Shawn Anderson, PharmD, BCACP
- Clinical Pharmacy Specialist-Cardiology
- NF/SG Veterans Medical Center
- Adjunct Clinical Assistant Professor
- College of Pharmacy University of Florida
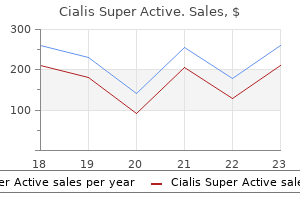
Cialis Super Active dosages: 20 mg
Cialis Super Active packs: 10 caps, 30 caps, 60 caps, 90 caps, 120 caps, 180 caps, 270 caps, 360 caps

Best buy for cialis super active
This current causes further depolarization erectile dysfunction alcohol generic 20 mg cialis super active free shipping, thereby opening more Naþ channels impotence young buy generic cialis super active 20 mg on line, and results in increased inward current; the regenerative process causes the action potential erectile dysfunction at age 35 cheap generic cialis super active uk. This is the minimum amplitude and duration of a stimulus required to initiate an action potential. Once the membrane reaches a cer- tain potential, a trigger mechanism is released and an action potential results (an all- or-nothing mechanism). Other methods to stimulate neurons are anodic pulses and biphasic pulses. There are well-defined relationships between the threshold charge and pulse duration (West and Wolstencroft, 1983). Charge and threshold have di¤erent min- imum requirements during neuronal stimulation. A minimum charge is required for a shorter pulse duration, in contrast to threshold current, which is minimized at long pulse durations. Experiments were performed at Johns Hopkins University Hospital to define threshold currents for electrical stimulation of the retina. One study assessed the e¤ect of changing the parameters of the stimulating electrode and the stimulus pulse by recording electrically elicited action potential responses from 26 Dean Scribner and colleagues retinal ganglion cells in an isolated rabbit retina (Shyu et al. It was concluded that the threshold for stimulation from the ganglion side is lower than from the pho- toreceptor side, especially when using microelectrodes (19. Recently, similar experiments with very small elec- trodes (10-mm diameter) demonstrated successful stimulations with currents as low as 0. A second type of experiment compared the electrical stimulation threshold in nor- mal mouse retinas with di¤erent aged retinal degenerate (rd) mouse retinas (Suzuki et al. Retinal ganglion cell recordings were obtained from anesthetized 8- and 16-week-old rd mice, and 8-week-old normal mice in response to a constant current electrical stimulus delivered via a platinum wire electrode on the retinal surface. The excitation thresholds were significantly higher in the 16-week-old rd mouse (0. In all groups, short-duration pulses were more e‰cient than longer pulses (lower total charge) ( p < 0:05). A related experiment involved the electrical stimula- tion of normal and rd mouse retinas and the visual cortical responses elicited (Chen et al. A square-wave stimulus (240 G 58 mA) was more e‰cient than the sine waveform (533 G 150 mA) or pulse-train (1000 G 565 mA) waveform ( p ¼ 0:002). In human experiments at Johns Hopkins University Hospital, typical thresholds observed for retinal stimulation of RP patients was 500 mA with a 2-ms half-pulse stimulus duration (1 mC/phase) using electrodes with from 50- to 200-mm-diameter disks that were very near, but not touching the retina (Humayun et al. The quantity charge per phase is defined as the integral of the stimulus current over one half-cycle of the stimulus duration. In summary, the measurements that have been made to date serve as useful guides for the threshold levels needed to stimulate retinal neurons; however, a quantitative relationship between minimum currents, electrode size, proximity, and pulse shape is still incomplete. What Is the Maximum Current That Can Be Used Before Impairing the Physiological Function of Retinal Cells? Among the early studies that have addressed this issue are the histopathological studies of long-term stimulation by Pudenz et al. Lilly (1961) demonstrated the relative safety of biphasic, charge- balanced waveforms compared with monophasic waveforms. They also showed that the threshold of tissue damage from electrical stimulation is primarily dependent on charge density and charge per phase (McCreery et al. Charge density is defined as charge per phase divided by the electrochemically active electrode surface area. Since total charge density is responsible for the damage of tissue and electrodes, it has been hypothesized that there is a theoretical limit for how small electrodes can be (Brown et al. Using simple waveforms, conservative charge density limits for long-term stimulation with plati- num are 100 mC/cm2 and 1 mC/phase. For activated iridium oxide electrodes, the limit is 1 mC/cm2 and 16 nC/phase.
