Adrian S. Woolf, MD
- Professor of Nephrology and Head of Nephro-Urology Unit,
- Institute of Child Health, University College London,
- Great Ormond Street Hospital for Children, London, United Kingdom
Atorlip-10 dosages: 10 mg
Atorlip-10 packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

10 mg atorlip-10 with mastercard
Early enteral nutrition improves outcomes of open abdo- men in gastrointestinal fstula patients complicated with severe sepsis cholesterol test need to fast order atorlip-10 10 mg with mastercard. Effect of immediate enteral feeding on trauma patients with an open abdomen: protection from nosocomial infections high cholesterol medication erectile dysfunction atorlip-10 10 mg purchase line. Is it feasible to implement enteral nutrition in patients with enteroatmospheric fstulae? Metabolic and nutritional support of the enterocutaneous fstula patient: a three-phase approach cholesterol test dubai cheap atorlip-10 online mastercard. Early enteral nutrition after abdominal trauma: effects on septic morbidity and practicality. Effcacy and safety of active negative pressure peritoneal therapy for reducing the systemic infammatory response after damage control laparotomy (the intra-peritoneal vacuum trial): study protocol for a randomized con- trolled trial. Systematic review and evidence based recommendations for the use of negative pressure wound therapy in the open abdomen. Systematic review and meta-analysis of the open abdomen and temporary abdominal closure techniques in non-trauma patients. High risk of fstula formation in vacuum-assisted clo- sure therapy in patients with open abdomen due to secondary peritonitis-a retrospective analy- sis. Long-term vacuum-assisted closure in open abdomen due to secondary peritonitis: a retrospective evaluation of a selected group of patients. Independent predictors of enteric fstula and abdominal sepsis after damage control laparotomy: results from the prospective aast open abdomen registry. What is the effectiveness of the negative pressure wound therapy (Npwt) in patients treated with open abdomen technique? Systematic review and meta-analysis of the role of somatostatin and its analogues in the treatment of enterocutaneous fstula. Open abdomen treatment for septic patients with gastrointestinal fstula: from fstula control to defnitive closure. Negative pressure wound therapy man- agement of the “open abdomen” following trauma: a prospective study and systematic review. Temporary closure of open abdominal wounds by the modifed sandwich-vacuum pack technique. A novel approach to the problem of intestinal fstulization arising in patients managed with open peritoneal cavities. Biological dressings for the management of enteric fstulas in the open abdomen: a preliminary report. The foating stoma: a new technique for control- ling exposed fstulae in abdominal trauma. The “Fistula Vac” a technique for management of enterocutaneous fstulae arising within the open abdomen: report of 5 cases. D’hondt M, Devriendt D, Van Rooy F, Vansteenkiste F, D’hoore A, Penninckx F, Miserez M. Treatment of small-bowel fstulae in the open abdomen with topical negative-pressure therapy. A modifed “Fistula-Vac” tech- nique: management of multiple enterocutaneous fstulas in the open abdomen. The use of negative-pressure wound therapy to manage enteroatmo- spheric fstulae in two patients with large abdominal wounds. Vacuum assisted closure (Vac) therapy(Tm) as a swiss knife multi-tool for enteric fstula closure: tips and tricks: a pilot study. Open abdomen with concomitant enteroatmospheric fstula: validation, refnements, and adjuncts to a novel approach. Collapsible enteroatmospheric fstula isolation device: a novel, simple solution to a com- plex problem. Single-stage closure of enterocutaneous fstula and stomas in the presence of large abdominal wall defects using the components sepa- ration technique. A novel method for managing enterocutaneous fstu- lae in the open abdomen using a pedicle fap. A new technique of closing a gastroatmospheric fstula with a rectus abdominis muscle fap. Autologous reconstruction of massive enteroatmospheric fstulation with a pedicled sub- total lateral thigh fap. Di Saverio S, Tarasconi A, Inaba K, Navsaria P, Coccolini F, Costa Navarro D, Mandrioli M, Vassiliu P, Jovine E, Catena F, Tugnoli G.
