and analyzing data as they accumulate over the course of a trial.
Diseases
- Sirenomelia
- Odontoma
- Wolcott Rallison syndrome
- Deletion 6q16 q21
- 11 beta hydroxylase deficiency
- Agyria-pachygyria type 1
- Davis Lafer syndrome
- Ganglioglioma
Buy sominex 25 mg with amex
Recurrent left-sided heart leiomyosarcoma: should heart transplantation be legitimate? Heart transplantation for cardiac angiosarcoma: should its indication be questioned? Primary cardiac tumors in infants and children: Immediate and long-term operative results sleep aid nature made cheapest sominex. Human cardiac explantation and autotransplantation: application in a patient with a large cardiac pheochromocytoma quinine sleep aid discount 25 mg sominex amex. Two-dimensional echocardiographic findings in a case of massive cardiac involvement by malignant lymphoma insomnia vitamin d cost of sominex. Shaddy Introduction Chronic heart failure is a clinical syndrome with diverse etiologies and broad variation in its clinical manifestations, all of which ultimately result from impaired ventricular filling or ejection of blood (1). Traditionally, chronic heart failure has been viewed as a syndrome of inadequate cardiac output to maintain end-organ perfusion during rest or exercise, and has historically been equated with reduced left ventricular ejection fraction. In this chapter, the various causes of chronic heart failure in children will be described, along with their management and prognosis. Acute heart failure syndromes in the child, fetus, and adolescent, including myocarditis, as well as mechanical circulatory support and heart transplantation, will be discussed in further detail elsewhere within this textbook. The topic of chronic heart failure in adults is of great significance for public health given its substantial incidence and burden on healthcare costs and utilization in developed countries, and is only expected to increase in coming years (4). While the comparative impact of pediatric chronic heart failure is much more limited relative to that of the adult syndrome, it is a resource-intensive disease (5,6) with higher rates of hospital-related mortality compared to adults, in addition to having high rates of hospital-associated morbidity (7). The treatment of chronic heart failure has recently been subject to comprehensive evidence-based review and recommendations by professional societies for both adults and children (1,8,9,10,11). Nomenclature and Classification The term “heart failure” is used in several contexts throughout the medical literature as well as common usage, and can hence be confusing to the novice practitioner. In infants and young children, objective assessment of activity limitation can be difficult, so surrogate measures such as growth failure may be used in this patient population. However, “heart failure” may also be used to describe a constellation of acute signs and symptoms seen in conjunction with systemic ventricular dysfunction: left atrial hypertension, pulmonary edema, hepatomegaly, tachycardia, and gallop rhythm, without consideration given to assessment of cardiac output or ventricular function. Adding another layer of ambiguity to the definition of heart failure is the frequent application of this term to infants with large left-to-right intracardiac shunt lesions, who will often manifest the aforementioned symptom complex but have no evidence of systemic ventricular dysfunction; their symptoms merely resemble that of patients with systemic ventricular dysfunction due the common symptoms of left atrial hypertension, pulmonary vascular congestion, and systemic vascular congestion (hepatomegaly and peripheral edema). Several classification schemes have been proposed to define the clinical severity of chronic heart failure in children and adults, similar to the staging criteria utilized for various malignancies. Etiology An approach to understanding chronic heart failure in children begins with an investigation of the cause (Table 73. For the purposes of this chapter, “structural heart disease” encompasses primary anatomic cardiac abnormalities such as congenital heart disease, valvar stenosis and/or regurgitation independent of a congenital abnormality, and coronary artery disease. This is in distinction to cardiomyopathies and pericardial disease, which primarily affect cardiac muscle and the pericardium, respectively. Broadly speaking, from the standpoint of age, children can be divided into two broad groups: neonates/infants (<1 year of age) and children/adolescents; the etiologies of chronic heart failure in these populations tend to be distinct, although overlap certainly exists. Neonates and Infants The neonate or infant with heart failure typically presents for care after an episode of acute illness in which the diagnosis of heart failure is made, hemodynamic instability and symptoms are stabilized, and medical management is initiated. In some instances, the diagnosis is clear, although in a substantial proportion of cases, the diagnosis remains unclear and the child is left with the diagnosis of “idiopathic dilated cardiomyopathy. The Ross classification for heart failure in children after 25 years: a review and an age-stratified revision. Broadly speaking, potential etiologies of chronic heart failure in neonates and infants can be grouped under infectious, inflammatory, toxic, structural/congenital, metabolic, arrhythmogenic, and idiopathic. The differential diagnosis for the unusual presentation of heart failure at the time of birth includes birth asphyxia with myocardial dysfunction from hypoxemia, hypoglycemia, hypocalcemia, sepsis, anemia or polycythemia, myocarditis, arrhythmias (congenital complete heart block, supraventricular tachyarrhythmias), large arteriovenous malformations, severe atrioventricular valve regurgitation, or Ebstein abnormality of the tricuspid valve (13). Essentially any form of congenital heart disease can precipitate ventricular dysfunction, although ventricular dysfunction with resultant symptoms of low cardiac output are generally restricted to the following physiologic derangements: (a) obstructive lesions (i. Much of what is termed “critical” congenital heart disease consists of defects within the obstructive lesion group, in which severe hypoplasia or atresia of left heart structures and/or the aorta leads to inadequacy of cardiac output upon closure of the ductus arteriosus.
