Sharon Krystofiak, M.S., M.T. (A.S.C.P.), C.I.C.
- Infection Preventionist
- Infection Control and Hospital
- Epidemiology
- University of Pittsburgh Medical Center Presbyterian
- Pittsburgh, Pennsylvania
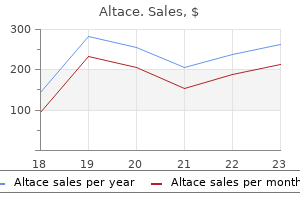
Altace dosages: 10 mg, 5 mg, 2.5 mg
Altace packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Buy altace online from canada
It is an expensive and invasive test that can cause some side effects arteria3d mayan city pack altace 5 mg buy free shipping, although these side effects are rarely lethal prehypertension journal order altace discount. Part of the art of medicine is determining which patients with one negative ultrasound can safely wait for a confirmatory ultrasound 3 days later blood pressure medication for ptsd buy online altace, and which patients 248 Essential Evidence-Based Medicine need to have an immediate venogram or initiation of anticoagulant medica- tion therapy. This considers biophysiological parameters, symptom severity, functional outcome, patient utility, expected values, morbidity avoided, mor- tality change, and cost-effectiveness of outcomes. We will discuss some of these issues in the chapter on decision trees and patient values (Chapter 31). Even a cheap test, if done excessively, may result in prohibitive costs to society. Out- comes include the additional cost of evaluation or treatment of patients with false positive test results and the psychosocial cost of these results on the patient and community. Other outcomes are the risk of missing the correct diagnosis in patients who are falsely negative and may suffer negative out- comes as a result of the diagnosis being missed. Again, physicians may need to also consider a cost analysis for evaluating the test. Interestingly, the per- spective of the analysis can be the patient, the payor, or society as a whole. Overall, patient or societal outcomes ultimately determine the usefulness of a test as a screening tool. Bertrand Russell (1872–1970): The Philosophy of Logical Atomism, 1924 Learning objectives In this chapter you will learn: r the characteristics and definitions of normal and abnormal diagnostic test results r how to define, calculate, and interpret likelihood ratios r the process by which diagnostic decisions are modified in medicine and the use of likelihood ratios to choose the most appropriate test for a given purpose r how to define, calculate, and use sensitivity and specificity r how sensitivity and specificity relate to positive and negative likelihood ratios r the process by which sensitivity and specificity can be used to make diag- nostic decisions in medicine and how to choose the most appropriate test for a given purpose In this chapter, we will be talking about the utility of a diagnostic test. This is a mathematical expression of the ability of a test to find persons with disease or exclude persons without disease. These are the likelihood ratios and the prevalence of disease in the target population. Additional test characteristics that will be introduced are the sensi- tivity and specificity. These factors will tell the user how useful the test will be in the clinical setting. Using a test without knowing these characteristics will result in problems that include missing correct diagnoses, over-ordering tests, increas- ing health-care costs, reducing trust in physicians, and increasing discomfort 249 250 Essential Evidence-Based Medicine and side effects for the patient. Once one understands these properties of diag- nostic tests, one will be able to determine when to best order them. The indications for ordering a diagnostic test can be distilled into two simple rules. They are: (1) When the characteristics of that test give it validity in the clinical setting. Will that result help in correctly identifying a diseased patient from one without disease? What will a positive or negative test result tell me about this patient that I don’t already know and that I need to know? If the test that is being considered does not fall into one of these categories, it should not be done! Diagnostic tests are a way of obtaining information that provides a basis for revis- ing disease probabilities. When a patient presents with a clinical problem, one first creates a differential diagnosis. One attempts to reduce the number of dis- eases on this list by ordering diagnostic tests. Ideally, each test will either rule in or rule out one or more of the diseases on the differential diagnosis list. Diseases which are common, have serious sequelae such as death or disability, or can be easily treated are usually the ones which must initially be ruled in or out. We rule in disease when a positive test for that disease increases the probability of disease, making its presence so likely that we would treat the patient for that disease.