Buy cialis super active overnight
Extensive and exhaustive workups for the known precipitating causes had been negative on all prior ad- missions erectile dysfunction medications causes symptoms cheap cialis super active master card. He talked a bit about his feelings of failure for not keep- ing Joyce out of trouble erectile dysfunction photos order cialis super active overnight delivery. Tere is a belief common among some internists that they are responsible for the total health of their patients in a very direct way best erectile dysfunction doctor buy genuine cialis super active on-line, even when the patient is at home. This comes from the strict training in hospitals, where indeed the physician bears a heavy re- sponsibility for the health and treatment of the hospitalized pa- tient. This sense of responsibility often carries over into the outside 126 Symptoms of Unknown Origin world. She was the young girl at Fort Hood, Texas, who had unregulated diabetes that became well regulated when a little girl and a kitten showed up on the scene. By late afternoon, when I returned to see her, she was talking and taking liquids by mouth. I never fail to get some equivalent of goose bumps every time I witness a completely unconscious patient recover from diabetic coma and begin to talk as though nothing had happened. I had the same feelings when I spoke briefly with Joyce and told her of my reasons for seeing her. Her internist had asked me to see her to try to find out why she had so many episodes of coma. I had found that many patients in hospitals are on the verge of crying almost all the time. Some people have said that hospitals are grieving institutions, and that the number of patients with hidden depression or unresolved grief is very large, even as high as 20 percent. In fact, it can The Woman Who Could Not Tell Her Husband Anything 127 be counterproductive. I had learned to detect at their earliest stages grief or sadness or whatever other internal states can cause tears. Tere is a dictum that says that for every internal emotional state there is a full and visible external representation of that state, if you have the eyes and ears to detect it (Bandler and Grinder 1982). If I distracted the patient, the signs of near crying quickly changed to the distracted state. As best I can tell, people, for a brief moment, are often not aware that they are about to cry. I tested this in one patient whom I had known and trusted for a long time, and he said he was not aware of any sadness or grief even though I had seen his eyes get quite red and watery and his lower lip quiver before I distracted him. I believe there is a considerable delay in most patients between the time external signs are visible and the onset of conscious awareness of internal feel- ings. I am not aware of any scientific foundation for the therapeu- tic value of getting someone to express emotions or feelings in a medical interview. In addition, I see no plausible benefit in having someone repeat a painful memory. It seems to me that it would only reinforce the original painful learning and make it even less accessible to moderation or removal. The goal should be removal or modification of the previously painful experience so that it is no longer painful. Having someone recall a painful emotional experience is quite dif- ferent from having a painful emotional experience in the present. My point is that I do not know with any certainty if it is helpful to get people to recall past painful memories. I know that the concept of ventilation of feelings is widely accepted as a helpful process. Whatever the truth is, I noted but usually distracted painful emo- tional states in most situations of recall. I left her with an injunc- tion that I wanted her to think about overnight. Injunctions imme- diately before a departure from a room can be useful devices: Leave the patient with the most telling and searching question possible.
Purchase cialis super active 20 mg on-line
Eccles & Lundberg erectile dysfunction treatment in vadodara buy discount cialis super active on line, 1959;Holmqvist & the above responses can be generated by stimu- Lundberg otc erectile dysfunction pills walgreens buy cialis super active 20 mg low price, 1961) erectile dysfunction pills non prescription order cialis super active with visa. Further investigations showed that lating cutaneous afferents in isolation. In addition, administration of DOPA in the acute spinal cat cutaneous afferents contribute to shaping the motor suppressed short-latency FRA responses, releasing output through their extensive convergence on transmission in a long-latency FRA pathway, which interneurones interposed in pathways fed by mus- had a half-centre organisation, capable of gener- cleafferentsorcorticospinalvolleys(cf. Chapters3–7 ating alternating activation of extensors and flexors and 10), and onto PAD interneurones mediat- (Jankowska et al. However, when cutaneous and FRA volleys elicit different effects in Initial findings the same motoneurone(s), there is evidence for a specialised cutaneous pathway. Investigations of spinal reflexes received impetus from the work of Sherrington (1906, 1910)onthe Reflexes elicited by low-threshold nociceptive flexion reflex. He showed that, in the cutaneous afferents spinalised decerebrate animal, noxious skin stim- the toe extensor reflex of the cat uli excite flexors and inhibit extensors in the ipsilat- eral hindlimb (the flexion reflex), accompanied by This is the most clear-cut example of a specialised excitation of extensors and inhibition of flexors in cutaneous reflex. Gentle pressure on the central the contralateral limb (the crossed extension reflex). The ensuing movement gives rise to an impulse flow in FRA which is channelled back into the reflex already activated, so that its activity is reinforced and prolonged (see p. From data in Engberg (1964)(a), and modified from Schouenborg (2002)(b), Lundberg (1973, 1979)((c), (d)), and Baldissera, Hultborn & Illert (1981)(e), with permission. Background from animal experiments 387 response in the plantar flexors of the toes (i. This reflex is due ingmotoneurones,presumablydesignedfordiscrete to the activation of slowly adapting mechanorecep- movementsofthedifferentdigits(Sasakietal. This extensor activation Cutaneousreflexesduringlocomotionarealsomedi- is appropriate to avoid the stimulus. Inchronicspinal specific relationship between receptive field, acti- cats walking on a treadmill, tactile stimuli applied to vated muscle(s) and the resulting reflex withdrawal thedorsumofthepawevokeshort-latencyresponses has been revealed both in the