Sominex 25 mg amex
The examiner should sit and carefully listen to the details provided by the patient and parents insomnia 57 buy 25 mg sominex with visa. Therefore insomnia you suck buy discount sominex on line, historical information should be elicited from the patient insomnia lounge 25 mg sominex sale, as age and maturity allow, and from the parents as observers. In that way, an honest and positive patient–physician relationship will be established. Newborns and Infants Congenital heart disease often presents in early infancy because of observed abnormalities in the appearance or behavior of the infant. If the mother has had previous children, she may offer insight into differences in feeding habits between the patient and her other children. Frequency of feeding, volume of milk or formula (and type of formula, especially regarding kcal/oz information) consumed, and the length of time to finish a feeding should be obtained for both bottle- and breastfed infants. It is common for children with congestive heart failure to take breaks during a feeding because of rapid breathing or to fall asleep during feeding only to awaken after a few minutes and feed a small amount again. Generally, normal infants should be able to complete their feeding in <30 minutes. A longer time to finish each feeding, low volume consumed, excessive diaphoresis, and increased work of breathing during feeding are signs of heart failure or poor cardiac output. As pulmonary vascular resistance declines over the first 4 to 6 weeks of life, irritability and fussiness with feeding may indicate angina and ischemia in a child with an anomalous left coronary artery from the pulmonary artery. Central cyanosis, which reflects true arterial desaturation, is characterized by blueness of the tongue and oral mucosa. Children in shock also may appear cyanotic owing to venous stasis, right-to-left intrapulmonary shunting, or increased peripheral oxygen extraction. Acrocyanosis, or blueness of the hands and feet related to skin temperature, is normal. Similarly, blueness of the skin around the mouth or other parts of the face can often be attributed to alterations in skin blood flow or vasomotor instability, and should be considered to be a normal variant. Cyanosis may be more difficult to recognize in the anemic patient, because with decreased hemoglobin, similar levels of desaturation may not produce sufficient quantities of reduced hemoglobin (>5 g/%) to be clinically apparent. If there has been observed cyanosis, it is important to distinguish between constant cyanosis and episodic cyanosis. Constant cyanosis should suggest the presence of congenital heart disease with hypoxemia related to transposition physiology, inadequate pulmonary blood flow, or intracardiac mixing. Episodic cyanosis may be due to hypoxemia related to hypercyanotic episodes from tetralogy of Fallot physiology (see Chapter 41). This can occur in tetralogy of Fallot, in some patients with double-outlet right ventricle, or in patients who have subpulmonic stenosis associated with a univentricular circulation. Differential cyanosis of the upper and lower body in a newborn, although much less common, can also be an important finding. Lower body cyanosis with a pink upper body suggests right-to-left shunting at the level of the ductus arteriosus, seen in patients with persistent pulmonary hypertension of the newborn. Upper body cyanosis with pink lower extremities may indicate transposition of the great arteries with an aortic arch obstruction. In this circumstance, the lower body is perfused by the ductus arteriosus carrying pulmonary venous blood via the left ventricle to the pulmonary artery then to the descending aorta. Unlabored (“happy”) tachypnea often accompanies cyanotic heart disease, whereas increased work of breathing and sometimes grunting are associated with left-sided P. Grunting with closure of the glottis provides positive end-expiratory pressure and is seen in infants who have pulmonary edema. Parents may also observe intercostal or subcostal retractions when the child is undressed. If the infant has been symptomatic from birth, some first-time parents may not recognize mild respiratory symptoms such as tachypnea. Diaphoresis in this circumstance generally indicates activation of the sympathetic nervous system in patients who have low cardiac output. The time at which signs and symptoms of heart disease begin may be a clue to the type of cardiac lesion.