Discount 10 mg altace
Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease 21 While whole-genome sequencing remains expensive by the standards of most clinical laboratory tests blood pressure ranges order altace with amex, the trend-line leaves little doubt that costs will drop into the range of many routine clinical tests within a few years hypertension classification discount altace 2.5 mg with amex. Whole-genome sequencing will soon become cheaper than many of the specific genetic tests that are widely ordered today and ultimately will likely become trivial compared to the cost of routine medical care hypertension nclex questions order altace line. Instead, the clinical utility of genome sequences and public acceptance of their use will drive future developments. However, it is by no means unique: parallel developments in other areas of molecular analysis, such as the analysis of large numbers of small-molecule metabolites and proteins, and the detection of single molecules, are likely to sweep away purely economic barriers to the diffusion of many data-intensive molecular methods into biomedical research and clinical medicine. These technologies will make it possible to monitor and ultimately to understand and predict the functioning of complex molecular networks in health and disease. The Opportunity to Integrate Data-Intensive Biology with Medicine Human physiology is far more complex than any known machine. The molecular idiosyncrasies of each human being underlie both the exhilarating potential and daunting challenges associated with “personalized medicine”. Individual humans typically differ from each other at millions of sites in their genomes (Ng et al. More than ten thousand of these differences are known to have the potential to alter physiology, and this estimate is certain to grow as our understanding of the genome expands. All of this new genetic information could potentially improve diagnosis and treatment of diseases by taking into account individual differences among patients. We now have the technology to identify these genetic differences — and, in some instances, infer their consequences for disease risk and treatment response. Some successes along these lines have already occurred; however, the scale of these efforts is currently limited by the lack of the infrastructure that would be required to integrate molecular information with electronic medical records during the ordinary course of health care. The human microbiome project represents an additional opportunity to inform human healthcare. The microorganisms that live inside and on humans are estimated to outnumber human somatic cells by a factor of ten. A growing list of diseases, including obesity, inflammatory bowel disease, gastrointestinal cancers, eczema, and psoriasis, have been associated with changes in the structure or function of human microbiota. The ultimate goal of studying the human microbiome is to better understand the impact of microbial variation across individuals and populations and to use this information to target the human microbiome with antibiotics, probiotics, and prebiotics as therapies for specific disorders. While this field is in its infancy, growing knowledge of the human microbiome and its function will enable disease classification and medicine to encompass both humans and their resident microbes. Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease 22 individuals. Lifestyle interventions alone are ineffective in these individuals at reducing the likelihood of early-onset cardiovascular disease (Huijgen et al. Consequently, the ability to identify the patients that carry the non-functional receptor makes it possible to proceed directly to the use of statin drugs at an early age, rather than first attempting to control cholesterol with diet and exercise. There is strong evidence that the early use of statin drugs in these individuals can provide a therapeutic benefit. These mutations predispose to cancer, particularly breast and ovarian cancer (King et al. Women who carry these mutations can reduce their risk of death from cancer through increased cancer screening or through prophylactic surgeries to remove their breasts or ovaries (Roukos and Briasoulis 2007); until these mutations were identified it was not possible to determine who carried the mutations or to take proactive steps to manage risk. In addition, epidemiological studies and other data have raised the possibility that H. The human genome and microbiome projects are only two examples of emerging biological information that has the potential to inform health care. It is similarly likely that other molecular data (such as epigenetic or metabolomic data), information on the patient’s history of exposure to environmental agents, and psychosocial or behavioral information will all need to be incorporated into a Knowledge Network and New Taxonomy that would enhance the diagnosis and treatment of disease. Traditionally, lung cancers have been divided into two main types based on the tumors’ histological appearance: small- cell lung cancer and non-small-cell lung cancer. Non-small-cell lung cancer is comprised of three sub-groups, each of them defined by histology, including adenocarcinoma, squamous- cell carcinoma, and large cell carcinoma. Since 2004, knowledge of the molecular drivers of non-small-cell lung cancer has exploded (Figure 2-1). Drivers are mutations in genes that contribute to inappropriate cellular proliferation.