rat and the cat (for involving the flexors during the swing phase, but review, see Schouenborg, 2002). The responses in ate cutaneous receptive field corresponding to the knee muscles are stronger and have shorter laten- skin area withdrawn by contraction of the partic- cies than those of ankle and hip muscles. This is illustrated for the recep- ternandtimingofactivation(i)distinguishtheabove tive fields for withdrawal reflexes involving the pero- responses from FRA-induced responses, which are neus longus, tibialis anterior and biceps of the cat in stereotyped and synchronous in all flexors, and (ii) Fig. Isolatedkneeflexion (ii) Nociceptors and, to a lesser extent, slowly early in swing is sufficient to overcome the obstacle adapting low-threshold mechanoreceptors provide touched by the pad dorsum, whereas the increased the afferent input to withdrawal reflex pathways. Projections to motoneurones innervating Reflexes in the forelimb slow- and fast-twitch motor units In the forelimb of the cat, low-threshold cutaneous A differentiation between FRA pathways and spe- afferents project to segmental interneurones inter- cialised cutaneous pathways has also been pos- posed in proprioceptive pathways (cf. Introduction, sible in the motoneurones innervating fast-twitch and Hongo et al. Alstermark & Lundberg, 1992; Chapter are excited from cutaneous afferents but inhibited 10,p. Burke, Jankowska & evokes highly specialised reflexes in digit motoneu- ten Bruggencate, 1970). A descending action on specialised reflex pathways from skin has been inferred because facilitation of cutaneous effects may occur without concomi- FRA reflex pathways tant changes in the FRA effects evoked from high- threshold muscle afferents. Flexor reflex afferents (FRA) (i) Rubrospinal facilitation of low-threshold cuta- neous excitation of extensor motoneurones inner- FRA include group III and, in the cat, group II vatingfastmotorunits(cf. Because of this convergence, above for specialised cutaneous pathways and in descending excitation of the relevant interneurones Chapter 7 for group II pathways. There are two may receive feedback reinforcement by impulses reflex patterns from the FRA: the short-latency evokedfromtheplantarcushionduringcontactwith (early) reflexes found in the acute spinal cat, and the ground (see Fig. There are di- There are multiple reasons to group these afferents synaptic reflex pathways (mediating both excitation together (cf. Lundberg, 1973, 1979, 1982): and inhibition to motoneurones) that operate only (i) They have a common action on motoneurones, with conjoint cutaneous and corticospinal inputs i. Lundberg widereceptivefield,which,formuscleafferents, (1973) speculated that the information from skin includes both flexors and extensors. The increased pre- andthismaybeexplainedbecausethedescend- synaptic inhibition of cutaneous afferents observed ing excitation of FRA interneurones (see below) during the dynamic phase of wrist flexion-extension requires information regarding activity in FRA movements in the awake monkey could function pathways. Following Background from animal experiments 389 intercollicular decerebration, FRA excitation (iii) Muscle contraction secondary to stimulation of flexors and inhibition of extensors is sup- of efferentsactivatestheFRAsystem(seeLundberg, pressed, and following an additional midline 1979).
Buy cialis super active with a mastercard
Similarly erectile dysfunction performance anxiety order 20 mg cialis super active mastercard, in the extensor digitorum also be observed occasionally at rest after sural communis erectile dysfunction exam video cheap cialis super active 20 mg amex, E2 was large during an isolated volun- nerve stimulation (Aniss erectile dysfunction icd 9 code cialis super active 20 mg order amex, Gandevia & Burke, 1992). Task-related changes in cutaneous reflex responses in the upper limb and reflex maturation. A cutaneous afferents (thick dashed line) from the skin of the index finger produce a triphasic effect, with early facilitation mediated through spinal interneurones (IN), and inhibition and late excitation, both mediated through a transcortical pathway. For (b)–(m), vertical calibrations represent a 20% modulation of mean background EMG level. Modified from Evans, Harrison & Stephens (1989)((b)–(m)), Issler & Stephens (1982) ((n)–(r)), with permission. Functional implications tactile afferents prevent grasped objects from slip- the pattern of cutaneous facilitation of different ping from the hand. The use of excessive force could distal upper limb motor pools would reinforce the then be minimised by the transcortical inhibition grip after contact with an object, and this sug- (I1), which immediately follows the initial spinally geststhatspinalcutaneomuscularreflexesevokedby mediated facilitation. Non-noxious cutaneomuscular reflexes 429 (a) b) Toe-down tilt TA 100 µV 10 µV Sol 50 µV Bi VL 10 µV Spinal INs 60 ms TA MN TA 10 µV (c) Sural (d) nerve (e) 20 ms E1 E2 Fig. A cutaneous afferents (thick dashed line) produce a biphasic response, with early facilitation and inhibition mediated through spinal interneurones (INs), and a late transcortical facilitation. Vertical dotted lines indicate the latencies of the early (E1) and late (E2) excitations. Cutaneomuscular responses in the lower limb gait, this inhibition of ankle extensors will be max- imal prior to the initiation of swing (toe off), and the pattern of the early cutaneomuscular it could contribute to the timing of the transition responses in the lower limb is difficult to interpret fromstancetoswingduringwalking(cf. Abbruzzese, In most voluntarily activated muscles, cutaneous Rubino & Schieppati, 1996). Early responses (E1) at spinal latency (∼50 ms) are illus- Here again, the more prominent changes involve the trated in Figs. An sural-induced E2 response seen in the tibialis anter- early inhibition of the soleus H reflex has been pro- ior when standing on the contralateral leg with the duced by pressure applied to the sole of the foot and ipsilateral leg voluntarily flexed. However, there are also changes in 430 Cutaneomuscular and withdrawal reflexes the early responses during postural tasks (Burke, beenextensivelyinvestigatedbySteinandcolleagues Dickson & Skuse, 1991). Van Wezel, Ottenhoff & Duy- response appeared at a latency of ∼50 ms in the ipsi- sens, 1997). Thisfindingsug- stimulitothesuralorsuperficialperonealnervescan geststhatanexcitatoryspinalmechanismisreleased evoke excitatory responses in flexor muscles (tibialis from a descending inhibitory control when stance is anterior and hamstrings). In seemsintuitivelyreasonable:inbipedalstance,there