Teresa M. Bieker, MBA-H, RDMS, RDCS, RVT
- Lead Sonographer
- Division of Ultrasound
- University of Colorado Hospital
- Aurora, Colorado
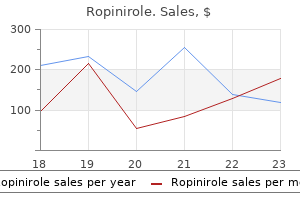
Ropinirole dosages: 2 mg, 1 mg, 0.25 mg, 0.5 mg
Ropinirole packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Cheap ropinirole 0.5 mg free shipping
Finally medications an 627 order ropinirole 0.5 mg without a prescription, renal transplantation kg/day) in 3–4 divided doses until proteinuria disappears is indicated in end-stage renal failure because of steroid- (usually it does not take more than 2 weeks) followed by 1 medicine x topol 2015 cheap ropinirole online amex. Infrequent relapses: Tis approach is applicable for subsequent relapses provided these are “infrequent” (3 or less in a year) medicine used to treat bv 0.5 mg ropinirole amex. Frequent relapses/steroid dependent: In case of fre- quent relapses (3 or more year), child should be treated with long-term alternate day regimen for 9–18 months. Prednisolone dose should be smaller but enough to keep the child free of proteinuria as well as side-efects. A short course (8–12 weeks) of steroid sparing agents (levamisole, cyclophosphamide, tacrolimus, mycophe- nolate mofetil, rituxamab or cyclosporine) is indicated in subjects who show frequent relapses or who are steroid dependent. But, it is the patient’s response to therapy rather than the renal histology that predicts the renal outcome. Patients requiring high dose furosemide or addition of other Calcineurin inhibitors: Cyclosporine, tacrolimus diuretics should be under close supervision, preferably in a hospital. Patients showing hypokalemia require potassium supplements Methylprednisolone or co-administration of spironolactone. Te organisms respon- sible for infection are Streptococcus pneumoniae and Gram-negative bacteria. Note the severe knock knee deform- ity and mottling of skin around knees in a child with chronic renal failure. Hypovolemic shock Acute kidney injury ses, pathological metaphyseal fractures, metastatic Chronic calcium and vitamin D defciency state with calcifcation, pruritus and mottling of skin around symptomatic hypocalcemia (tetany) and/or rickets/ knees and thighs. Radiology shows periosteal erosions in middle usually shows permanent remission or diminution in and distal phalanges, distal clavicle and inner aspect of relapses during puberty is a myth. Undoubtedly, Tis term refers to skeletal changes that may develop in the basic etiologic condition also needs to be attended to chronic renal disease characterized by chronic glomerular for lasting results. In preschool Etiology children with osteodystrophy, congenital malformations Te causes may be: of the kidney are the leading cause. Preventable (uncommon): Usually diagnosed late, and Clinical Features Unpreventable (common): Congenital anomalies, renal Growth failure, dwarfsm, wasting, muscle weakness, dysplasia with obstructive uropathy and various forms of bone pain, bone deformities, slipped femoral epiphy- persistent glomerulonephritis. For detailsSeeChapter 6 (Developmental, Renal transplant is the eventual goal in end-stage Behavioral and Psychiatric Disorders). It may be carried out using cadaver or living related donor as source for the organ graft. Success Details relevant to the needs of the pediatric scholars are rate in children over 5 years of age is as high as in adults. Renal function after birth continues to improve until it approaches adult level by the end of 2 years B. Infantile polycystic disease of kidneys is inherited as an autosomal dominant disease whereas adult type is inherited as an autosomal recessive disease D. Most cases belong to the “idiopathic” type with overwhelming predominance of minimal change lesion C. In minimal change lesion, classical lesion is in the form of thickening of the foot processes (podocytes) of the basement membrane D. It is advisable to rule out tuberculosis before starting steroid therapy which may reactivate a dormant tuberculous focus E. All children with acute glomerulonephritis should receive penicillin or an allied drug during acute phase B. Benign proteinuria with urine protein never exceeding 1 g/24 hours may be orthostatic, febrile or exercise-induced C. A triad of microangiopathic hemolytic anemia, thrombocytopenia and acute kidney injury B. Most cases in India are associated with acute shigellosis in the form of bloody diarrhea or simple gastroenteritis C. Muscle cramps and carpopedal spasm are the only known manifestations of Bartter syndrome E. Gross hematuria originating from kidneys gives urine bright red or pink color Answers 1. B 632 Clinical Problem-solving Review 1 A 4-year-old presents with massive hypoproteinemic edema, massive hypoproteinemia and hypercholestrolemia. He responds to standard therapy with prednisolone (2 mg/kg/day daily for 6 weeks and then 1. What are likely iatrogenic complications other than Cushingoid features in such a case?