Discount atorlip-10 10 mg overnight delivery
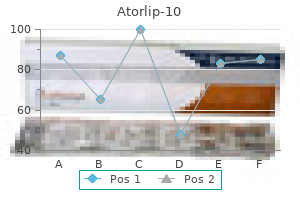
Tis microinvasive approach provides several advantages over the techniques currently used test je cholesterol buy atorlip-10 10 mg with mastercard. In this phase percentage of cases cholesterol medication statin buy atorlip-10 10 mg otc, near 50% cholesterol levels of athletes trusted 10 mg atorlip-10, while chronic stabilization is obtained, with cardiac function cardiomyopathies do not. In view of the absence of reasonable chances of recovery, and of the constantly 8. J Heart Lung Transplant 34(12):1495–1504 T10 has been overcome by the introduction of the 3. Patients whose ventricular function is deemed dysfunction or intractable ventricular arrhyth unrecoverable or unlikely to recover without mias). A heart that is unable to eject adequately long-term device support ofen leads to ventricular distension and B. Patients who are deemed too ill to maintain stagnation of blood inside the cardiac chambers, normal hemodynamics and vital organ function pulmonary vasculature, and aortic root. Some of the more common options considered to allow for proper assessment of the include both percutaneous and surgical neurologic status of the patient. Impella (Abiomed) is another extracorporeal device used for partial circulatory support and for determining intravascular pressure. Benefts include reducing enddia Myocardial stunning following acute ischemia stolic volume and pressure, mechanical work, and reperfusion myocardial wall tension, oxygen demand, and Postcardiotomy overall cardiac output. Te pumps are available in fve beneft, but randomized prospective studies show sizes based on stroke volume (10, 25, 30, 50, and no beneft between devices. Results has excellent reliability and a low risk of highlighted a reduction of lactate levels, suggesting thrombosis. Devices may be considered consistent with a low-output state when oxygenation remains impaired or for failure to wean of cardiopulmonary bypass. Pulmonary artery pressure was subsequently stable, but wedge Our patient had advanced endstage heart pressure went up, indicating a reduction in failure complicated by renal failure due to pulmonary vascular resistance. Pulmonary cardiorenal syndrome with an acute kidney saturation did increase with the nitroprusside, injury. With the degree of rightsided heart failure suggesting a signifcant improvement in forward and severe pulmonary hypertension, she initially fow with vasodilatation (see. However, she did tolerate a high dose of et al (2005) Randomized comparison of intra-aortic balloon support with a percutaneous left ventricular nitroprusside suggesting she might beneft from assist device in patients with revascularized acute further aferload reduction. She continued on myocardial infarction complicated by cardiogenic elevated doses of both hydralazine and isosorbide shock. Seyfarth M, Sibbing D, Bauer I, Frohlich G, Bott-Flugel L In the interim, we considered shortterm (2008) A randomized clinical trial to evaluate safety and efcacy of a percutaneous left ventricular assist solutions to allow time for improved hepatorenal device versus intra-aortic balloon pump for treatment function in the setting of cardiogenic shock. J Thorac Cardiovasc Surg 141(4): stable with improved renal and hepatic function (see 932–939. Cheng J, den Uil C, Hoeks S, van der Ent M, Jewbali L References et al (2009) Percutaneous left ventricular assist devices vs intra-aortic balloon pump counterpulsation for 1. At the frst decompensated cardiac myopathy, postcar- encounter for patients with cardiogenic shock, diotomy shock, and fulminant myocarditis. Moreover, these patients always restore hemodynamic instability and end-organ receive antiplatelet therapy before and afer percu- function and may improve outcomes following taneous coronary intervention or other causes. In this report, despite optimal medical therapy, bridge-to-deci- the 90-day mortality was 6. Tese patients ofen Considering these results, one-stage durable have simultaneous hepatic dysfunction. Patients with severe acute pulmonary injury, simultaneous in cardiogenic shock ofen show some degree of implantation of a temporary right ventricular biventricular dysfunction. Lorusso R, Centofanti P, Gelsomino S, Barili F, Di membrane oxygenator support for right ventricular Mauro M, Orlando P et al (2015) Venoarterial failure following implantable left ventricular assist extracorporeal membrane oxygenation for acute device placement. Eur J Cardiothorac Surg 49: fulminant myocarditis in adult patients: a 5-year multi- 73–77 institutional experience. J Am Coll Cardiol circulatory support for fulminant myocarditis 61(3):313–321 complicated by cardiogenic shock.
Diseases
- Kikuchi disease
- Pachygyria
- Apudoma
- Keratolytic winter erythema
- Popliteal pterygium syndrome lethal type
- Weissenbacher Zweymuller syndrome
- Exotropia
- Schizophrenia, paranoid type
10 mg atorlip-10 order mastercard
In the 1990s in the past decade cholesterol shrimp squid atorlip-10 10 mg buy amex, it has become evident that the same peri- and early in the 2000s cholesterol test boston atorlip-10 10 mg visa, many of the studies on peri-implantitis odontal disease processes that afect teeth afect dental were done in the canine model using ligature-induced peri- implants cholesterol lowering supplement buy cheap atorlip-10 line. Clinically it It has been shown that reosseointegration can occur on a is present when three conditions are seen: radiographic evi- repaired surface. Protocols for regenerative procedures are evolving; they suppuration on probing (Figure 25-1, A and B). Success rates vary, depending on 4 of implant sites may develop peri-implant mucositis. Peri- the anatomy and amount of preexisting bone loss, but typi- 11,12 implant mucositis typically is treated nonsurgically, with cally are in the 60% to 70% range. Most studies also weeks or months after crown cementation, surgical explora- conclude that smoking and a history of periodontitis tion for retained cement is indicated (Figure 25-2). Another common cause is periodontally compromised 16 teeth elsewhere in the mouth. Studies have shown that pocket depths of 6 mm or more around teeth cause the seeding of implants with periodontal pathogens; peri- implantitis presents itself with a lag time of approximately 2 17 to 3 years after pocket development. Considerable research is under way regarding a genetic component underlying the 18 individual susceptibility to implant loss. Te interleukin-1 and interleukin-6 genes have been studied and may ofer an explanation for the clusterization phenomenon, in which certain individuals appear to be susceptible to chronic peri- odontitis and peri-implantitis, resulting in an increased inci- dence of implant loss. Other common causative factors include a poor prosthesis design that inhibits hygiene, inadequate attached tissue, endodontic defects on adjacent teeth, and systemic issues, 20 such as smoking and diabetes. It is interesting to note that when Brånemark and col- A leagues originally presented their 15-year success rates, their long-term success rates were high, and peri-implantitis was not a major problem in their patient population. Tis is likely due to the fact that the vast majority of