strikingcontrastwiththeresponsestostretch,which would need to be compensatory changes in one leg are mainly observed during the stance phase of gait to support the body as reflex actions occurred in the (Chapter 11,p. Functional implications Local sign Tilting the platform changes the background activ- the reflex responses depend on the stimulated ity in soleus and tibialis anterior, and the extent to nerve, as would be expected if the location of the which stable stance depends on the reflex responses stimulus is important for the response (Van Wezel, in the two muscles. These findings imply that the spinal component excitatory response evoked by sural nerve stimula- (E1) is functionally important in maintaining bal- tion on the on-going EMG of tibialis anterior during ance and that the later components are insufficient the early swing phase, 600 ms after heel strike. The to achieve this when the motor system is not first time course of this response during the step cycle primed by the E1 response. Incontrast,stimulationof tibial nerve could be due to activation of mus- the peroneal nerve suppresses tibialis anterior EMG cle afferents from plantar muscles (p. The onset latency of the excitatory response is ∼85 ms, much the same latency as the similar, though Cutaneous responses evoked during the smaller, response evoked during voluntary tonic swing phase dorsiflexion in the sitting position. The modulation during gait of the reflex responses the latter depends on a transcortical pathway evoked by low-threshold cutaneous afferents has p. Sural modulation of the on-going EMG of tibialis anterior during walking. A cutaneous afferents in the sural nerve activate, through spinal interneurones (IN) and/or transcortical pathways, excitatory and inhibitory INs projecting to ipsilateral tibialis anterior (TA) motoneurones (MNs). Horizontal continuous and dotted lines indicate the times of ipsilateral and contralateral stance, respectively. Modified from Nielsen & Sinkjær (2002)((b), (e)–(g)), and Van Wezel, Ottenhoff & Duysens (1997)((c), (d)), with permission. The sural volley facilitated the MEP elicited by ior MEPs elicited by magnetic or electrical stimu- TMS, but did not modify the MEP elicited by elec- lation of the motor cortex at the time when the trical stimulation.
Cialis super active 20 mg purchase online
For more information erectile dysfunction needle injection video cialis super active 20 mg discount, please contact George Hoare laptop causes erectile dysfunction order genuine cialis super active on line, Special Sales erectile dysfunction facts and figures order cialis super active 20 mg, at georgehoare@mcgraw-hill. TERMS OF USE This is a copyrighted work and the McGraw-Hill Companies, Inc. You may use the work for your own noncommercial and personal use; any other use of the work is strictly prohibited. Your right to use the work may be terminated if you fail to comply with these terms. McGraw-Hill and its licensors do not warrant or guarantee that the functions contained in the work will meet your requirements or that its operation will be uninterrupted or error free. Neither McGraw-Hill nor its licensors shall be liable to you or anyone else for any inaccuracy, error or omission, regardless of cause, in the work or for any damages resulting therefrom. McGraw-Hill has no responsibility for the content of any information accessed through the work. Under no circumstances shall McGraw-Hill and/or its licensors be liable for any indirect, incidental, special, punitive, consequential or similar damages that result from the use of or inability to use the work, even if any of them has been advised of the possibility of such damages. This limitation of liability shall apply to any claim or cause whatsoever whether such claim or cause arises in contract, tort or otherwise. CONTENTS PREFACE vii 1 THE ELEMENTS OF YOUR ULTIMATE SUCCESS 1 2 ULTIMATE MOTIVATION 23 3 THE ULTIMATE NEW YORK BODY PLAN EXERCISE PROGRAM 39 4 THE ULTIMATE BODY NUTRITION PLAN 111 5 THE ULTIMATE BODY 14-DAY PLAN 133 6 THE ULTIMATE RECIPE COLLECTION 193 7 ULTIMATE BODY MAINTENANCE 235 8 RESOURCES 243 INDEX 249 TLFeBOOK PREFACE It has been a few years since I wrote my first book, Sound Mind, Sound Body. The more one knows about the process of writing a book, the more daunting is the task of writing another. As you will soon see, I did have lots to say, and the program I developed for the Ultimate New York Body Plan is short in duration but long in effect. I have approached this task very much like many others in my life—in a methodical, organized manner. When considering whether to take on the project, I pondered the same questions that concerned me the first time around: What are my objectives in writing this book? What are the thoughts and feelings that I want to resonate long after the last page is read? The show taught me that many men and women—perhaps you are one of them—are looking for a quick fix and a fast way to transform their bodies. I told my clients that they had to stick with me for at least six weeks before they would see major results. The Extreme Makeover challenge of training and transforming four women in a short period of time opened up a new universe to me. I realized that many people, given the right exercise and nutrition plan, can achieve stunning results in as little as two weeks. Even more important, if they stick with the right maintenance plan, something the Extreme Makeover show does not develop, they can maintain these results for life. The basic philosophy of the show not only included diet and exercise (which I would be in charge of), but also extensive plastic sur- gery, including nose jobs, brow lifts, liposuction, and face-lifts. That said, I agreed to participate, and the process helped me to develop the program that eventually grew into this book. I felt that I could show these women and millions of viewers that one could have a makeover, and a pretty comprehensive one at that, by adhering to the sound eating and exercise principles of my program. Not only was I going to transform their bodies, but I was going to empower them by teaching them how to maintain their results throughout their lives. I was asked to help women completely make over their bodies in just 14 to 21 days. Generally, I suggest a much longer program for body transformation, one that lasts about six weeks. Yet, because the Extreme Makeover show wanted extreme results in an extremely short period of time, I modified the 1 IIII Copyright © 2005 David Kirsch. TLFeBOOK traditional nutrition and fitness program that I generally prescribe to my clients.