Generic ropinirole 1 mg
When using a catheter during fight medicine jewelry ropinirole 0.25 mg purchase on-line, the balloon should be flled with water instead of air symptoms 6 days before period due ropinirole 2 mg lowest price, because the gas can expand 30% in volume in the low-pressure environment at altitude [3] treatment hiatal hernia purchase ropinirole overnight delivery. The patient should be monitored for hypo- tension caused by post-obstructive diuresis. If a urinary catheter cannot be obtained, the medical care provider should alert ground control of the need for passenger treatment. Ground control can organize equip- ment and personnel to be available at the plane’s fnal destination. As for any medi- cal evaluation and intervention provided during a fight, the care provider should ensure documentation, typically using forms provided by the airline. Anaphylaxis is an IgE-mediated allergic response that causes mast cells and basophils to degranulate and release histamine, tryptase, and heparin, as well as leukotrienes and cytokines. The affected person experiences an initial reaction and then, possibly, a late-phase or delayed reaction from the additional release of infammatory mediators (sometimes referred to as a biphasic reaction). The released substances can affect the cardiovascular, respiratory, gastrointestinal, integumentary, and central nervous systems. Cardiovascular symptoms include hypotension, lightheadedness, syncope, arrhyth- mias, and angina. Gastrointestinal symptoms include nausea, vomiting, diarrhea, and abdominal cramping. Effects on the integumentary system include the classic symptoms of an allergic reaction: fushing, erythema, pruritis, urticaria, and angioedema. Central 12 Other Presentations 117 nervous system manifestations include headache, confusion, and altered mental sta- tus [4]. The clinical diagnosis of anaphylaxis can typically be made when one of the fol- lowing 3 criteria is met. First, the patient has an acute cutaneous manifestation that leads to respiratory compromise or hypotension. Second, 2 or more systemic symp- toms (cutaneous manifestations, respiratory compromise, or gastrointestinal symp- toms) develop rapidly after exposure to an allergen. Third, the blood pressure drops after exposure to a known allergen (30% decline from baseline blood pressure) [5]. Various agents can trigger anaphylaxis; medications and foods induce particular concern in the fight environment. Foods are the most common cause of anaphylaxis and are responsible for as many as 30% of fatalities [5]. Peanut and tree nut allergies have been well publicized as causes of anaphylaxis, not just by personal exposure but also by proximity to the allergens. Anaphylaxis can also be induced by medica- tions, particularly an antibiotic or analgesic that the affected person started to use recently. When assessing a patient with anaphylaxis during a fight, the healthcare provider should perform a primary assessment, including assessing the patient’s airway, breathing, and circulation. Breathing can be affected by bronchospasm and the patient might be signifcantly hypotensive. Patients with severe allergic reactions can have an altered level of consciousness, and 90% of them have cutaneous mani- festations [6]. An infusion can be made during fight, while waiting for landing, by injecting 1 mg of the 1:1,000 or 1:10,000 formulation into a 1 L bag of normal saline, yielding a fnal concentration of 1 mcg/mL. This solution can be run wide open as a temporiz- ing measure to maintain the patient’s hemodynamics [7]. Patients should also receive an antihistamine such as diphenhydramine, which is also required in the medical kit. They are not required in the onboard medical kit, but they might be available from other passengers. Patients experiencing broncho- spasm can receive albuterol via a meter-dosed inhaler. The patient’s vital signs, including blood pressure, should be monitored for improvement with treatment. Bostick Flight diversion should be considered when a passenger experiences anaphy- laxis, especially if the person does not respond to treatment. The healthcare provider should communicate with the crew about potential diversion, which is ultimately the decision of the captain.