their original patients were edentulous and had screw-retained prostheses. Teir protocol thereby eliminated the two most common causes of peri-implantitis: retained cement and periodontal pathogens associated with periodontally compromised natural teeth. Prevention of peri-implantitis starts with proper implant site development, obtaining optimized bone and soft tissue, and subsequent ideal implant placement. Prevention of peri- odontal disease elsewhere in the mouth, proper prosthesis design for adequate hygiene, prevention of retained cement, and regular hygiene recall for early detection of peri- implantitis are all necessary to minimize peri-implant disease. Indications for the Use of the Procedure B Once the diagnosis of infammation with bone loss has been Figure 25-4 A and B, Four-wall crater defect of peri-implantitis. Unlike teeth, when implants are removed, they typically leave a sizable defect that does not have four walls. Limitations and Contraindications Te resultant osseous regeneration often is minimal and typi- cally requires aggressive bone grafting to regenerate the site Te treatment and resolution of the infammation associated for a new implant. For this reason, undergoing an implant with peri-implant disease often result in some degree of salvage procedure is often in the patient’s best interest. Tis becomes a major concern in the Typically, osseous defects of 5 to 6 mm or less vertically esthetic zone, where just a slight amount of gingival recession along the implant are amenable to treatment. In these esthetically may be treated if the implants are critical in support of the demanding situations, the best treatment results esthetically prosthesis and removal may result in complete loss of a sig- and functionally are obtained when the prosthesis is removed, nifcant prosthesis. In the case illustrated in Figure 25-3, cover screws are placed, and treatment is performed 8 to 10 implant #10 was vital to the prosthesis, and a repair was weeks later. Tis may leave the patient in provisional pros- carried out, despite greater than 50% bone loss. For this reason, prevention of treatable defects appear to be the circumferential crater type peri-implant disease in the frst place, of course, is ideal, but lesions caused by retained cement, which closely resemble a when it occurs, treatment should be initiated as soon as the three- or four-wall periodontal defect (Figure 25-4). However, as a around the implant or if the implant is mobile, the implant patient’s age and peri-implant disease advance, these rough- should be removed. Typically, when bone loss approaches ened surfaces and screw threads become exposed, either 50% of the implant length, implant removal should be seri- within the pocket or visibly. Exceptions can be made if the implant is a removing the adherent bacterial plaque and bioflm. Te infammation associated with peri-implantitis causes Te cause of the peri-implantitis also needs to be addressed a secondary loss of attached tissue. If the cause is a poorly designed implantitis has been left untreated for extended periods, the prosthesis that results in inability to clean it, the prosthesis attached tissue is completely lost due to infammation. If the cause is bacterial seeding from adequate band of keratinized tissue is necessary for long-term periodontally involved teeth elsewhere in the mouth, these maintenance of peri-implant health.
Trusted 10 mg atorlip-10
The in vitro mechanisms and in vivo efficacy of intravenous lidocaine on the neuroinflammatory response in acute and chronic pain definition of cholesterol crystal atorlip-10 10 mg mastercard. Peri-operative intravenous administration of magnesium sulphate and postoperative pain: a meta-analysis cholesterol test canada purchase atorlip-10 10 mg free shipping. Perioperative systemic magnesium to minimize postoperative pain: a meta-analysis of randomized controlled trials cholesterol medication with alcohol order atorlip-10 10 mg online. Ketamine and magnesium association reduces morphine consumption after scoliosis surgery: prospective randomised double-blind study. The preoperative use of gabapentin, dexamethasone, and their combination in varicocele surgery: A randomized controlled trial. Perioperative single dose systemic dexamethasone for postoperative pain: a meta-analysis of randomized controlled trials. Research priorities regarding multimodal peripheral nerve blocks for postoperative analgesia and anesthesia based on hospital quality data extracted from over 1,300 cases (2011–2014). Effect of perioperative systemic alpha2 agonists on postoperative morphine consumption and pain intensity: systematic review and meta-analysis of randomized controlled trials. Epidural, cerebrospinal fluid, and plasma pharmacokinetics of epidural opioids (part 1): differences among opioids. Small dose of clonidine mixed with low-dose ropivacaine and fentanyl for epidural analgesia after total knee arthroplasty. A single injection ultrasound-assisted femoral nerve block provides side effect-sparing analgesia when compared with intrathecal morphine in patients undergoing total knee arthroplasty. Continuous peripheral nerve blocks in hospital wards after orthopedic surgery: a multicenter prospective analysis of the quality of postoperative analgesia and complications in 1,416 patients. Outpatient management of continuous peripheral nerve catheters placed using ultrasound guidance: an experience in 620 patients. The Second American Society of Regional Anesthesia and Pain Medicine evidence-based medicine assessment of ultrasound guided regional anesthesia. Ultrasound-guided interscalene blocks: understanding where to inject the local anaesthetic. The maximum effective needle-to-nerve distance for ultrasound-guided interscalene block: an exploratory study. For outpatient rotator cuff surgery, nerve block anesthesia provides superior same-day recovery over general anesthesia. Brachial plexus examination and localization using ultrasound and electrical stimulation: a volunteer study. Comparison of a single- or double-injection technique for ultrasound-guided supraclavicular block: a prospective, randomized, blinded controlled study. Ultrasound-guided supraclavicular brachial plexus block: single versus triple injection technique for upper limb arteriovenous access surgery. Clinical sonopathology for the regional anesthesiologist: part 1: vascular and neural. Clinical sonopathology for the regional anesthesiologist: part 2: bone, viscera, subcutaneous tissue, and foreign bodies. Neurostimulation in ultrasound-guided infraclavicular block: a prospective randomized trial. The Houdini clavicle: arm abduction and needle insertion site adjustment improves needle visibility for the infraclavicular nerve block. Use of magnetic resonance imaging to define the anatomical location closest to all three cords of the infraclavicular brachial plexus. Sonographically guided infraclavicular brachial plexus block in adults: a retrospective analysis of 1146 cases. Infraclavicular perineural local anesthetic infusion: a comparison of three dosing regimens for postoperative analgesia. The posterior lumbar plexus (psoas compartment) block and the three-in-one femoral nerve block provide similar postoperative analgesia after total knee replacement.