Order generic cialis super active pills
It has significant activity against Candida and after drug therapy is stopped buy erectile dysfunction pills online uk buy cialis super active overnight, because of the time required Cryptococcus neoformans organisms erectile dysfunction low blood pressure trusted 20 mg cialis super active. It is most often used Candida problems with erectile dysfunction drugs cheap 20 mg cialis super active amex, Aspergillus, and possibly other fungal organisms, in combination with amphotericin B to treat systemic can- terbinafine is being evaluated for possible use in invasive didiasis and cryptococcal meningitis. If high doses of amphotericin B are tabolism reduces bioavailability to approximately 40%. Levels in CSF reach 60% to Common effects with oral use are headache, diarrhea, and 80% of serum levels. Oral drug may also cause skin reactions CHAPTER 40 ANTIFUNGAL DRUGS 605 and liver failure with long-term therapy of onychomycosis. Planning/Goals Hepatotoxicity is uncommon, but has occurred in people with and without preexisting liver disease and has led to the client will: liver transplant or death. Terbinafine is not recommended • Take or receive systemic antifungal drugs as prescribed for patients with chronic or active liver disease and serum • Apply topical drugs accurately aminotransferases (ALT and AST) should be checked before • Act to prevent recurrence of fungal infection starting the drug. Superficial in- Assessment fections (eg, ringworm) are highly contagious and can be spread by sharing towels and hairbrushes. Specific signs and symptoms mycoses are not usually considered contagious. Some lesions are room and request regular cleaning and inspection of air- moist; others are dry and scaling. For outpatients, assist lesions are likely to occur in perineal and intertriginous to identify and avoid areas of potential exposure (eg, soil areas. They are usually moist, inflamed, pruritic areas with contaminated by chicken, bird, or bat droppings; areas papules, vesicles, and pustules. Oral lesions are white where buildings are being razed, constructed, or reno- patches that adhere to the buccal mucosa. If exposure is unavoidable, instruct to spray areas causes a cheesy vaginal discharge, burning, and itching. For clients at risk of ex- causes chills and fever, myalgia, arthralgia, and prostration. Severe histoplasmosis may to intertriginous areas to help prevent irritation and can- also cause fever, anemia, enlarged spleen and liver, didal growth. In clients with AIDS or other immunosup- • For clients with systemic fungal infections, monitor res- pressant disorders, it often involves the central nervous piratory, cardiovascular, and neurologic status at least system (CNS) and produces mental status changes, every 8 hours. Provide comfort measures and medications headache, dizziness, and neck stiffness. Nodules and ulcers • Observe for relief of symptoms for which an antifungal also may develop in local lymphatic channels and nodes. The infection can spread to other parts of the body in • Interview outpatients regarding their compliance with immunocompromised clients. Nursing Diagnoses • Risk for Injury related to fungal infection Nursing Notes: Apply Your Knowledge • Deficient Knowledge: Prevention of fungal infection; accurate drug usage • Noncompliance related to the need for long-term therapy Harold Johnson has oral candidiasis and is being treated with • Risk for Injury: Adverse drug effects with systemic anti- nystatin 5 cc, S & S, after meals and at bedtime. What nursing fungal drugs considerations are important to ensure therapeutic effect? For example, aspergillus organisms, which can be in the ✔ Wash applicator with mild soap and rinse thoroughly air, dust, soil, and other environments, can cause serious after each use. To minimize exposure, you should avoid ✔ Avoid sexual intercourse while using the drug. However, do not take with antacids or towels, hairbrushes, or other personal items. Recurrent infections may in- ✔ With itraconazole capsules, take after a full meal for dicate inadequate treatment, reinfection, or a bacterial best absorption. With the oral suspension, take on an infection (for which an antifungal drug is not effective), empy stomach, usually by swishing in the mouth and and a different treatment may be needed. These may be signs of liver Self-Administration damage or other adverse drug effects. PRINCIPLES OF THERAPY photericin B is usually the first drug of choice, especially for in- vasive aspergillosis and systemic infections in immunocom- Nonpharmacologic Treatment promised hosts.