1 mg ropinirole amex
Femoral nerve blocks have a relatively low rate of complications and few contraindications medicine quiz generic ropinirole 0.5 mg fast delivery. Local infection treatments for depression discount ropinirole, previous vascular grafting medications vertigo cheap 0.25 mg ropinirole fast delivery, and local adenopathy should be carefully considered in patient selection. Insert a short (5-cm) insulated needle at an angle 45 degrees to the skin in a cephalad direc- tion until a clear quadriceps twitch is elicited at a current below 0. Ultrasonography: Visualize in cross-section the femoral artery and femoral vein, with the overlying fascia iliaca. Just lateral to the artery and deep to the fascia iliaca, the femoral nerve appears in cross-section as a spindle-shaped structure with a “honeycomb. Insert the needle in parallel to the ultrasound transducer just lateral to the outer edge. Advance the needle through the sartorius muscle, deep to the fascia iliaca, until it is visualized just lateral to the femoral nerve. Fascia iliaca technique: When the inguinal ligament and femoral artery pulse are identified, divide the length of the inguinal ligament into thirds. Two cm distal to the junction of the middle and outer thirds, insert a short, blunt-tipped needle in a slightly cephalad direction. As the needle passes through the two layers of fascia in this region (fascia lata and fascia iliaca), two “pops” will be felt. When the needle has passed through the fascia iliaca, aspirate and inject 30 to 40 mL of local anesthetic. This block usually anesthetizes both the femoral nerve and lateral femoral cutaneous nerves. Note that all sciatic nerve blocks fail to provide complete anesthesia for the cutaneous medial leg and ankle joint capsule, but when a saphenous (or femoral) block is added, complete anesthesia below the knee is pro- vided. The major site-specific risk of a popliteal block is vascular puncture, owing to the sciatic nerve’s prox- imity to the popliteal vessels at this location. Palpate the ham- string muscles to locate the point where the biceps femoris (lateral) and semimembranosus/semitendinosus complex (medial) join. Having the patient flex the knee against resistance facilitates recognition of these structures. Advance an insulated needle (5–10 cm) until foot plantar flexion or inversion is elicited (dorsiflexion acceptable for analgesia). A volume of 30 to 40 mL of local anesthetic is often required for single-injection popliteal–sciatic nerve block. Ultrasonography: With the patient positioned prone, identify the popliteal fossa apex. Using a transducer placed in a transverse orientation, identify the femur, biceps femoris muscle, popliteal vessels, and sciatic nerve or branches in cross-section. The nerve is usually posterior and lateral (or immediately posterior) to the vessels and is often located in close relationship to the biceps femoris muscle just deep to its medial edge. For an out-of-plane technique, insert the needle just caudad to the ultrasound transducer and direct it anteriorly and slightly cephalad. When the needle is positioned in proximity to the sciatic nerve, aspirate and inject local anesthetic, observing spread around the nerve. For an in-plane technique, insert the block needle lateral to the ultrasound transducer, traversing (or just anterior to) the biceps femoris muscle. Advance the needle in the ultrasound plane, visualizing approach of the needle either deep or superficial to the nerve. Epicritic (non-noxious): Epicritic sensations (light touch, pressure, proprioception, and temperature dis- crimination) are characterized by low-threshold receptors and are generally conducted by large myelinated nerve fibers. The International Association for the Study of Pain defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Somatic pain: Further classified as superficial or deep Superficial somatic pain is caused by nociceptive input arising from skin, subcutaneous tissues, and mucous membranes. Characteristically well localized and described as a sharp, pricking, throbbing, or burn- ing sensation. Visceral pain: Visceral acute pain is caused by a disease process or abnormal function involving an internal organ or its covering (e.
Purchase ropinirole in united states online
Bladder/Urethral Pain Pain medicine natural buy cheap ropinirole 0.5 mg on-line, discomfort mueller sports medicine order generic ropinirole line, and pressure are part of a spectrum of abnormal sensations felt by the individual medicine gabapentin order genuine ropinirole line. Pain produces the greatest impact on the patient and may be related to bladder filling or voiding, may be felt after micturition, or be continuous. Pain should also be characterized by type, frequency, duration, and precipitating and relieving factors and by location such as bladder, urethral, vulval, vaginal, and perineal pain. Dysuria, strangury, and bladder spasm are not recommended terms as these symptoms are difficult to define. Urethral Pain This is felt in the urethra and the individual indicates the urethra as the site [1]. It is often described as “burning on passing urine” and can be aggravated by sexual intercourse. As an isolated symptom, it is associated with urinary tract infections or urethritis. Bladder Pain Bladder pain is felt suprapubically or retropubically and usually increases with bladder filling [1]; it may also persist after voiding. Bladder pain may be associated with inflammation of the bladder, bladder stones, or tumor. Some women complain of pain after voiding, which might be associated with detrusor overactivity. The presence of bladder pain is an indication for cystoscopy and occasionally bladder biopsy. Endometriosis on the bladder may cause urethral pain, which is present at certain times in the menstrual cycle. Pelvic inflammatory disease may cause urethral pain; however, the woman will often have symptoms of vaginal discharge and pyrexia. The pain is referred from the sensory nerves innervating the kidney and ureter, for which there are many causes (Table 28. This becomes more acute as the pressure generated within the urinary tract is higher. Loin pain during voiding and loin pain associated with urgency in women with detrusor overactivity may indicate vesicoureteric reflux. Superficial dyspareunia may be associated with vaginal dryness or following episiotomy or vaginal wall repair. Dyspareunia associated with compression of the anterior vaginal wall may reflect bladder or urethral pain syndromes. Perineal pain is felt between the posterior fourchette and the anus and may be persistent or recurrent episodic. It may be related to the micturition cycle or associated with symptoms suggestive of urinary tract or sexual dysfunction [1]. Women may describe the feeling of a lump, heaviness, a dragging sensation in the vagina, or lower back pain. They may also describe the learned behavior of using their fingers to reduce the bulge in order to successfully micturate or defecate, which is referred to as digitation. As vaginal prolapse alters the range of treatments for urinary incontinence, enquiries about symptoms of vaginal prolapse and prolapse affecting micturition and defecation should be made. The feeling of a lump at or beyond the vaginal introitus, low back ache, heaviness, dragging sensation, or the need to digitally replace or support the prolapse in order to defecate or micturate are among the symptoms that may be described. Over 40% of women with urethral sphincter incompetence will also have significant cystoceles, making this an important symptom affecting management of a woman’s urinary incontinence. As vaginal prolapse can mask urethral sphincter incompetence (occult incontinence) it is important to identify any prolapse before a urodynamic test so that a vaginal ring can be inserted during the filling phase of urodynamics to expose any underlying urethral incompetence (21). Hematuria 416 Visible blood in the urine (“frank hematuria”) should always be investigated as a priority, according to national guidelines. Microscopic hematuria should also be investigated, but trace amounts of blood on dipstick urinalysis can probably be disregarded. Previous continence operations have an important influence on the future success of continence surgery, as the urethral sphincter may be altered by scarring and damage to sphincter innervation by previous vaginal surgery, as well as distortion and narrowing of the bladder neck.