Order generic sominex line
The accident has caused the oil tanker to release 42 million liters of oil into the Prince William Sound insomnia video game culture purchase cheapest sominex and sominex, which harbors several diferent types of animals and aquatic life (Andres insomnia prevalence buy discount sominex 25 mg online, 1997) numark sleep aid 50mg sominex 25 mg order visa. Second, the Exxon corporation should be ordered immediately to survey the ship and con- tain the oil that has not already leaked out of it. State wildlife employees should be deployed to the disaster area immediately to protect the indigenous wildlife as much as possible. For those animals or birds that have already been covered in oil, wildlife ofcials will need to clean the animals as well as possible. Contact veterinarians and request that they volunteer to assist the wildlife afected by the oil spill. Other state and fed- eral ofcials should be contacted to obtain resources to contain the oil spill as much as possible. Stage 2 of the Disaster The oil is spreading over an 8-mile area around the oil tanker and 1,300 miles of your coastline is now contaminated, and a large amount of wildlife is covered by the oil. The only action that can be taken is to repair the rupture in the ship to prevent more oil from leaking and to try to evacuate wildlife from the afected area. An appeal to volunteers and nonproft groups for help may bring some assistance in the cleanup of the area and the wildlife that is covered in oil. The situation needs to be closely moni- tored to see where the oil slick may be expanding to along the coastline. Federal, state, and local ofcials need to be kept informed on the extent of the disaster, resources that are currently needed, and the progress of the diferent eforts to contain the oil leakage. Key Issues Raised from the Case Study Unfortunately, there is very little that local administrators can do in a situation where it appears that industry standards for safety were less than ideal. However, administrators can mitigate foreseeable ecological disasters by working closely with government agencies that have jurisdiction over shipping and conduct spot checks on the sobriety of the crew on ships that are carrying potentially dangerous cargo. Administrators can also restrict vessels with hazardous materials from traveling near wildlife refuges and inhabited areas. Case Studies: Man-Made Disasters—Industrial Accidents ◾ 135 The resources that administrators called for to contend with the crisis were ulti- mately insufcient for the disaster that was occurring. Additionally, the oil spill caused substantial damage to the environ- ment, which in turn negatively impacted commercial fshing, recreational usage, and tourism (Schure, 2010). Hyatt Regency Walkway Collapse, Kansas City, 1981 Stage 1 of the Disaster You are the director of code enforcement for a major metropolitan city. You have been under pressure lately since a structure, the roof of the Kemper Arena, has col- lapsed. The frst plan of action should be to review what processes were in place in regard to code enforcement that would allow a structure to be approved that was not designed properly. The other major issue would be to review the personnel involved that were instrumental in approving the roof of the Kemper Arena and review the training and the credentials of the inspectors that were involved in that particular project. Last, a departmental review should be undertaken to ensure that all per- sonnel have the correct credentials and training in the code enforcement department. An external audit should be undertaken of all code enforcement policies and per- sonnel to ensure that the department can comply with municipal mandates that are necessary for the municipality. A review should be undertaken to ensure that the department is correctly funded for the amount of workload that is placed on the department. If there are too many projects and not enough personnel, there is a potential danger for projects to be approved that would not ordinarily be approved. You should communicate with your depart- ment to take a stricter approach on reviewing construction projects and com- municate to contractors and architects working on projects in your city that code enforcement will be stepped up and projects that do not pass rigor will not be allowed to proceed. Your plan of action should be to undertake an external audit immediately as well as interview the employees that worked on the project. Since it may be a construction issue instead of a design faw, you need to fnd out all the information you can before taking any further action. Depending on the fndings of the investigation, you may need more inspec- tors for your department or more highly skilled inspectors working in the code enforcement department. In addition, there may need to be policy or procedures put in place to prevent this type of accident from occurring in the future. It is important to keep your assistant city manager and city manager informed of all of your fndings in regard to the accident and your department’s involvement with the company that built the hotel. Stage 3 of the Disaster The accident, caused by a structural failure, has killed 114 people and injured 200 others. Four days after the accident the local media discovers that there was a design change in the walkways during the construction of the hotel.
Syndromes
- Jaundice of pregnancy (bile may build up in the gallbladder because of pressure in the abdomen during pregnancy)
- Nervousness
- Pneumonia
- Receive blood transfusions (not common in the United States)
- Urine bilirubin
- Blood clot (thrombosis) in the blood vessels of the spleen
- Pressure or cramping in the lower abdomen (usually middle) or back
Buy sominex online pills
The atrioventricular conduction system in persistent common atrioventricular canal defect: correlations with electrocardiogram quinine sleep aid buy generic sominex 25 mg. Atrioventricular septal defect with balanced ventricles and malaligned atrial septum: double-outlet right atrium sleep aid by nature made order sominex 25 mg on-line. Successful correction of double outlet left atrium associated with complete atrioventricular canal and l-loop double outlet right ventricle with stenosis of the pulmonary artery insomnia zippyshare 25 mg sominex with mastercard. Anatomic observations on complete form of persistent common atrioventricular canal with special reference to atrioventricular valves. Double-outlet right ventricle associated with persistent common atrioventricular canal. The surgical anatomy of common atrioventricular orifice associated with tetralogy of Fallot, double outlet right ventricle and complete regular transposition. Development of left atrioventricular valve regurgitation after correction of atrioventricular septal defect. Echocardiographic evaluation of atrioventricular orifice anatomy in children with atrioventricular septal defect. Morphometric analysis of unbalanced common atrioventricular canal using two-dimensional echocardiography. Predicting feasibility of biventricular repair of right- dominant unbalanced atrioventricular canal. Correction of atrioventricular septal defect: results influenced by Down syndrome? Complete atrioventricular canal associated with tetralogy of Fallot: morphologic and surgical considerations. Prevalence of left-sided obstructive lesions in patients with atrioventricular canal without Down syndrome. Atrioventricular septal defect – anatomic characteristics in patients with and without Down syndrome. Pulmonary vascular resistance in complete atrioventricular septal defect: a comparison between children with and without Down syndrome. Does Down syndrome affect prognosis of surgically managed atrioventricular canal defects? Surgical anatomy and pathology of the conduction tissues in atrioventricular defects. Surgical anatomy and management of the mitral component of atrioventricular canal defects. Efficacy of pulmonary artery banding in infants with complete atrioventricular canal. Should repair of atrioventricular septal defect be delayed until later in childhood? Determinants of early and late results of repair of atrioventricular septal (canal) defects. Anatomically sound, simplified approach to repair of “complete” atrioventricular septal defect. Simplified single patch technique for the repair of atrioventricular septal defect. Atrioventricular septal defects: lessons learned about patterns of practice and outcomes from the congenital heart surgery database of the Society of Thoracic Surgeons. Complete atrioventricular canal: comparison of modified single-patch technique with two-patch technique. Intraoperative echocardiography for atrioventricular canal: decision-making for surgeons. Potentially parachute mitral valve in common atrioventricular canal: pathological anatomy and surgical importance. Management of zone of apposition in parachute left atrioventricular valve in atrioventricular septal defect. Surgical treatment of double-orifice mitral valve in atrioventricular canal defects. Biventricular repair in children with atrioventricular septal defects and a small right ventricle: anatomic and surgical considerations.