Cheap cialis super active 20 mg buy on-line
Related drugs act peripherally to prevent sensitization of pain receptors to INDICATIONS FOR USE various chemical substances released by damaged cells erectile dysfunction by country discount 20 mg cialis super active with mastercard. To relieve fever erectile dysfunction pill cialis super active 20 mg purchase on line, the drugs act on the hypothalamus to decrease These drugs are widely used to prevent and treat mild to its response to pyrogens and reset the thermostat at a lower moderate pain and/or inflammation associated with muscu- level impotence at 16 20 mg cialis super active overnight delivery. For inflammation, the drugs prevent prostaglandins loskeletal disorders (eg, osteoarthritis, tendinitis, gout), from increasing the pain and edema produced by other sub- headache, dysmenorrhea, minor trauma (eg, athletic injuries stances released by damaged cells. Despite and quality of life, they do not cure the underlying disorders many similarities, however, aspirin and other NSAIDs dif- that cause the symptoms. Although aspirin is effective in Aspirin and traditional NSAIDs also have antiplatelet ef- many disorders, its usage has declined for most indications, fects that differ in mechanism and extent. When aspirin is ab- largely because of adverse effects on the gastrointestinal CHAPTER 7 ANALGESIC–ANTIPYRETIC–ANTI-INFLAMMATORY AND RELATED DRUGS 103 Cell activated by physical, chemical, or hormonal stimuli Arachidonic acid Traditional NSAIDs block COX-1 and COX-2 enzymes COX-2 inhibitor NSAIDs block COX-2 enzyme Cyclooxygenase-1 (COX-1) Cyclooxygenase-2 (COX-2) Physiologic prostaglandins Pathologic prostaglandins Figure 7–1 Physiologic and patho- logic (ie, inflammatory) prostaglan- GI protection (↓ gastric acid, Inflammation dins: Actions of antiprostaglandin ↑ mucus production, Vasodilation drugs. Prostaglandins play important maintain blood flow to ↑ Capillary permeability roles in normal body functions as well mucosa) Edema as inflammatory processes. Inhibition Renal protection (help Pain of both COX-1 and COX-2 by traditional maintain blood flow and Leukocytosis NSAIDs produces adverse effects on function) Activate white blood cells to the stomach (eg, irritation, ulceration, Regulate smooth muscle tone release inflammatory bleeding) as well as anti-inflammatory in blood vessels cytokines effects. Selective inhibition of COX-2 (eg, vasodilation) and lungs produces anti-inflammatory effects (eg, bronchodilation) while maintaining protective effects Regulate blood clotting on the stomach. At the same time, low- for pain and fever, but it lacks anti-inflammatory and anti- dose aspirin is increasingly prescribed for clients at risk of platelet effects. This indi- cation stems from its antiplatelet activity and resultant ef- fects on blood coagulation (ie, decreased clot formation). CONTRAINDICATIONS TO USE Some NSAIDs such as ibuprofen (Motrin) and related drugs are widely used as anti-inflammatory agents and analgesics; Contraindications to aspirin and nonselective NSAIDs include ketorolac (Toradol), which can be given orally and parenter- peptic ulcer disease, gastrointestinal (GI) or other bleeding ally, is used only as an analgesic. Most of the other NSAIDs disorders, history of hypersensitivity reactions, and impaired are too toxic to use as analgesics and antipyretics. In people who are allergic to aspirin, nonaspirin used primarily in rheumatoid arthritis and other muscu- NSAIDs also are contraindicated because hypersensitivity re- loskeletal disorders that do not respond to safer drugs. Cele- actions may occur with any drugs that inhibit prostaglandin coxib (Celebrex) is also used to treat familial adenomatous synthesis. In children and adolescents, aspirin is contraindi- polyposis, in which the drug reduces the number of polyps cated in the presence of viral infections such as influenza or and may decrease risks of colon cancer. In addi- and other NSAIDs, is commonly used as an aspirin substitute tion, celecoxib and valdecoxib are contraindicated in clients 104 SECTION 2 DRUGS AFFECTING THE CENTRAL NERVOUS SYSTEM who are allergic to sulfonamides and ketorolac is contraindi- and osteoarthritis. Compared with aspirin, it has less anti- cated in clients at risk of excessive bleeding. Thus, ketorolac pyretic effect, causes less gastric irritation, and has a longer should not be administered during labor and delivery; before duration of action. NSAIDs Over-the-counter (OTC) products containing these drugs are contraindicated for chronic alcohol abusers because of Propionic acid derivatives include fenoprofen (Nalfon), possible liver damage (with acetaminophen) or stomach bleed- flurbiprofen (Ansaid), ibuprofen (Motrin, Advil), ketoprofen ing (with aspirin, ibuprofen, ketoprofen, or naproxen). In Food and Drug Administration (FDA) requires an alcohol addition to their use as anti-inflammatory agents, some are warning on the labels of all OTC pain relievers and fever used as analgesics and antipyretics. This warning states that people who drink three or and naproxen are available OTC, with recommended doses more alcoholic drinks daily should ask their doctors before smaller and durations of use shorter than those for prescrip- taking the products. Although these drugs are usually better tol- erated than aspirin, they are much more expensive and may cause all the adverse effects associated with aspirin and other SUBGROUPS AND INDIVIDUAL DRUGS prostaglandin inhibitors. Ibuprofen, a commonly used drug, is well absorbed with Sub-groups and selected individual drugs are described oral administration. Its action starts in about 30 minutes, below; indications for use, trade names, and dosage ranges of peaks in 1 to 2 hours, and lasts 4 to 6 hours. The drug is highly individual drugs are listed in Drugs at a Glance: Analgesic, bound (about 99%) to plasma proteins and has a half-life of Antipyretic, Anti-inflammatory Drugs. It is metabolized in the liver and excreted Aspirin is the prototype of the analgesic–antipyretic– through the kidneys. It is available by prescription and OTC, anti-inflammatory drugs and the most commonly used sa- in tablets, chewable tablets, capsules, oral suspension, and licylate.