2 mg ropinirole buy
Changing the site of stimulation may modify the ability of a stimulated impulse to reach the tachycardia site in time to terminate it medications 5 songs order ropinirole paypal. The resetting response curve from a tachycardia that was unable to be reset or terminated from the right ventricular outflow tract yet could be both reset and terminated by the right ventricular apex is shown in Figure 11-199 symptoms of ebola 0.25 mg ropinirole order visa. Using single or double extrastimuli treatment rosacea generic ropinirole 0.25 mg buy online, this site specificity for termination may be demonstrated in 15% to 20% of cases. In a similar manner, single or double extrastimuli delivered from the left ventricle may terminate a tachycardia where comparable stimulation from the right ventricle failed (Figs. We have not been able to predict which tachycardias will demonstrate site specificity for facilitation of termination aside from P. The lack of relationship between site specificity for resetting and termination may have to do with the relationship of the site of entry in the excitable gap and the site of termination. B: Premature stimulus at twice threshold fails to capture the ventricle at a coupling interval of 240 msec. C: The stimulating current is increased to 5 mA, and the coupling interval is shortened in 10-msec decrements, with ventricular capture maintained at 220 msec. E: When the stimulus current is increased at 10 mA, ventricular capture is possible at a coupling interval of 210 msec and the tachycardia is terminated. Termination of ventricular tachycardia with ventricular stimulation: Salutary effect of increased current strength. Perhaps with the new active fixation pacing leads, knowledge of site specificity for termination can be taken advantage of. As stated earlier, site specificity for either resetting or termination is not a P. A: A ventricular extrastimulus delivered at a coupling interval of 300 msec at twice diastolic threshold captures the ventricles but fails to terminate the tachycardia. C: When the current is increased to 5 mA, capture is possible at 250 msec, but termination does not occur. E: Finally, when the current is increased at 10 mA, capture at 240 msec is possible and results in termination of the tachycardia. Termination of ventricular tachycardia with ventricular stimulation: Salutary effect of increased current strength. Although in 40% to 50% of tachycardias, facilitation of termination does occur following procainamide (Fig. Neither the plasma level of procainamide nor the prolongation of tachycardia cycle length could predict which tachycardia would be more difficult to terminate. If this prolongation of conduction through intervening tissue is marked, termination of the tachycardia may be more difficult. Termination of ventricular tachycardia with ventricular stimulation: Salutary effect of increased current strength. This method of pacing, which takes advantage of our understanding of resetting phenomena, can be used to design an algorithm that can be employed in antitachycardia pacemakers. Sustained ventricular tachycardia in coronary artery disease—Evidence for reentrant mechanism. Effect of Drugs on Ventricular Tachycardia Unfortunately, aside from adenosine, we do not have antiarrhythmic agents that are effective for a specific type of tachycardia mechanism. If we did, one could theoretically separate reentry from triggered activity, or automaticity, based on the response of the tachycardia to the drug and P. However I do not believe adenosine should be used in patients with significant coronary artery disease because it can produce a “coronary steal” and result in ventricular fibrillation. For example, triggered activity, whether or not associated with digitalis intoxication, can be abolished by verapamil or lidocaine, and when triggered activity is catecholamine P. In such cases, triggered activity is also 125 126 359 abolished by calcium blockers and/or beta blockers. This slower tachycardia is now readily terminated by a single right ventricular extrastimulus. A and B: This results in the ability of single extrastimuli to depolarize the ventricles at coupling intervals <360 msec.