10 mg atorlip-10 buy amex
Furthermore cholesterol medication for life 10 mg atorlip-10 purchase with visa, convulsions are typically noted before the onset of cardiac toxicity cholesterol test procedure atorlip-10 10 mg amex, which also confers a greater safety level over bupivacaine foods to bring cholesterol down order atorlip-10 in india. As a result, in populations with lower circulating pseudocholinesterase levels, there is a modestly increased serum half-life of these drugs. The duration of action of the drug is short; hence, a continuous infusion of chloroprocaine is recommended even when used for only intraoperative anesthesia. This drug is experiencing a resurgence within the neonatal population as interest in its safety profile has reinvigorated its use. Even though neonates have a lower level of circulating pseudocholinesterase, the plasma half-life of chloroprocaine remains short. The plasma half-life of chloroprocaine in adults is 23 seconds, whereas in neonates it is 43 seconds. The plasma half-life of lidocaine, an intermediate-acting amide local anesthetic, is 90 to 120 minutes. Thus, the toxicity profile of chloroprocaine is expected to be much better across a range of doses, though studies in neonates have not been specifically designed to answer this clinical question. This level will be effective in producing complete surgical78 anesthesia for neonates’ major abdominal surgery. Lower doses such as 1 mL/kg bolus and an infusion of 1 mL/kg/hr have been used successfully for 2958 inguinal and penoscrotal surgery. Given the high concentrations of local that79 can be used, motor block is easy to achieve with this local anesthetic. Its effect on human models was parlayed in80 a case report where lipid was used as a last resort to reverse the effects of bupivacaine following a regional anesthesia technique. Lipid should be81 readily available if local anesthetics are being used in neonates. There is a report where an infant received a caudal block which resulted in cardiac toxicity which was treated successfully with lipid rescue. Although82 guidelines for neonatal administration of lipid rescue do not exist, lipid administration across a wide range of doses appears to be safe in neonates. The most common local anesthetic preparations for topical use include lidocaine, tetracaine, benzocaine, and prilocaine. When these are applied to skin they produce effective but relatively short duration of analgesia. The preparation has to be applied under an occlusive bandage for 45 to 60 minutes to obtain effective cutaneous analgesia. Liposome-encapsulated86 lidocaine or tetracaine has been shown to remain in the epidermis after topical application, affording a fast and lasting anesthetic effect. For safe and effective care, the anesthesiologist must take extraordinary caution to understand the current status of the patient, the nature of the planned surgery, and the potential need for stabilization and preparation before surgery. After ensuring that the patient has been adequately prepared, the anesthesiologist needs to develop a detailed plan that encompasses the issues of anesthetic equipment and monitoring, airway management, drug choice, fluid management, temperature control, anticipated surgical needs, pain management, and postoperative care. Studies have shown that morbidity and mortality related to anesthesia is higher in infants, especially neonates, compared with infants, older children, and adults. There are probably several89 causes for the higher complication rate observed with neonatal surgery, including the emergent nature of most surgical procedures that are performed at this age, the physiologic instability of the neonate, the relative lack of experience most clinicians have with patients in this age range, and the technical challenges of monitoring and treating a very small patient. Because of the specialized nature of neonatal surgery and care, it is important that each institution that provides care to these patients has the resources of equipment, critical care facilities, nursing, laboratory, blood bank, and social work necessary to meet the needs of these patients and their families, as well as systems in place to guarantee a robust quality assurance emphasis on the provision of care. Both the American Academy of Pediatrics and the American Society of Anesthesiologists have provided guidance to many of the systems issues that should be addressed in institutions caring for these patients. In the distant past, concerns about physiologic instability and other challenges of caring for neonates led some practitioners to use minimal or no anesthesia for both minor and major procedures. It is now widely recognized that neonates have stress responses similar to those of older patients, and the lack of adequate anesthetic care is as inhumane in the neonate as it is in the older child or adult. The neurologic system in neonates is sufficiently91 developed to transmit painful stimuli and lack of pain control may result in a higher morbidity rate, increased pain to subsequent events, and increased neuroendocrine response to painful stimuli.