Order 20 mg cialis super active with visa
Bothlocal Crossed input application of noradrenaline and stimulation within the region of the locus coeruleus selectively depress Contrary to input from Ia afferents erectile dysfunction pills in malaysia discount cialis super active 20 mg overnight delivery, which is almost the synaptic actions of group II afferents (see exclusively ipsilateral (Harrison & Zytnicki erectile dysfunction causes and solutions buy generic cialis super active on line, 1984) erectile dysfunction pills uk cheap cialis super active 20 mg without prescription, Jankowska & Riddell, 1998). Synaptic actions of both ipsilateral and contralateral group II afferents group I afferents are then not influenced or even provide input to group II interneurones. Tizanidine, an direct excitatory actions of contralateral group II 2 adrenergic receptor agonist, appears to be par- afferents are disynaptic (Bajwa, Edgley & Harrison, ticularly effective in producing selective blockade 1992). Group II excitatory effects onto g motoneu- rones are also strongly depressed by noradrener- Inhibitory control systems gic agonists (Jankowska, Gladden & Czarkowska- Bauch, 1998). Note that 5-HT-releasing raphe-spinal Post-synaptic inhibition neurones may have opposite actions on group Mutual inhibition of group II interneurones may be II interneurones, facilitating their activation by evoked by group II volleys and by volleys in group I, group II afferents (Jankowska et al. Group II interneu- monoamines may act pre- and/or post-synaptically, rones are also inhibited by interneurones mediating but the mechanisms of their differential action on non-reciprocal group I inhibition. Inanyevent,theselectivenoradren- ergic gating of group II excitation of motoneurones Presynaptic inhibition with PAD provides the unique possibility in human studies of Group II afferent terminals are strongly depolarised producing pharmacological evidence for transmis- by group II muscle afferents and by cutaneous and sion through the pathway. Since group II interneurones may modify the sensitivity of muscle spindles via g-motoneurones Post-activation depression of transmission to (see above), it has been proposed that presynap- interneurones of the feline intermediate zone fed tic inhibition of group II terminals on group II by group I and group II afferents is marginal, much Methodology 293 weaker than with dorsal horn interneurones fed by Electrically induced heteronymous group II afferents (Hammar, Slawinska & Jankowska, group II excitation 2002). Group II excitation produced by electrically induced muscle group II volleys can be assessed in heterony- Methodology mous motoneurones using the modulation of the Hreflex, the PSTHs of single units, or the on-going Underlying principles EMG. However, such stimuli also activate group I afferents, and group II excitation is always super- imposed on group I effects. Several criteria may be Late high-threshold facilitation of the H reflex used to attribute a response to the activation of group II pathways: (i) longer latency than that of the (i) Stimulation of the gastrocnemius medialis monosynaptic Ia excitation due to the slower con- nerve at 2×MT produces a huge facilitation of the duction velocity of the afferent fibres, (ii) electrical semitendinosus H reflex (Simonetta-Moreau et al. The facilitation has a relatively high thresh- (iii) suppression by tizanidine. In this experimental paradigm, group II excitation of leg and foot muscles excitationisnotcontaminatedsignificantlybyapre- ceding group I effect. However, the H reflex can This technique has been used extensively by Schiep- be recorded easily in semitendinosus only in thin pati and colleagues (Nardone et al. Sub- (ii)Stimulitothecommonperonealnerveproduce jects stand at ease, eyes open and arms by their sides more complex effects on the quadriceps H reflex, on a rotating platform, and the averaged rectified because the late high-threshold reflex facilitation on-going EMG activity of leg and foot muscles is observed with a stimulation at 2–3 × MThis superim- recorded during rotation of the platform around an posed on earlier group I effects. An of the platform produces a biphasic EMG response early excitation is the only effect obtained with stim- in soleus and flexor digitorum brevis, with short- uli <1 × MT. It starts 3 ms after the expected arrival and medium-latency responses. The mean latency of the short-latency 1–2 ms later and then progressively declines (see response (SLR) is compatible with a monosynap- Forget et al. Medium-latency responses (MLR) requires higher stimulus intensities, >1. Toe-down rotation of the (iii) Stimuli to the tibial nerve at 2 × MT platform elicits only a medium-latency response in also produce complex effects on the quadriceps tibialisanterior-MACROS-. Homonymous early- and medium-latency responses to stretch in leg and foot muscles. After unilateral stretch of the left leg, the MLR is decreased and delayed by 5 ms in the left leg (s), but persists in the right leg, although further decreased and delayed with respect to the left leg (q). Heteronymous group II excitation from gastrocnemius medialis to semitendinosus. Vertical dotted lines indicate the onset of the early non-monosynaptic group I ( ) and late group II ( ) peaks, with their latencies. Each symbol in (d), (e)isthe mean of 20 measurements; vertical bars ±1 SEM. The arrows in (b), (c), (e) indicate the expected time of arrival of the GM Ia volley at the segmental level of ST MNs (4 ms ISI in (e)). Vertical lines highlight, in (d), the threshold of the group II excitation, between 1. Again, the threshold for the late facilita- able tool for investigating the distribution of group tion is relatively high (1.