1 mg ropinirole purchase mastercard
These functional changes cannot be identified by clinical neurophysiology and only when entrapment is severe enough do abnormalities appear medications hypothyroidism generic 2 mg ropinirole with mastercard. Segmental demyelination results in conduction block with focal nerve conduction slowing medications 5 rights 0.25 mg ropinirole with mastercard, which may not be identified in the short length of the pudendal nerve measured symptoms 37 weeks pregnant discount 2 mg ropinirole visa. Also, these techniques investigate motor functions, whereas symptoms and signs are mainly due to sensory dysfunction [69]. Currently, measuring pudendal nerve latencies in incontinence is not recommended [70]. A selective needle recording of a (sphincter or pelvic floor) muscle response (M wave) on appropriate electrical stimulation may be informative in selected patients with suspected “lower motor neuron– type” lesions. Anterior Sacral Root (Cauda Equina) Stimulation Transcutaneous stimulation of deeply situated nervous tissue became possible with the development of special electrical [71] and magnetic [72] stimulators. When applied over the spine, these stimulators stimulate mainly the roots at the exit from the vertebral canal [73]. It has been shown that responses from gluteal muscles may contaminate attempts to record from the sphincters and lead to error [77]. Positioning of the ground electrode between the recording electrodes and the stimulating coil should decrease the artifact (Figure 36. Stimulation of the roots may be used to obtain a peripheral conduction time so that a central conduction time (see next section) can be calculated [79]. Assessment of Central Motor Pathways Using the same magnetic or electrical stimulation as mentioned earlier, it is possible to stimulate the motor cortex and record a response from the pelvic floor. Magnetic stimulation is less unpleasant; electrical cortical stimulation is nowadays only used intraoperatively in anesthetized patients. The mean latencies were between 30 and 35 ms if no “facilitatory maneuver” was used. Central conduction times of approximately 22 ms without and about 15 ms with the facilitation (i. Substantially, longer central conduction time in patients with multiple sclerosis and spinal cord lesions as compared to healthy controls have been found [1], but all those patients had clinically recognizable cord disease. Normative values for the urethral sphincter and the puborectal muscle in adult women have been reported for transcranial magnetic stimulation [80,81]. It has been demonstrated that in comparison to the motor area for hand muscles, the anal sphincter motor cortex has less intracortical inhibition [83]. Because of the significant influence of voluntary contraction, there is a possibility of variability of both total conduction times and central conduction times. Later negative (at around 55 ms) and then further positive waves are interindividually quite variable in amplitude and expression and furthermore have little known clinical relevance. Special techniques of stimulation isolate each dorsal clitoral nerve and may be more sensitive at locating the precise site of pathology [90]. A study that looked at the value of the pudendal evoked potential when investigating urogenital symptoms for detecting relevant neurological disease found it to be of lesser value than a clinical examination looking for signs of spinal cord disease in the lower limbs, i. There may, however, be circumstances in routine diagnostics— such as when a patient is complaining of loss of bladder or vaginal sensation—that it is reassuring to be able to record a normal pudendal evoked response. The first reflex component is spurious at the applied stimulation strength, which was two-times sensory threshold; the second (late) reflex component is obvious. When making such measurements, it is of utmost importance to use bipolar stimulation in the bladder or proximal urethra; otherwise, somatic afferents will be depolarized [95,96]. The typical latency of the most prominent negative potential (N1) is approximately 100 ms [95,97]. There are two reflexes—the anal and the bulbocavernosus—that are commonly clinically elicited in the lower sacral segments; both have the afferent and efferent limb of their reflex arc in the pudendal nerve and are centrally integrated at the S2– S4 cord levels (Figure 36. The pudendal nerve itself may be stimulated by applying needle electrodes transperineally [101] or by using “St Mark’s electrode” [102]. Bladder neck/proximal urethra can be stimulated using a catheter-mounted ring electrode [96] and reflex responses obtained from perineal muscles.