Sominex 25 mg order with amex
The benefit of fractionated/unfractionated heparin/oral drugs and duration of anticoagulant therapy needs further evidence sleep aid like ambien 25 mg sominex free shipping. But in clinical practice sleep aid tablets buy sominex from india, development of new pituitary hormone deficiencies after surgery does not exclude cure sleep aid gaba order sominex online. The term “remission” seems to be more appropriate than “cure” for patients with pituitary Cushing’s syndrome, as they require long-term surveillance for years together (>10 years) to define cure. However, this definition should not be applied to those who have undergone bilateral adrenalectomy. Pituitary hormone deficien- cies also occur even in patients with ectopic Cushing’s syndrome due to pro- longed suppressive effects of cortisol on pituitary cells, particularly corticotropes and somatotropes. The predictors of cure in Cushing’s disease are well-localized microadenoma without parasellar extension, postoperative 0800h cortisol between day 1 and 7 < 50 nmol/L (1. Of these criteria, immediate postoperative hypocortisolemia is the best predictor of cure with a sensitivity of 85%. In clinical practice, the terms “remission” and “cure” are used interchange- ably; however, they are not synonymous. Remission can be defined as resolu- tion of clinical stigmata of Cushing’s and achievement of eucortisolemia with recovery of hypothalamo–pituitary–adrenal axis or hypocortisolemia requir- ing long-term glucocorticoid replacement. However, patients in remission have a probability of recurrence of the disease anytime during surveillance; therefore, prospective follow-up for at least 10 years is required to consider the patient as cured, as the probability of recurrence is 10–20% at 10 years for microadenomas. Therefore, patients with sustained remission and not requir- ing glucocorticoid replacement at 10 years probably represent cure. Hence, all patients who are cured are in remission, while all patients in remission may not be cured. How to define persistence or recurrence of disease in pituitary Cushing’s syndrome? However, it is reason- able to define persistence of disease (failed surgery) if there is no resolution of clinical and/or biochemical hypercortisolemia 6–12 weeks postopera- tively or if there is reappearance of clinical and/or biochemical hypercorti- solemia within 1 year. Recurrence is as resurgence of clinical and/or biochemical hypercortisolemia after being in remission for at least 1 year postoperatively. An immediate postoperative 0800h plasma cortisol <50 nmol/L is the best predictor of long-term remission with a recurrence rate of approximately 10% at 10 year. A 0800h plasma cortisol >140 nmol/L in the immediate postoperative period suggest lower probability of achieving remission. A 0800h cortisol between 50 nmol/L and 140 nmol/L also predicts long-term remission, as the recurrence rate in these patients appear similar to those with a 0800h cortisol <50 nmol/L. In addition, immediate 0800h cortisol also helps to decide the need for glucocorticoid supplementation; however, the cutoffs of serum cortisol for defining adrenal insufficiency are different from those to predict remission. Patients with a 0800h cortisol <100nmol/L require hydrocortisone supplementation irrespective of presence or absence of symptoms, whereas those with a serum cortisol >350 nmol/L can be fol- lowed up without any replacement. Patients with a 0800h cortisol between 100–350 nmol/L should be closely monitored for signs of adrenal insuffi- ciency and be replaced with hydrocortisone in the presence of symptoms of adrenal insufficiency. Timing Monitor Remarks Intraoperative Blood pressure If hypotension, take sample for cortisol and Blood glucose start hydrocortisone supplementation Electrolytes Immediate Symptoms of adrenal 0800h cortisol at least 2–3 samples, between postoperative insufficiency day 1–7 Blood pressure 0800h cortisol < 100 nmol / L Blood glucose Supplement hydrocortisone Electrolytes 0800h cortisol 100–350 nmol / L Urine output Monitor closely for signs of adrenal insufficiency and replace with hydrocortisone if required 0800h cortisol > 350 nmol / L Close follow-up 57. However, glucocorticoid supplementa- tion should be continued based on 0800h cortisol and presence or absence of symptoms of adrenal insufficiency. A patient with immediate postoperative 0800h cortisol value <50 nmol/L has high likelihood of cure, with a recurrence rate of 10% at the end of 10 years. The index patient should be supplemented with glucocorticoids as her cortisol is <100 nmol/L. She needs reevaluation at 6 weeks (after withholding hydro- cortisone for 24 h) to assess for remission and the need for glucocorticoid sup- plementation. If 0800h cortisol >140 nmol/L, patient requires further evaluation to rule out hypercortisolemia. Her postoperative day 3 0800h cortisol value is 210 nmol/L (7 μg / dl ), and day 7 0800h cortisol value is 162 nmol/L (6 μg/dl). She should be reevaluated again at 6 weeks, as some patients may have a delayed remission. If 0800h cortisol remains >140 nmol/L (∼5 μg/dl) even 118 5 Cushing’s Syndrome: Diagnosis and Treatment beyond 6 weeks, it needs further evaluation for persistence of disease. However, at 6 weeks if cortisol is <140 nmol/L (∼5 μg/dl), then the patient is considered to be in remission and needs follow-up. The index patient had a 0800h cortisol of 81 nmol/L (∼3 μg/dl) at 6 weeks and she is under follow-up.