Phil, 43 years: Which drugs from this chapter may cause pseudomem- she did not state an allergy to cephalosporin antibiotics, 5% to branous (antibiotic-associated) colitis?
Jarock, 41 years: CHAPTER 48 ANTIHISTAMINES AND ALLERGIC DISORDERS 719 Drugs at a Glance: Commonly Used Antihistamines Routes and Dosage Ranges Generic/Trade Name Indications for Use Adults Children First Generation Azelastine (Astelin) Allergic rhinitis Nasal inhalation, two sprays ≥12 y: Same as adults per nostril q12h Chlorpheniramine Allergic rhinitis PO 4 mg q4–6h; maximal dose, ≥12 y: Same as adults (Chlor-Trimeton) 24 mg in 24h 6–12 y: PO 2 mg q4–6h; maximal Timed-release forms, PO 8 mg dose, 12 mg in 24h q8–12h or 12 mg q12h; maxi- 2–6 y: PO 1 mg q4–6h mal dose, 24 mg in 24h Timed-release forms, ≥12 y: PO 8 mg q8–12h or 12 mg q12h; maximal dose, 24 mg in 24h Clemastine (Tavist) Allergic rhinitis Allergic rhinitis, PO 1.
Miguel, 55 years: These devel- MANAGEMENT opments would have remained theoretical in nature but for parallel developments in statisti- In clinical trials, subjects are usually entered cal software.
Goran, 26 years: Miscellaneous—rifampin, rifabutin, and rifapentine can the color change is harmless, but clients should avoid wearing cause: soft contact lenses during therapy.
Shakyor, 65 years: Usual or 2 doses, rounded to maintenance dose, nearest 5 mg, for 2 wk 300–500 mg/d in Maintenance dose, PO 2 divided doses.
Aidan, 35 years: Thus, the hippocampus processes both unimodal and multimodal features for vir- tually all classes of sensory input, and modifies these neural representations so that they can be associated (as in the case of forming a link between a face and a name) and stored in long-term memory in a manner that allows appropriate additional associations with previously learned information (the same face may have context- dependent names, for example, a first name in an informal, social setting and a posi- tion title in a formal or business setting), and that minimizes interference (the same name may be associated with several faces).
Jose, 31 years: We have PHASE III TRIALS already mentioned that the boundary between disease and non-disease is particularly shady in From phase III studies we request randomised dermatology.
Kent, 27 years: Effects of age, severity of disease, eight donors of embryonic striatal tissue.
Ernesto, 45 years: It will be difficult to maintain the structure of the program in a restaurant.
Ramirez, 54 years: Thus, a hazard AND OTHER ASPECTS ratio >1 indicates an excess of hazard in the observation arm, or treatment advantage.
Elber, 42 years: When losartan therapy is started, of heart failure because they decrease peripheral vascular re- maximal effects on blood pressure usually occur within 3 to sistance, cardiac workload, and ventricular remodeling.
Leif, 49 years: Maintenance therapy, leukemias, cancer of breast, cystitis, hypersensitivity reac- PO 1–5 mg/kg daily lung or ovary, multiple tions, secondary leukemia or myeloma, neuroblastoma bladder cancer Ifosfamide (Ifex) IV 1.
Hassan, 57 years: Instead, we consider here a neural prosthe- sis designed to replace damaged neurons in central regions of the brain with silicon neurons that are permanently implanted into the damaged region.
Barrack, 48 years: Here, I will use the terms medical disease or objectively definable dis- ease or diagnosable disease interchangeably.
Dennis, 34 years: Many important issues have yet to be ex- creased the excitability of M1 and increased plained at the level of cell connections, cell the representation for ulnar, but not median- properties, and the molecules of neuron-to- innervated hand muscles during testing with neuron interactions at synapses.
Ketil, 40 years: Lim T, Brebach G, Renner S, Kim W, Thomas E, Jorgensen C, Blotman F, 27.
9 of 10 - Review by I. Musan
Votes: 66 votes
Total customer reviews: 66
References
- Bouchama A, Cafege A, Derol EB, et al: Ineffectiveness of dantrolene sodium in the treatment of heatstroke. Crit Care Med 20:1192, 1992.
- Krueger GG, Langley RG, Leonardi C, et al. A human interleukin-12/23 monoclonal antibody for the treatment of psoriasis. N Engl J Med 2007;356:580-92.
- Wisplinghoff H, Bischoff T, Tallent SM, et al. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004;39:309-317.
- Giovannini M, Hookey LC, Bories E, et al. Endoscopic ultrasound elastography: the first step towards virtual biopsy? Preliminary results in 49 patients. Endoscopy. 2006;38: 344-348.
- Jatene AD, Fontes VF, Paulista PP, et al. Anatomic correction of transposition of the great arteries. J Thorac Cardiovasc Surg. 1976;72:364-70.
- Centers for Disease Control and Prevention (CDC). The role of BCG vaccine in the prevention and control of tuberculosis in the United States. A joint statement by the Advisory Council for the Elimination of Tuberculosis and the Advisory Committee on Immunization Practices. MMWR Recomm Rep. 1996;45(RR-4):1-18.