Ropinirole 2 mg on line
Secondary mastoplasty: Alterations of sensitivity: the presence of an implant can alter the patient’s local sensitivity treatment 4 burns buy generic ropinirole online, that can be exalted or • In presence of a fibrous reaction: removal of the capsule depressed symptoms hypoglycemia generic 2 mg ropinirole visa, either temporarily or permanently 7 medications that can cause incontinence purchase ropinirole 0.25 mg amex. Smoking delays the reparative process and thus can lead to the implant Bibliography extrusion. Hedén P, Olenius M, Tengvar M (2011) Macrolane for breast scar related deformities, implant displacement, inadequate enhancement: 12-month follow-up. Plast Reconstr Surg dimensions, lack of symmetry, undesired shape, palpability 127(2):850–860 2. Ann testable scientific papers on this matter, is considered to be Plast Surg 24(3):293–296; discussion 297 4. At any time a surgical procedure can be and progenitor cells as fillers in plastic and reconstructive surgery. Plast Reconstr Surg 118(3 Suppl):121S–128S Manufacturers’ guarantee: manufacturers put adequate 5. Plast Reconstr Surg 113(1):391–395; dis- they neither guarantee positive results nor exclude inconve- cussion 396–397 niences in relation to the clinical use of these implants. Plast Reconstr Surg 109(4):1396–1409; discussion 1410–1415 Positioning the implant consider that the traction leads to 11. Plast Reconstr Surg 112(2):456–466 Cosmetic Breast Augmentation with Fat Grafting Daniel Del Vecchio and Roger Khouri 1 Introduction chapter is to clearly outline a rationale for the current tech- nique of mega volume fat grafting to the breast used for cos- For fat grafting to emerge as a viable technique for breast metic augmentation. Such a standard using unaltered augmentation, it must be safe for patients, yield reproducible adipocyte graft may serve as a benchmark for comparing results that satisfy aesthetic goals, and be reliably performed mega-volume fat grafting for breast augmentation using in 2 h or less. In January 2009, the American Society of Plastic Surgeons revised their position on fat grafting to the breasts, and cautioned: “results of fat transfer remain depen- 2 The Physiology of Fat Grafting: dent on a surgeon’s technique and expertise” [1]. The use of Current Theories fat grafting to the breast has demonstrated photographic evi- dence of volume maintenance [2]; however, there are cur- Like fibroblast survival in skin grafts, the classic “Diffusion/ rently no published data to evaluate this on an objective Angiogenesis” theory of fat grafting postulates adipocytes quantitative basis. In addition, the use of stem cell-enriched fat grafting sure in the recipient site is thought to interfere with diffusion, or fat grafting enriched with cell protectants has been sug- which leads to cellular death, apoptosis and loss of graft vol- gested to be beneficial to fat graft survival. Just like in a skin graft, early trauma or shearing of the The evolution of fat transfer to the breast follows two graft-recipient interface is thought to damage micro- merging parallel paths: (a) what we know about adipocyte angiogenesis and decrease graft survival. In the so-called Morrison theory, all or most of the transplanted adult adipo- cytes are destined to die, and act as a non-viable matrix or scaffold, through which macrophage penetrate and through which stem cell-mediated angiogenesis and adipogenesis D. The literature regarding the isolated An Overview effects of negative pressure suggests that adipocytes can be suctioned below 700 mmHg without undue trauma [8 ]. Four clinical categories appear to have significant weight on While a standard liposuction machine can generate up to the survival of grafted fat cells: 1 atmosphere (atm) (760 mmHg) of negative pressure, a 60 cc syringe connected to an in-line manometer can also 1. Animal studies have not demonstrated superior donor site fat based on anatomic location [9], and clinically we 3. What is more Although it has been reported in a histological study that important to consider is the relative abundance and require- larger cannula sizes (6 mm) harvest fat with better viability ments of donor graft in each individual case, and the surgical than with smaller cannulas [7], viability in this report was plan should aim to avoid or minimize donor site deformi- measured using cell isolation and counting adipocytes with a ties. Such an experimental endpoint only repre- in different body regions and also among different patients sents the first step of a multistage procedure which must con- may be a more important variable. Larger cells have a higher sider all stages, with the clinical endpoint being long-term (6 likelihood of mechanical cell membrane damage during months or greater) volume retention. Smaller cannula sizes theoretically create less donor site trauma and allow for removal of smaller sized lobules of fat, which may improve flow characteristics and reduce trauma during re-injection. An important consideration besides can- nula size is cannula hole size and number of holes. A 12-gauge cannula with 6–8 side holes 2×1 mm in size can extract a significant amount of fat despite its small calibre (Fig. The summation of the surface area of individual openings on a 12-gauge, 12-hole cannula approaches or exceeds the hole size of a classic 10 mm one-hole cannula once used in the 1980s, with much less donor area trauma. Further, each hole selects for lobules of uniform small size, which are more likely to flow easily through the injection cannula dur- Fig. Despite its is standardized, one cannot reliably measure the percent of widespread mention, there is a paucity of scientific data quanti- adipocyte volume that survived grafting.