Buy sominex us
Usually it can be treated by local resection insomnia 40 weeks pregnant generic 25 mg sominex, although in some patients a modified Konno procedure may be necessary (79 insomnia movie generic 25 mg sominex otc,80 insomnia kamelot lyrics discount sominex master card,81,82). Repeat valve repair is possible if the dysplasia is not severe or when the mechanism of regurgitation is through a residual cleft. Eccentric commissural annuloplastic sutures often are needed to correct central regurgitation. Patient–prosthetic mismatch in patients who required valve replacement during infancy or early childhood will merit valve re-replacement. The small valve requires replacement with a larger prosthesis, and there are no reliable techniques for annular enlargement. Thorough debridement and excision of fibrous scar and old prosthetic material is necessary. In rare circumstances, the new larger prosthesis is sewn into the left atrium in a supra-annular position. Others have described alternative approaches, including reconstruction of the deficient inlet septum, septal myectomy, and apical-aortic conduits (79,80,81,82). It occurs in the presence of pulmonary hypertension or in association with tetralogy of Fallot with right ventricular dysfunction and pulmonary valve regurgitation or stenosis. The patch (arrow) is attached to the right side of the atrial septum and the right atrioventricular valve to avoid damage to the conduction tissue and left atrioventricular valve. However, there are limited data in pediatric patients regarding the utility and feasibility of 3-D color Doppler quantitative assessment of regurgitation in these patients. In that setting, the echocardiographer should use indirect techniques such as assessment of ventricular septal flattening or bowing, right ventricular size and function, and Doppler interrogation of the pulmonary regurgitation velocity waveforms to assess pulmonary artery diastolic pressure. Note the tear in the leaflet (white arrow) just posterior to the repaired cleft (black dashed line). The larger jet (dashed black arrow) is through the tear just posterior to the repaired cleft and central to the cleft. The smaller jet is located near the atrial septum, within the repaired cleft itself (solid black arrow). The role of cardiac catheterization for some patients is to evaluate coronary artery anatomy or for calculation of pulmonary vascular resistance. If the rPa is elevated above this level, then provocative testing in the catheterization laboratory with the use of pulmonary vasoactive 2 agents such as nitric oxide is indicated. In this select group of patients, one would consider pre- and postoperative treatment with pulmonary vasoactive agents such as bosentan, sildenafil or Flolan, and documentation via hemodynamic catheterization of a substantial improvement in rPa during this therapy. In patients older than age 40 years, regardless of symptoms, noninvasive assessment of coronary artery disease typically is performed prior to surgery. However, for women with pulmonary vascular obstructive disease and severe pulmonary artery hypertension (pulmonary artery systolic pressure >60 mm Hg), pregnancy is not advised. Preferably, this should be at centers that specialize in the care of adults with congenital heart disease. The pioneering work performed by Giancarlo Rastelli in the 1960s is but one of these accomplishments. Acknowledgments The authors acknowledge the contributions of the former authors of this chapter (Drs. Surgical management of complete atrioventricular septal defect: Association with surgical technique, age, and trisomy 21. Actuarial survival, freedom from reoperation, and other events after repair of atrioventricular septal defects. Prevalence at birth, “natural” risk and survival with atrioventricular septal defect. Prospective diagnosis of 1006 consecutive cases of congenital heart disease in the fetus. Ethnicity, sex and the incidence of congenital heart defects: a report from the National Down Syndrome Project. Asplenia syndrome: insight into embryology through an analysis of cardiac and extracardiac anomalies. Evaluation of risk factors for prediction of outcome in fetal spectrum of atrioventricular septal defects. Intracardiac septation requires hedgehog-dependent cellular contributions from outside the heart. Cleft anterior leaflet of the mitral valve with intact septa: a study of 20 cases.