Syndromes
- Childhood infections, such as meningitis, mumps, scarlet fever, and measles
- Serum potassium
- Healthy snacks
- Hypoparathyroidism
- Pallor
- Beckwith syndrome
- "Prancing" and wide walk
- Joint or muscle pain
- Abnormal blood vessels (arteriovenous malformation)
Order atorlip-10 overnight delivery
If neuraxial instrumentation is attempted cost of cholesterol test buy discount atorlip-10 10 mg on-line, heparin dosing should be delayed per current guidelines cholesterol meaning generic 10 mg atorlip-10 otc. Induction of general anesthesia and intubation can be associated with dramatic hemodynamic lability and sympathetic stimulation cholesterol test explained atorlip-10 10 mg for sale, which may put the aneurysm at risk of rupture. It is prudent to ensure adequate blood product availability in the operating room and large-bore peripheral intravenous access prior to the induction of general anesthesia. There is no single “best” induction technique; regardless of agents chosen, the goal is a smooth induction with stable hemodynamics and avoidance of tachycardia or hypertension. Preinduction placement of an arterial line may aid in appropriate titration of induction agents. Central venous catheterization is generally employed for monitoring volume trends and for the reliable delivery of vasoactive medication. Cardiac function is commonly assessed with either a pulmonary artery catheter or transesophageal echocardiography. Either technique can provide valuable information about cardiac functioning and volume status. Echocardiography is the most sensitive marker for new regional wall motion abnormalities and direct visualization of appropriate ventricular filling. Pulmonary artery catheterization can be useful both intraoperatively and postoperatively to guide resuscitation. The use of pulmonary artery catheters has been the subject of debate, with conflicting evidence as to their benefit in high-risk surgical patients. As with any monitor, the information obtained is only as good as the clinician interpreting and intervening upon the data. Virtually all anesthetic drugs and techniques have been described for aortic reconstructive surgery. The ability to maintain hemodynamic equilibrium and attend to detail is far more important than is the choice of drug. Volatile agents may improve preconditioning mechanisms should myocardial ischemia occur. The maintenance anesthetic is designed to maintain hemodynamics within 20% of the baseline range. An array of short-acting vasoactive agents (including vasodilators, vasopressors, and inotropes) should be on hand to immediately treat hemodynamic lability. Alternatively, deepening the anesthetic or injection of the epidural catheter with local anesthetic will increase vasodilation, although both of these approaches require careful attention to avoid unintended hypotension. When there is concern about spinal cord perfusion, it may be prudent to allow permissive hypertension, to the extent possible, above the level of the clamp to provide higher distal perfusion pressure and avoid distal ischemia. After the vascular clamps are placed and the aneurysm sac is incised, blood loss is swift from any vessels arising from the aorta between the two clamps. Blood loss can be considerable without the onset of hypotension or tachycardia because a significant portion of the vascular tree is excluded from circulation during aortic occlusion. An autotransfusion device should be employed to reduce the amount of autologous blood needed. It is prudent to volume load during the period of aortic cross-clamping in anticipation for the vasoplegic washout and reactive hyperemia that will occur with the removal of aortic cross-clamp. This augmentation of central volume will then fill the increased capacitance distal to the aortic clamp when it is subsequently released. Immediately prior to the removal of the aortic clamp, vasodilating agents are discontinued. The surgeon opens the aortic clamp gradually to ensure that severe hypotension or bleeding does not develop. Ongoing fluid resuscitation and vasopressor and inotropic support is frequently necessary. Severe refractory hypotension can be temporarily abated with reapplication of the aortic cross-clamp until appropriate measures can be instituted. Over the course of the reconstruction, there may be frequent instances of cross-clamp application and release to limit the ischemic time to vital organs and to “test” the anastomoses.
Discount atorlip-10 10 mg visa
Both compliance and inspiratory elastic work can be measured for a single breath by measuring airway pressure (Paw) cholesterol side effects buy atorlip-10 10 mg low price, intrapleural (Ppl) pressure cholesterol medication sore muscles discount atorlip-10 10 mg fast delivery, and tidal volume cholesterol medication zetia atorlip-10 10 mg purchase with amex. If esophageal pressure is measured correctly, the esophageal pressure values can be substituted for Ppl values. Elastic work (W ) is performed during inspiration only because expirationel is passive during normal breathing. The area within the triangle in Figure 15- 2 describes the work required to inspire. The equation that yields elastic work (and the area of the triangle) is Resistance to Gas Flow Both laminar and turbulent flows exist within the respiratory tract, usually in mixed patterns. Laminar Flow Below critical flow rates that create turbulent flow, gas proceeds through a straight tube as a series of concentric cylinders that slide over one another. Fully developed flow has a parabolic profile with a velocity of zero at the cylinder wall and a maximum velocity at the center of the advancing “cone. The advancing conical front means that some fresh gas reaches the end of the tube before the tube has been completely filled with fresh gas. Thus, laminar flow in the airways results in alveolar ventilation that can occur even when the tidal volume (Vt) is less than anatomic dead space. As noted by Rohrer in 1915, it allows high-frequency14 ventilation to achieve adequate alveolar ventilation. Resistance (R) to laminar gas flows in a straight, unbranched cylinder can be calculated by the following equation of Poiseuille: where P and P are barometric and alveolar pressures. It is essential to noteB A that as radius decreases in narrowed airways, resistance will increase by a power of four. Viscosity is the only physical gas property that is relevant under conditions of laminar flow. However, if flow is turbulent due to critical airway narrowing or abnormally high airway resistance, low-density helium is potentially useful therapy (see next section). Turbulent Flow High flow rates, particularly through branched or irregularly shaped tubes, disrupt the orderly flow of laminar gas. When resistance to gas flow is significant, turbulent flow occurs and is usually audible. Turbulent flow usually presents with a square front; fresh gas will not reach the end of the tube until the amount of gas entering the tube is almost equal to the volume of the tube. Four conditions that will change laminar flow to turbulent flow are high gas flows, sharp angles within the tube, branching in the tube, and a decrease in the diameter of the tube. Conversely, during turbulent flow, resistance increases significantly in proportion to the flow rate. A detailed description of these phenomena is beyond the scope of this chapter, but the reader is referred to descriptions by Nunn. Mild expiratory resistance does not result in muscle use for active exhalation in conscious or anesthetized subjects. Instead, the initial work to overcome expiratory resistance is performed by augmenting inspiratory force until a sufficiently high lung volume is achieved that allows elastic recoil to overcome expiratory resistance. Only when19 expiratory resistance becomes excessive are accessory muscles recruited to expel gas from the lungs. During acute increases in expiratory resistance, this response is well tolerated by most patients. However, chronic use of 951 accessory muscles to exhale significantly increases the risk of ventilatory failure as the work of breathing is further increased. Work of breathing that exceeds physiologic reserves becomes detrimental to physiologic homeostasis, and increases the risk of ventilatory failure. Acute ventilatory failure secondary to muscle fatigue is evidenced by an acute increase in arterial carbon dioxide. Physiologic Changes in Respiratory Function Associated with Aging Physiologic aging of the lung is associated with dilation of the alveoli, enlargement of the airspaces, decrease in exchange surface area, and loss of supporting tissue.