Buy genuine altace line
Researchers and readers must always be concerned about social desirability bias when considering the responses 212 Essential Evidence-Based Medicine or comments that participants may provide when they know they are being observed blood pressure vitals purchase 5 mg altace mastercard. The extent to which researchers attempt to collect richly detailed per- spectives from study subjects can help to reassure the reader that subjects at least had ample opportunity to express their knowledge blood pressure when sick altace 5 mg order on line, attitudes arrhythmia and chest pain discount 10 mg altace amex, or concerns. The approach that researchers take will reflect the study question, the nature of the available data, and the preferences of the researchers themselves. Nevertheless, several key principles should guide all qualitative analyses, and readers should be able to assess how well the study adhered to these principles. This point may seem obvious, but it is important that readers feel reasonably confident that the data collection not only captured all relevant perspectives but that the analysis did not disregard or overlook elements of data that should be considered. There is no sure-fire way to determine whether all data were included in the analysis, but readers can rea- sonably expect study authors to report that they used a systematic method for cataloguing all data elements. Consider whether multiple observers participated in the analysis and whether the data were reviewed multiple times. The agreement between observers, also known as the inter-rater reliability, should be measured and reported. The results of interviews or open-ended questions can be analyzed using an iterative technique of identification of common themes. First the answers to questions given by an initial group are reviewed and the important themes are selected by one observer. A sec- ond researcher goes over those same responses with the list of themes and cat- alogues the responses, blinded from the results of the first researcher. Following this process, inter-rater reliability is assessed and quantified using a test such as the Kappa statistic. If the degree of agreement is substantial, one reviewer can categorize and analyze the remaining responses. Studies of human subjects’ attitudes or perspectives rarely yield a set of obser- vations that unanimously signal a common theme or perspective. It is common in qualitative studies for investigators to come upon observations or sentiments that do not seem to fit what the preponderance of their data seem to be signaling. These discrepancies are to be expected in qualitative research and, in fact, are an important part of characterizing the range of emotions or behaviors among the study participants. Readers should be suspicious of the study’s findings if the results of a qualitative study all seem to fall neatly in line with one salient emerg- ing theory or conclusion. Triangulation refers to the process by which key findings are verified or corroborated through multiple sources. For example, researchers will frequently have subjective reactions to qualitative data, and these reactions help them to formulate conclusions and should lead to further data collection. Having multiple researchers indepen- dently analyzing the primary data helps to ensure that the findings are not unduly influenced by the subjective reactions of a single researcher. Another form of triangulation involves comparing the results of the analysis with exter- nal information, either from or about the study participants or from other stud- ies. Theories or conclusions from one study may not be consistent with existing theories in similar fields, but when such similarities are observed, or when the results would seem to fit broader social science theories or models, researchers and readers may be more confident about the validity of the analysis. Researchers frequently perform another form of triangulation known as member-checking. This approach involves taking the study findings back to the study participants and verifying the conclusions with them. Frequently, this pro- cess of member-checking will lead to additional data and further illumination of the conclusions. Since the purpose of qualitative research is, in large measure, to describe or understand the phenomena of interest from the perspective of the participants, member-checking is useful, because the participants are the only ones who can legitimately judge the credibility of the results. Readers of qualitative articles will encounter a few analytic approaches and principles that are commonly employed and deserve mention by name. A con- tent analysis generally examines words or phrases within a wide range of texts and analyzes them as they are used in context and in relationship with other lan- guage. Using this approach, researchers immerse themselves repeatedly in the collected data, usually in the form of transcripts or audio or video recordings, and through iterative review and interaction in investigator meetings, coupled with reflection and intuitive insight, clear, consistent, and reportable observations emerge and crystallize.
Altace 10 mg for sale
A philosophy of the profession that grounds the ethics of the professions is therefore more than an idle academic exercise prehypertension during third trimester best order for altace. He distin- guishes among four themes bearing on the nature of the good: (1) “the pa- tient’s concept of ultimate good arrhythmia 101 buy 5 mg altace amex,” (2) “biomedical or techno-medical good arteria thyroidea ima buy altace online now,” (3) “the patient’s concept of his own good,” and (4) “the good of the patient as a person. He draws as well from Aristotle’s account of the good, thus estab- lishing connections among the philosophical traditions, understandings of the good, and good clinical decision making. This essay provides a careful analysis of the implications of diferent senses of autonomy for diferent models of the physician-patient relationship. In so doing, Pellegrino lays out cardinal conficts between autonomy and benefcence, and between autonomy and justice. In the process, Beauchamp and Childress’s principles are embedded in the re- alities of clinical decision making, as well as in the foundational scafold- ing of the physician-patient relationship. Rather than principles, we can speak of obligations freely undertaken when we freely ofer to help a sick person. The last essay in this section, “Patient and Physician Autonomy: Con- ficting Rights and Obligations in the Physician-Patient Relationship,” completes the analysis of the healing relationship, as well as of Pellegrino’s critical recasting of the signifcance of Beauchamp and Childress’s four principles. As Pellegrino notes, these principles mark points of strategic tension and ambiguity. Although the principle of benefcence is