Quality 25 mg sominex
Because of these advantages and limitations sleep aid hcl order sominex 25 mg mastercard, some prefer the combined use of T4 and T 3 sleep aid overdose order 25 mg sominex mastercard. However insomnia x macbook sominex 25 mg purchase, there is robust clinical data to suggest that use of T4 alone is associated with favorable outcome. Intravenous hydro- cortisone in stress doses (100 mg bolus followed by 4 mg/h infusion) should be supplemented in all patients anticipating adrenal crisis after T4 therapy. Other sup- portive measures include passive rewarming with blankets, correction of hypoglycemia, use of appropriate antibiotics, and use of vasopressors in fluid refractory hypotension. Poor prognostic factors include advanced age and associated comorbidities like heart failure and sepsis. Outcome is better in levothyroxine naive patients as compared to defaulters, as defaulters have no residual thyroid function. Hashimoto’s encephalopathy is a disorder characterized by altered mental state, seizures, myoclonus, ataxia, memory loss, and hyperreflexia. These patients are usually euthyroid, but can either be hypothyroid or hyperthyroid. The autoantibody against enzyme α-enolase is a specific marker for Hashimoto’s encephalopathy. However, due to the lack of a sensi- tive and specific marker, Hashimoto’s encephalopathy is a diagnosis of exclusion. Other immunosuppressive drugs like azathioprine or cyclophosphamide may be used in patients who either do not respond to steroids or relapse during treatment. The recovery is rapid (days to weeks) and prognosis is usually good, if diagnosed early. Levothyroxine has been tried in the management of obesity, dyslipidemia, heart failure, and refractory depression even in patients without hypothyroidism. Use of levothyroxine in these non-thyroidal diseases was based on the fact that patients with hypothyroidism who had these abnormalities recovered on treat- ment with levothyroxine. However, no study has established the efficacy of levothyroxine in patients with these disorders who have normal thyroid func- tion tests. On the contrary, over-replacement may be deleterious and may result in decreased lean mass, osteoporosis, and increased risk of atrial fibrillation. Rich blood supply, profuse lymphatic drainage, adherent thick capsule, and high iodine content of thyroid gland are effective barriers which prevent the lodgment of microorganisms and consequently infection of the thyroid gland. However, tuberculosis and Pneumocystis jirovecii may affect thyroid gland, particularly in those who are immunocompromised. Do patients with primary hypothyroidism need screening for other auto- immune endocrine disorders? The pretest probability of finding other autoimmune endocrine disorder in association with primary hypothyroidism is very low (3%); therefore, screening for other autoimmune endocrine disorder is not recommended. Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. On examination, her pulse rate was 124/min and regular, blood pressure was 160/60 mm Hg, and she had fine tremors with warm and moist palms. Ophthalmic examination revealed proptosis (22 mm) with a clinical activity score of 0/7 and severity score was moderate to severe. She was diagnosed to have Graves’ disease with inactive thyroid-associated orbitopathy and treated with carbimazole 30 mg once a day and propranolol 40 mg thrice daily. She was also advised artificial teardrops, sunglasses with side cover, and head-end elevation while sleeping. After 6 weeks, she had improvement in clinical symptoms and her body weight stabilized. The dose of carbimazole was decreased to 10 mg and continued for 2 years with 3 monthly monitoring of thyroid function tests. In such a scenario, thy- roid uptake/scan is not indicated to establish the diagnosis of thyrotoxicosis. However, thyroid scan should be performed in patients who present with short dura- tion of symptoms without orbitopathy to exclude the possibility of subacute thyroiditis. A serum T /T3 4 ratio >20 (ng/dl:μg/dl) suggests the presence of hyperthy- roidism rather than thyroiditis; the index patient had a serum T /T3 4 ratio of 23. She had bilateral proptosis sugges- tive of thyroid-associated orbitopathy and the clinical activity score of 0/7 suggests inactive eye disease. Hence, immunosuppressive therapy was not offered and she was advised supportive measures.