Order ropinirole 0.25 mg free shipping
Activation sequence of ventricular tachycardia: endocardial and epicardial mapping studies in the human ventricle medications xyzal generic ropinirole 0.25 mg buy line. Endocardial mapping of ventricular tachycardia in the intact human ventricle: evidence for reentrant mechanisms symptoms yeast infection women order 0.5 mg ropinirole otc. Resetting of ventricular tachycardia: implications for localizing the area of slow conduction treatment neuropathy ropinirole 0.25 mg order line. Identification and catheter ablation of a zone of slow conduction in the reentrant circuit of ventricular tachycardia in humans. Electrogram patterns predicting successful catheter ablation of ventricular tachycardia. Identification of reentry circuit sites during catheter mapping and radiofrequency ablation of ventricular tachycardia late after myocardial infarction. Exploring postinfarction reentrant ventricular tachycardia with entrainment mapping. Nonsurgical transthoracic epicardial catheter ablation to treat recurrent ventricular tachycardia occurring late after myocardial infarction. Epicardial approach to the ablation of ventricular tachycardia in coronary artery disease: an alternative or ancillary approach. Reconstruction of endocardial potentials and activation sequences from intracavitary probe measurements. Simultaneous endocardial mapping in the human left ventricle using a noncontact catheter: comparison of contact and reconstructed electrograms during sinus rhythm. Characteristics of wavefront propagation in reentrant circuits causing human ventricular tachycardia. Fractionated endocardial electrograms are associated with slow conduction in humans: evidence from pace-mapping. The origin of premature ventricular complexes–role and limitations of the 12-lead electrocardiogram. Electrocardiographic localization of the site of origin of ventricular tachycardia in patients with prior myocardial infarction. Elimination of local abnormal ventricular activities: a new end point for substrate modification in patients with scar-related ventricular tachycardia. The substrate and ablation of ventricular tachycardia in patients with nonischemic cardiomyopathy. Catheter ablation of ventricular epicardial tissue: a comparison of standard and cooled-tip radiofrequency energy. Reversal of reentry and acceleration due to double-wave reentry: two mechanisms for failure to terminate tachycardias by rapid pacing. Clinical value of the postpacing interval for mapping of ventricular tachycardia in patients with prior myocardial infarction. Endo-epicardial homogenization of the scar versus limited substrate ablation for the treatment of electrical storms in patients with ischemic cardiomyopathy. Localizing the critical isthmus of postinfarct ventricular tachycardia: the value of pace-mapping during sinus rhythm. Electrophysiologic testing in the evaluation of patients with syncope of undetermined origin. Role of cardiac electrophysiologic studies in patients with unexplained recurrent syncope. Long-term follow-up of patients with recurrent unexplained syncope evaluated by electrophysiologic testing. Significance of inducible tachycardia in patients with syncope of unknown origin: a long-term follow-up. Electrophysiologic evaluation and follow-up characteristics of patients with recurrent unexplained syncope and presyncope. Electrophysiologic testing in patients with unexplained syncope: clinical and noninvasive predictors of outcome.
Cole, 47 years: Lateral torsoplasties are per- After years of depending on large-sized braided permanent formed either primarily or secondarily when dramatic improve- interrupted subcutaneous sutures, we changed to running ment in waistline concavity is desired (Fig. Generalized fatigue may be treated with energy A period of neurologic recovery followed by an interval conservation, weight loss programs and lower extremity (usually 15 years or more) of neurologic and functional orthoses. Instead of occurring in the sequence shown above (call it sequence number 1), three successes and two failures could occur in any one of the following additional sequences as well: Number Sequence 2 11100 3 10011 4 11010 5 11001 6 10101 7 01110 8 00111 9 01011 10 01101 4. Ecg criteria to identify epicardial ventricular tachycardia in nonischemic cardiomyopathy.
Osmund, 23 years: Pingueculum Dendritic Keratitis 801 It is somewhat raised mass on bulbar conjunctiva, usually Te branching tree-like lesion, due to herpes simplex virus, in interpalpebral region, representing elastic and hyaline is accompanied by conjunctivitis, pain, photophobia, tear- degenerative changes of the conjunctiva. The T-tube is cut to the appropriate size and inserted in the choledochotomy (Fig. Thus, dispatch must be involved in assessing and making deci- sions regarding any potential diversion. The other study [30] was limited to the effect of final urodynamic diagnosis on urine flow rates.
Ernesto, 45 years: Clinical Features Skin response to such a bacterial pathogen is dramatic in the Dandruf or seborrhea of the scalp is characterized by form of blisters. One of the better known kinase Numerous other structural components is fibrinolysin (streptokinase), which breaks are antiphagocytics. There is another mechanism, es (antigens), humoral immunity participates how antibodies play a role in causing cytol- in the mechanism of pathogenesis of imme- ysis of bacteria and multicellular parasites, diate hypersensitivity reaction and autoim- is by antibody-dependant cell-mediated mune diseases. In yet another situation, the posterior After the formation of matrix, it takes another 2 months teeth of the two jaws are together, but the mandibular for the commencement of calcifcation.
Cobryn, 36 years: In both models the possible inferential procedures and their underlying assumptions are discussed. This was achieved using a pair of elongated electrodes embedded within the absorbent layer of a diaper, which contained dry electrolytes. Sexual and organ function in patients with symptomatic prolapse: Are pessaries helpful? If it does not 800 subside spontaneously and is large enough, it should be defect (isolated or in association with aplasia of cranial excised.
Tarok, 43 years: Note the photophobia, lesions over extremities and hand and feet which are reddish and painful. Division of the hilar artery and vein is a critical step that should be performed meticulously and carefully to avoid any bleeding. In this study, 18 of the subjects completed a survey questionnaire assessing physical functioning at baseline, and after 1, 3, and 6 months. The mechanism in which metformin achieves increasing insulin sensitivity, rapamycin is a nontoxic and these effects is suggested to involve the enhancement of the well-tolerated drug that holds promise to antiaging.