Best 10 mg atorlip-10
When an infusion is terminated at steady state cholesterol test fasting requirements order atorlip-10 10 mg on-line, input into the system’s central compartment is lost and net transfer of drug is no longer zero cholesterol profile values cheap atorlip-10 generic. Instead lowering cholesterol with diet change cheap 10 mg atorlip-10, net drug distribution immediately begins moving toward the central compartment from the peripheral compartments rather than away, as was the case during infusion, and elimination from the central compartment continues unabated by the infusion’s input. Plasma or central compartment concentrations will fall relatively rapidly, compared to the elimination half- life, until set concentration ratios of central:fast and central:slow are achieved. These ratios with higher peripheral compartment drug concentrations will achieve the net drug distribution flux into the central compartment that will balance the elimination flux to create a constant elimination rate. During the elimination phase, the multicompartmental system behaves, kinetically, as a single compartment, but only does so because there are (fixed) drug concentration ratios among the compartments. With a short infusion, the peripheral compartment drug concentrations will have only achieved low drug concentrations, and the plasma drug concentration will have to fall quite far to reach the central:peripheral drug concentration ratios needed to enter the constant elimination phase. After a very long infusion with peripheral compartment drug concentrations reaching higher drug concentrations as they approach their steady state, plasma drug concentrations will not need to fall as much to reach the concentration ratios required for the elimination phase, and the rate of plasma drug decline will begin approaching the elimination half-life sooner, resulting in longer half-times. This means it cannot be extrapolated backward or, more importantly, forward to lesser or greater drug concentration decrements, as is possible with true kinetic parameters. Rather, a model of the specific drug pharmacokinetics is programmed into a simulation with a set drug infusion regimen; tedious for pencil and paper or handheld calculator, but a simple 709 matter for even a modest computing device (e. It could be less than one-half or, as is likelier in practice, more than one-half. Therefore, simulating both the specific infusion context as well as the required percentage decrease from the target concentration should be done to get the best estimate of when a drug’s effect will reach the clinically desired end point. Figure 11-18 The context-sensitive 25%, 50%, and 75% plasma decrement times for fentanyl, alfentanil, sufentanil, and remifentanil. Although a 50% decrease in plasma concentration is an appealing and comprehensible parameter, larger or smaller decreases in plasma concentrations may be required for recovery from the drug. Simulations show that the times for different percent decreases in plasma concentration are not linear. In addition, if the concentration of interest is the effect site concentration rather 710 than the plasma concentration, simulations can be performed to calculate the context-sensitive effect site decrement time. Finally, if a constant plasma or effect site concentration is not maintained throughout the delivery of the drug (which is typically the case with manual bolus and infusion schemes and also with varying drug requirements depending on surgical stimulation, etc. If precise drug administration data are known, it is possible to compute the context-sensitive decrement time for the individual situation or context. Soft Pharmacology and Anesthesiology Accumulation of drug in well perfused but inactive tissue beds (i. When the arterial concentration of drug is less than the tissue concentration of drug in any of these tissue depots, the drug redistributes from the tissue back into the plasma, thereby slowing the rate of decline of the plasma concentration. One strategy that has been used to limit tissue uptake of drug is to design active compounds that are rapidly metabolized by plasma and/or tissue enzymes into inactive metabolites—so-called soft drugs. However, the preclinical data have resulted in selection of an etomidate analog that has context insensitive decrement times as well as limited adrenal suppression. However, in the operating room, once the anesthetic has commenced, without the help of a computer, software, and possibly an assistant, it is laborious and difficult to make any calculations to determine how to adjust the infusion or how to bolus (or stop the infusion) to increase or decrease the target plasma concentration. The blue line represents the predicted plasma propofol concentration of 5 μg/mL, which in theory is attained at time t = 0 and is then maintained by a variable rate infusion. The red line is the predicted effect site concentration under the conditions of a constant pseudo–steady-state plasma concentration. Note that 95% of the target concentration is reached in the effect site at approximately 4 minutes. The success of this approach is influenced by the extent to which the drug pharmacokinetic and pharmacodynamic parameters programmed into the computer match those of the particular patient at hand. For a computer-control pump to produce and maintain a plasma drug concentration it must first administer a dose equal to the product of the central compartment, V , and the target concentration (1 Fig. Then for each moment after that, the amount of drug to be administered into the central compartment to maintain the target concentration is equal to drug eliminated from the central compartment plus drug distributed from the central compartment to peripheral compartments minus drug returning to the central compartment from peripheral compartments. The software keeps track of the estimated drug in each compartment over time and applies the rate constants for intercompartmental drug transfer from the pharmacokinetic model to these amounts to determine drug movement at any given time. It then matches the estimated concentrations to the target concentration at any time to determine the amount of drug that should be infused. The software can also predict future concentrations, usually with the assumption that the infusion will be stopped so that emergence from anesthesia or the dissipation of drug effect will occur optimally according to the context-sensitive decrement time.