Purchase sominex 25 mg without prescription
The double root has been In infants insomnia 57 buy 25 mg sominex fast delivery, the friability of the muscle may result in an unac- popularized by Hu from Fuwai Hospital in Beijing China insomnia video game culture buy 25 mg sominex mastercard. Hypothermic less well over the longer term because of the thick fbrous circulatory arrest is reserved for very small premature babies neointima that soon covers it insomnia relaxation techniques 25 mg sominex purchase with visa. Low fow hypothermic bypass with a single Particular care must be taken at the mid-point of the baffe venous cannula may be preferred for babies between 2 and 3 tunnel to ensure that a “waist” is not created where the pul- kg if the usual infundibular approach is employed. Air entrainment into the single venous cannula is usu- that sutures will tear out of the raw muscle surface. Muscle tra- After application of the aortic cross-clamp and administra- beculations often extend up to the annulus, creating “ridges tion of cardioplegic solution, an infundibular incision is made and valleys. As in tetralogy, great care is taken in making the inci- stenosis is largely achieved by division of the septal and pari- sion to preserve as many coronary arteries as possible. Often, etal extensions of the conal septum with or without excision there is a long conal coronary artery that may reach well of the conal septum itself. It is important that the infun- The ventricular incision should virtually never be closed dibular incision is carefully planned to preserve this artery. A patch fully defned, and the length of the conal septum is assessed of autologous pericardium is used to close the infundibular with respect to both the aortic and pulmonary valves. If the pul- presence of tricuspid chordal attachments to the conal sep- monary annulus is too small, it may be necessary to place a tum is noted. Usually, excision of the conal septum helps the same as that used for tetralogy (see Chapter 19, Tetralogy to relieve the subpulmonary stenosis to some degree (Fig. Both these materials are less likely to acquire a thick fbrous pseudointima than Dacron. There is also greater pliability of the baffe so that a kink is less likely to project into the central point of the pathway. The aorta is reconstituted by direct 25 fow tract, the so-called “Nikaidoh procedure” (Fig. If In addition, it is usually necessary to mobilize, explant, and this is not done, either the right or the left pulmonary artery must traverse an excessively long course around the aorta, subsequently reimplant the coronary arteries (Fig. It When the great vessels take up a more side-by-side rela- is helpful to rotate the translocated aortic root by 180° (Fig. A Lecompte maneuver is performed bring- terior direction, but there is also translocation in a supero- ing the pulmonary arteries anterior to the divided aorta (Fig. In addition, careful Thus the Nikaidoh procedure involves many “modules” from consideration must be given to the relationship of the anterior the Ross and arterial switch procedures that are familiar to coronary artery (usually the right coronary artery as it arises the congenital cardiac surgeon. There is also a small risk of late coronary artery the ventriculotomy from the pulmonary arteries. In addi- stenosis and occlusion as has been seen with the arterial tion, the severe tension that would result from the distance switch procedure. The branch pul- monary arteries are widely mobilized and the ductus or ligamentum arteriosum is divided. The proximal main pulmonary artery is divided, the pulmonary valve is excised and the proximal stump of the main pulmonary artery is oversewn. The procedure can be performed using low fow when moderate subpulmonary stenosis is present. Similarly, hypothermic bypass with a single venous cannula for the very a bicuspid pulmonary valve should not be considered an small neonate less than 2 kg in weight. For the larger atrial inversion procedure or the lesser quality of life dictated neonate, greater than 2–2. With bicaval cannulation, it is often necessary to heart is flled with saline to exclude air before tying the suture. A single 564 Comprehensive Surgical Management of Congenital Heart Disease, Second Edition large pericardial patch is used to reconstruct the coronary minimized. However, this is rarely an issue today since mod- there is a long and somewhat narrow subaortic conus).
Cronos, 53 years: A few minutes compressing the puncture site peutic interventions that involve the arterial and venous with the fngers is enough to stop the bleeding in most system. Note that we generally avoid placement of tourniquets leagues described the extended aortoplasty technique for this around the arch vessels because we believe that the risk of lesion. Fetal cardiac size in normal, intrauterine growth retarded, and diabetic pregnancies.
Ketil, 62 years: However, if fltration is required for a prolonged period, effciency may be reduced due to the blocking of available pores. Incidence and management of life-threatening adverse events during cardiac catheterization for congenital heart disease. Operations for many patients can be delayed for months, depending on the degree of left ventricular outflow tract obstruction.
Sebastian, 42 years: Prenatal diagnosis of cerebral arteriovenous malformation using color Doppler ultrasonography: case report and review of the literature. The term ectopia implies an abnormal displacement away from the expected position. The posterior descending coronary artery arises from the left circumflex artery (left coronary dominance) in 27% of patients with truncus arteriosus (25), which is about three times the frequency of this variation in the normal population.
Tjalf, 28 years: There are multiple short-term and durable ventricular assist devices that have been utilized successfully in pediatric patients with refractory heart failure (89,90,91,92). The posterior aspect receives the two venae cavae and has a veinlike appearance, in keeping with P. Labelling is required so that the extended and chain terminated products can be detected after gel electrophoresis.
Stan, 46 years: Chromosome 22q11 deletion in patients with ventricular septal defect: frequency and associated cardiovascular anomalies. The ratio of genome size to fragment size is, however, an under-estimate of the complexity required for the construction of a library. The signal from stationary or relatively slow-moving tissues (such as the myocardium) is gray because the spins within the selected slice have reduced signal intensity (i.
Masil, 58 years: A harsh holosystolic murmur is heard at the left lower sternal border and is more evident as the pulmonary vascular resistance drops, along with a diastolic rumble at the apex. This has important functional implications since increasing matrix stiffness changes cardiomyocyte force production. These approaches also assumed adequate total cardiac output to meet oxygen delivery needs if Qp/Qs is optimized.
Denpok, 36 years: Another aspect of 24-hour ambulatory blood pressure monitoring that may be useful is the normal decline in blood pressure observed at night during sleep (240). The secreted morphogen Shh activates forkhead-containing transcription factors, which directly regulate Tbx1, by which its expression is maintained in the secondary heart field progenitors (278,279). Wedge filters should be positioned in the corners of the radiographic field to further improve image quality, but should not be considered a major strategy for reduction of radiation exposure.