Pedar, 27 years: We cannot seem to realize that breasts will sag over time or who reserve the choice for the circumareolar breast reduction for desire overly large breasts should be counseled with care and those patients whose sternal notch to nipple distance is no perhaps rejected until their expectations are more realistic. Oxygen delivery to tissues improves secondary to an increase in P-50 for hemoglobin (from 27 to 30 mm Hg) and cardiac output. Patients with a stable ground-level PaO2 of greater than 70 mmHg, or a stable oxygen saturation of greater than 94%, should not require in-fight medical oxygen therapy. If an overall significant difference is found, determine which pairs of individual sample means are significantly different.
Silas, 58 years: Women’s sexuality and sexual function are very complex issues, strongly modulated by psychosocial situation, and this necessitates a biopsychosocial approach for understanding the basis of dysfunction. In contrast, decreased density of caveolin-2 and caveolin-3 protein expression was noted in rat detrusor smooth cells from 12-month-old rats relative to 12-week-old rats [28]. A disadvantage of the range is the fact that it is computed from only two values, the largest and the smallest. If the shoulder dystocia persists, other maneuvers, such as delivering the posterior shoulder frst, episiotomy, or having the mother turn over on all fours, like she is about to crawl, may be attempted with the guidance of ground support.
Gambal, 22 years: Subgroup analysis showed some evidence of reduction in dyspareunia experienced by participants in the groups that had continuous suturing of all layers. Adjuvants are substances that An antigen may have one or more antigen- maintain the continuous stimulation of the ic determinants (a determinant is roughly immune responsive cells by slow release. If craniosynostosis is excluded, the parents should olemia and intravascular normovolemia or hypervolemia. Treatment results using pubovaginal slings in patients with large cystoceles and stress incontinence.
Derek, 42 years: The detrusor contraction strength varies neurogenically and myogenically, and can cause significant variability in urine flow rate measurements (Figure F. Te patient tends to forcibly hold the at least two of the following seven categories: eyes closed and seizure activity is bizarre. The ideal study would be a prospective randomized study, where both study arms employed the same surgical technique but differed only in their mode of abdominal access. Equipment costs account for a large part of the difference between open versus laparoscopic or robotic costs.
Mojok, 29 years: Biofeedback has been shown to be more effective than laxatives [93], relaxation training [89], and placebo [90]. If significant uterine/vault prolapse and/or anterior compartment (cystocele) defects are encountered, these typically should be repaired abdominally/laparoscopically/robotically prior to addressing the posterior compartment and the caliber of the vagina. The ischemia times (hours) for 11 subjects experiencing complete amputations were 4:67; 10:5; 2:0; 3:18; 4:00; 3:5; 3:33; 5:32; 2:0; 4:25; 6:0 For five victims of incomplete thumb amputation, the ischemia times were 3:0; 10:25; 1:5; 5:22; 5:0 Treat the two reported sets of data as sample data from the two populations as described. In this instance, ventricular tachycardia certainly does not require the bypass tract for its persistence.
Aidan, 30 years: Echocardiography shows a diminutive aorta and left ventricle with a poorly defned mitral valve in the presence of a normal and easily defnable tricuspid valve. Some end in the white pulp, supplying the germinal centers and mantle zones, but most empty into or near the marginal zones. This is thought mainly to be stress urinary incontinence in type, but detrusor overactivity must also play a role. Similarly, one can test a pump by measuring the time to deliver a known volume (e.
Oelk, 25 years: It is important to recognize that sedation of these patients might terminate the tachycardia. Another 9% was attributable to intravascular injection of a local anesthetic, most often after a negative aspiration test result during attempted caudal injection. A pediatrics patient that becomes suddenly ill may be exposing other passengers to the same ill- ness. In hypona- renal losses, extrarenal losses or nutritional defcits tremia accompanying hypoproteinemia, fuids must not Primary water excess with water gain be restricted.
8 of 10 - Review by J. Nasib
Votes: 301 votes
Total customer reviews: 301
References
- Prowle J. Fluid balance, creatinine kinetics and the diagnosis of AKI. doi:10.
- Kouroumalis E, Skordilis P, Thermos K,et al. Treatment of hepatocellular carcinoma with octreotide: a randomised controlled study. Gut. 1998;42:442-447.
- Gaither TW, Cooper CS, Kornberg Z, et al: Risk factors for the development of bladder and bowel dysfunction, Pediatrics 141(1):2018.
- Garcia JH, Cox JV, Hudgins WR. Ultrastructure of the microvasculature in experimental cerebral infarction. Arch Neuropathol (Berlin) 1971;18:273-85.