10 mg atorlip-10 amex
Impella group cholesterol levels malaysia buy cheap atorlip-10 line, but to date there is no mortality Indications for the use of the Impella 5 cholesterol ratio 3.4 discount 10 mg atorlip-10 visa. It is used in the setting of ade cholesterol count for foods atorlip-10 10 mg on line, damage to the aortic valve, device malfunc- lef ventricular or biventricular failure. Hemolysis from mechanical confguration, the infow cannula is placed via a shearing can also occur in 5–10% of patients but large central vein. If renal extracorporeal pump but is returned to the body failure from persistent hemolysis occurs, the afer gas exchange through an arterial cannula. Potential complications uration both the infow cannula and the outfow include bleeding, vascular injury, limb isch- cannula are placed through a venous access, emia, thromboembolic events, and pump fail- sometimes even the same vein if a dual lumen ure. Because blood is being removed by placement of a reperfusion cannula to pro- from and returned to a vein, it ofers no hemody- vide additional blood flow to the limb distal to namic support and functions only for gas the cannulation site. The ited surgical approaches, the durability is limited, amount of flow generated is dependent on the and vascular complication rates are somewhat size of the cannulae and the speed of the pump. Tus, determined by the type of oxygenator in the cir- when these conditions are present, it can be easier cuit. Te consensus has been that if patients are able to survive their index hospitalization, Treatment of right ventricular failure in cardio- their overall mortality is good. Tough this genic shock has been predominantly medical in remains true, the in-hospital mortality is high in nature. Once placed, the insertion sheath is torn of, and a graded smaller sheath is advanced and secured with a mattress suture. Te inlet sits in the inferior vena cava where blood is aspirated and pumped into the proximal pulmo- nary artery (. Contraindications include with percutaneous device implantation due to severe regurgitation, stenosis, or mechanical its rigid nature and somewhat technically chal- replacement of the tricuspid or pulmonic lenging insertion. It can be limited by anatomy valves, anatomic conditions that preclude place- which ofen is not known until insertion is ment or correct positioning of the pump attempted. Tere Cost-efectiveness has increasingly become a are no clinical trials comparing the beneft of focus in healthcare. Classifcation of these patients was genic shock and require a higher level of support based on coding, however, and not clinical assess- than medical therapy provides. Higher cost of an intervention over medical shock are needed before the cost-efectiveness of therapy is acceptable if it translates into survival these therapies can be determined meaningfully. A potential example of this evolu- Yarzebski J (2009) Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospi- tion is the HeartMate Percutaneous Heart Pump tal death rates associated with cardiogenic shock (St. Scheidt S, Wilner G, Mueller H, Summers D, Lesch M, ofering some protection to the surrounding Wolf G et al (1973) Intra-aortic balloon counterpulsa- structures. Ann Thorac Surg 74(3):746– 751 discussion 51-2 Patients who present in cardiogenic shock con- 8. J Am Coll Cardiol 36(3 Suppl A):1123–1129 and type of support needed, the experience of the 9. J Am Coll Cardiol without mortality beneft in the limited studies to 30(3):708–715 date. Tere is a clear need for random- complicating acute myocardial infarction: data from the National Registry of Myocardial Infarction 2. Am ized, prospective trials to evaluate the efect of Heart J 141(6):933–939 these devices on mortality in patients with car- 11. Interact Cardiovasc Thorac Surg 8(6): cal expert consensus statement on the use of percuta- 682–683 neous mechanical circulatory support devices in 22. Sociedad Latino Americana de Cardiologia J Heart Lung Transplant 29(1):96–97 Intervencion; Afrmation of Value by the Canadian 23. J Am Coll left ventricular assist device: a bridge to coronary Cardiol 65(19):e7–e26 artery bypass grafting and cardiac transplantation. Am diogenic shock: the Academic Medical Center inten- Heart J 152(3):469 e1-8 sive care unit experience. Tex Heart Inst J 33(2):111–115 impact of heart failure in the United States: a policy 16. Circulation 131(4):e29–322 Jegaden O (2008) The right axillary artery approach 28. Ann S, Maini B et al (2013) A value-based analysis of Thorac Surg 85(4):1468–1470 hemodynamic support strategies for high-risk heart 18. Bresson D, Sibellas F, Farhat F, Jegaden O, Kirkorian G, failure patients undergoing a percutaneous coronary Bonnefoy E (2011) Preliminary experience with intervention.