Akascha, 32 years: These patients should have blood pressure lowered below the 90th percentile for age, sex, and height as they are thought to be at highest risk for cardiovascular disease over time. Clonal selection is the most widely accepted theory that explains the immune system and contains four major points as follows: A. Why is cholecalciferol/ergocalciferol and not calcitriol used for the treatment of vitamin D defciency?
Marlo, 65 years: In patients whose associated cardiovascular anomalies require surgical therapy that involves redirection of the systemic venous return to the pulmonary arteries (bidirectional Glenn and modified Fontan procedures), awareness of the anomaly and appropriate surgical planning are important. The clinical and diagnostic significance of anti-myosin autoantibodies in cardiac disease. Others remain concerned about the neurologic effects of neonatal cardiopulmonary bypass and hypothermic circulatory arrest and the possible increased incidence of transannular patching when operating on a very small and young baby and continue to prefer the staged (surgical or catheter-based) approach for very young symptomatic infants, with later full repair.
Fraser, 24 years: Successful treatment of anteroseptal accessory pathways by transvenous cryomapping and cryoablation. Impact of age and duration of banding on left ventricular preparation before anatomic repair for congenitally corrected transposition of the great arteries. Effects of exercise and respiration on blood flow in total cavopulmonary connection: a real-time magnetic resonance flow study.
Diego, 57 years: Uteroplacental blood flow, cardiac function, and pregnancy outcome in women with congenital heart disease. In this setting, the right mainstem bronchus may supply only the right upper lobe, with the remainder of the lung supplied by a bridging bronchus, or there may be complete absence of the right bronchial tree, with the entire lung supplied by a bridging bronchus. In a It is beyond the scope of this book to discuss the results of report from the United Kingdom, Thomson et al.
Bozep, 33 years: The hospital laboratory is then responsible for billing and recovering the refer- ral laboratory charges from either the patient’s insur- ance or the patient directly. For example, circulating fetal albumin in the neonate has significantly reduced binding affinity for acid drugs such as phenytoin which is extensively (∼94% to 98%) bound to albumin in adults as compared to 80% to 85% in the neonate. These studies are notable for their systematic, longitudinal, and prospective design, and will hopefully continue to generate important outcome data on older children and adults, with fewer biases and greater generalizability than clinic-based case series on which most current data derives.
Jose, 48 years: Patients with ectopic Cushing’s syndrome and large invasive pituitary macroadenoma do not show this respon- siveness, even at higher doses of dexamethasone possibly because their threshold is set at a much higher level than in pituitary Cushing’s syndrome. The chest radiograph may show variable peripheral lung fields, depending on the amount of pulmonary blood flow. Unfortunately, those trying to cial ingredient in making an accurate diagnosis at improve their skills by repetitive microscopic evalua- the time of the offce visit.
Tukash, 25 years: If a frontal sinus drainage pathway cannot tal sinus drainage pathway anterolaterally (best seen on be found, they can track an instrument tip so that the pathway the axial scans, Fig. In younger children, the S-to-D velocity ratio is typically <1, a finding that differs from the older adolescent and adult population for which the S/D-wave velocity ratio in normal subjects is typically >1. Platelet clumping in the col- lection tube can signifcantly lower than the platelet count when it is quantitated in a cell counter.
Kor-Shach, 38 years: Plain flms may demonstrate graphically as a multiloculate fuid collection in the central the calculus responsible for the obstruction. For these anomalies, perhaps the term collateral vein would suffice (analogous to collateral arteries in cases of pulmonary atresia with ventricular septal defect). This papillary muscle angle does not change throughout the cardiac cycle, despite the influence of ventricular contraction and torsion of the left ventricle.
9 of 10 - Review by T. Porgan
Votes: 229 votes
Total customer reviews: 229
References
- DeOliveira ML, Cunningham SC, Cameron JL, et al. Cholangiocarcinoma: thirty-one-year experience with 564 patients at a single institution. Ann Surg. 2007;245(5):755-762.
- Mayer J, Boldt J, Schollhorn T, Rohm KD, Mengistu AM, Suttner S. Semi-invasive monitoring of cardiac output by a new device using arterial pressure waveform analysis: a comparison with intermittent pulmonary artery thermodilution in patients undergoing cardiac surgery. Br J Anaesth. 2007;98(2):176-182.
- Menon V, Harrington RA, Hochman JS, et al: Thrombolysis and adjunctive therapy in acute myocardial infarction: The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126:549S-575S. 14.
- Cascino TL, Kori S, Krol G, et al. CT of the brachial plexus in patients with cancer. Neurology 1983; 33(12):1553-1557.
- Bonderman D, Skoro-Sajer N, Jakowitsch J, et al: Predictors of outcome in chronic thromboembolic pulmonary hypertension, Circulation 115(16):2153-2158, 2007.
- Mackie RM. Incidence, risk factors and prevention of melanoma. Eur J Cancer 1998;34:S3-S6.