Purchase discount atorlip-10 line
Sometimes this vessel rises as high as 4 cm above the Muscles (Figure 7-4) clavicle; occasionally lower cholesterol foods best order 10 mg atorlip-10 with visa, it passes in front of the anterior scalene or pierces the fbers of that muscle cholesterol levels what is good atorlip-10 10 mg order. Te subclavian vein lies Platysma behind the clavicle and is not usually seen in this space; in some cases it rises as high as the artery cholesterol levels high during pregnancy order atorlip-10 american express, and it has even been Te platysma originates from the fascia overlying the pecto- seen to pass with that vessel behind the anterior scalene. Te ralis major and deltoid muscle and inserts into the depression brachial plexus of nerves lies above the artery, in close contact muscles of the corner of the mouth, the mandible, and the with it. Tese layers are important because they help compartmentalize the various anatomic structures of the neck. It receives its blood supply from branches of the submental and suprascapular arteries. Te surgeon must keep in mind several opposite side and tilt the head toward the ipsilateral shoulder. It functions to depress the hyoid and tense the mentum nuchae, and the spinous process of C7 and T1-T12 deep cervical fbers. Te superior belly lies superfcial transverse cervical artery or superfcial cervical artery. Surgically, it delineates the posterior limit of Level of the mylohyoid for dissection of the submandibular V neck dissections. Blood Vessels (see Figure 7-2) Digastric Te digastric muscle, much like the omohyoid, consists of Blood supply to the neck can be divided according to the two muscles, an anterior belly and a posterior belly. Tey regional supply: anterior triangle, posterior triangle, and root originate at the digastric fossa of the mandible at the sym- of the neck. Te posterior belly is the common carotid artery, which ascends through the neck innervated by the facial nerve, and the anterior belly is inner- within the carotid sheath (Figure 7-5). Te posterior belly any branches until it reaches the level of the hyoid bone, at receives its blood supply from the occipital artery, whereas which point it divides into the internal carotid and external the anterior belly receives its blood supply from the submen- carotid arteries. Tis muscle elevates the hyoid branches as it moves upward to the base of the skull. Te bone and depresses the mandible (assisting the lateral ptery- external carotid, however, extends upward toward the parotid goid). Te anterior belly is the landmark for identifcation auricular arteries (see Figure 7-4). All veins of the anterior triangle, except the anterior jugular vein, drain to the internal jugular vein (Figure Te spinal accessory nerve originates in the spinal nucleus 7-4). Te internal jugular vein travels within the carotid and may extend to the ffth cervical segment. Te motor sheath, picking up the following tributaries as it descends: neurons of this branch pass through two foramina, the veins of the pharyngeal plexus, facial vein, lingual vein, supe- foramen magnum and jugular foramen. Within the posterior triangle of the neck, the subclavian Phrenic Nerve (see Figure 7-2) artery supplies the majority of the arterial blood. Two cervical branches, the transverse cervical and suprascapular, pass ante- Te phrenic nerve (C3, C4, and C5) is the sole nerve supply riorly to the anterior scalene muscle and pin down the phrenic to the diaphragm. It also lies posterior and lateral to the posterior triangle, where it picks up venous blood from three carotid sheath. Both the suprascapular and transverse cervical sources: the transverse cervical vein, suprascapular vein, and arteries also pass anteriorly to the anterior scalene, clamping anterior jugular vein. Hypoglossal Nerve Te root of the neck also contains the source of many of the vessels that eventually supply the majority of the vascular Te hypoglossal nucleus originates from the medulla oblon- supply of the neck. Te subclavian artery arches superiorly gata, and the hypoglossal nerve arises from the cell bodies of over the frst rib, becoming the axillary artery and giving of the hypoglossal nucleus. Te path of this nerve is also important thyrocervical trunk, and costocervical trunk. It ends as Nerves it extends upward along the hyoglossus muscle and into the genioglossus, fnally reaching the tip of the tongue. Although metastatic neck disease is one of the most Marginal Mandibular Nerve important factors in the spread of head and neck squamous (see Figure 7-2) cell carcinoma from primary sites, it is not encountered as Te marginal mandibular nerve is an important landmark, frequently as some of the other potential pathologies associ- and care should be taken to ensure its preservation during ated with the neck.
Kaelin, 23 years: Ambulatory Knee Surgery Ambulatory knee surgery has increased because health-care costs have encouraged outpatient management of less complex cases.
Marius, 21 years: Patients for certain procedures such as laparoscopic cholecystectomy or transurethral resection of the prostate should live close to the ambulatory facility because postoperative complications may require their prompt return.
Gamal, 61 years: Continuous psoas compartment block for anesthesia and perioperative analgesia in patients with hip fractures.
Yugul, 40 years: If pulmonary blood flow decreases, the most likely cause is a decreased cardiac output.
Lee, 50 years: Detection of an immediate early gene “anti-sense” tran- script by in situ hybridization.
Sigmor, 46 years: In this way blood is subsequently warmed or cooled and maintained at a desired temperature.
Narkam, 54 years: Tools such as a specialist opinion unless it is certain that the lesion is benign.
Lisk, 41 years: In adults, naevi, appendageal tumours, sebaceous hyperplasia and small cysts all large solitary lesions are hard to distinguish from non-melanoma skin cancer.
Hengley, 56 years: Te concept gave rise to a debate about I thought that we should follow Claude Bernard’s whether or not a pulse is necessary.
Jorn, 22 years: Warfarin-induced skin necrosis is a thrombotic complication often occurring when previously unrecognized congenital protein C deficiency accentuates this imbalance.
Falk, 53 years: A fexible membrane of four layers sideration in the mind of the author since he separates air from blood (.
Nemrok, 37 years: In patients who are obese, edentulous, or bearded, two hands or a mask strap may be required to ensure an adequate mask seal.
8 of 10 - Review by M. Wilson
Votes: 36 votes
Total customer reviews: 36
References
- Loh S, Bagheri S, Katzberg RW, et al: Delayed adverse reaction to contrastenhanced CT: a prospective single center study comparison to control group without enhancement, Radiology 255:764-771, 2010.
- Su TH, Wang KG, Hsu CY, et al: Prospective comparison of laparoscopic and traditional colposuspensions in the treatment of genuine stress incontinence, Acta Obstet Gynecol Scand 6(76):576n582, 1997.
- Viscoli C, Machetti M, Cappellano P, et al. False-positive galactomannan platelia Aspergillus test results for patients receiving piperacillin-tazobactam. Clin Infect Dis 2004; 38: 913-916.
- Cox D, Taylor J, Nanda NC. Refractory hypoxemia in right ventricular infarction from right-to-left shunting via a patent foramen ovale: efficacy of contrast transesophageal echocardiography. Am J Med. 1991;91(6):653-655.