in tension with autonomy, the physician’s autonomy receives little attention, and the autonomy of medical ethics has come under threat. Pellegrino’s analysis of Beauchamp and Childress’s principles brings him to fve con- clusions: (1) autonomy and benefcence, if rightly understood, turn out to be complementary, not contradictory; (2) in both theory and practice, au- tonomy is not merely a negative but a positive principle as well; (3) the ac- tual content of the principles of benefcence and autonomy is defned in the context of specifc actions and decisions; (4) the physician’s autonomy both as a person and a professional must also be taken into consideration; and (5) medical ethics must maintain its autonomy over against political and socio-economic pressures. The third section of this collection brings together three major essays in which Pellegrino examines the nature of virtue in general, its meaning © 2008 University of Notre Dame Press An Introduction in the medical profession in particular, and moral challenges to the con- science and integrity of physicians. The frst essay, “Character, Virtue, and Self-Interest in the Ethics of the Professions,” confronts the place of pro- fessional virtue and the difculty of contemporary medical professionals recognizing the claims of virtue. Commercialization, competition, gov- ernment regulation, malpractice suits, and advertising, as well as public and media hostility have engendered a profound professional malaise. Pellegrino argues that, though these forces are real and threatening, the major danger is posed by defciencies in medical-professional character and virtue. Medical professionals, in order to maintain their integrity, will need to embrace an ethos of altruism and fdelity that will often be incon- gruent with the dominant, conventional morality. To do this, Pellegrino argues, medical professionals must recognize that professions are moral communities, able to sustain their members if their members sustain their professional moral communities. Success in establishing a sound founda- tion for the professional life requires recognizing (1) the vulnerability of patients, (2) the inequality between physicians and patients, (3) the special fduciary character of the professional in such relationships, (4) the ways in which professional knowledge does not exist for its own sake, (5) the professional relationship as able to bring both help and harm, and (6) the professional relationship as dependent on the professional being a mem- ber of a moral community with its own internal morality. The second of this trio of essays, “Toward a Virtue-Based Normative Ethics for the Health Professions,” invites the reader to confront the mean- ing and foundations of virtue. As Pellegrino reminds us, the classical me- dieval synthesis understood virtue as excellence of character, as a trait appropriately oriented to defning ends and purposes, as an excellence of reason, not emotion, as centered in practical judgment, and as a trait acquired by practice. Pellegrino contrasts this account with Alasdair Mac- Intyre’s account, which regards virtues as dispositions or acquired quali- ties necessary (1) to achieve the internal good of practices, (2) to sustain the communities in which individuals seek the higher good of their lives, and (3) to sustain traditions necessary for the fourishing of individual lives. Despite his defense of virtue ethics, Pellegrino frankly acknowledges the difculties of virtue-based accounts: (1) virtue-based accounts tend to be circular (i. All of this leads Pellegrino to underscore that virtue-based accounts cannot stand alone and must be lodged within a more comprehensive moral phi- losophy, which he acknowledges does not now exist. This problem is com- pounded in medicine, where the Hippocratic tradition is, at best, in dis- array. The practice of medicine is marked by moral pluralism, relativism, and the privatization of morality. In the face of these challenges, Pellegrino calls physicians to an act of profession that can tie them to their engage- ment in healing, so that they can come to appreciate professional virtue in terms of the telos of the clinical encounter: the patient’s good. Pellegrino lists among the virtues that should mark the good physician: fdelity to trust and promise, benevolence, efacement of self-interest, compassion and caring, intellectual honesty, justice, and prudence. Having spoken to professional virtue in the clinical context, Pel- legrino turns in the next essay to challenges to the physician’s moral con- science. His focus is on the conficts engendered as a result of practicing medicine in an often afrmatively secular culture. This tension is rooted in the circumstance that traditional Christians know things about medical morality unrecognized within secular society. In “The Physician’s Con- science, Conscience Clauses, and Religious Belief: A Catholic Perspec- tive,” Pellegrino lays out a geography of some of the resulting moral conficts, giving special attention to the rising reluctance of the state and others to confront honestly what should count as violations of conscience.
Generic altace 2.5 mg with amex
Guidelines have already been developed [2 blood pressure basics altace 2.5 mg buy with amex, 4] and recommendations are available [5] arrhythmia guidelines 2014 buy altace online from canada, but work still has to be done pulse pressure guidelines purchase generic altace pills, in the near future, to practically improve radiation protection in operating rooms. Moreover, special attention should be paid to procedures performed on children, especially at the bedside and in dental radiology. Radiation protection is vital for all procedures performed under fluoroscopy guidance, including those performed in the endoscopy suite. Radiation protection in the endoscopy suite should follow published guidelines from the International Commission on Radiological Protection and the World Gastroenterology Organisation, which specifically address the issue of radiation protection for fluoroscopically guided procedures performed outside imaging departments and in the endoscopy suite. Recent studies have examined the issue of lifetime cumulative effective doses received by patients attending hospital with gastrointestinal disorders and have shown potential for substantial radiation exposures from gastrointestinal imaging, especially in small groups of patients with chronic gastrointestinal disorders such as Crohn’s disease. In these patients, radiation dose optimization is necessary and should follow the principles of justification, optimization and limitation. Currently, there are increasing numbers of medical specialists using fluoroscopy outside imaging departments and the use of fluoroscopy is currently greater than at any time in the past. This is partly explained by lack of education and training in radiation protection in this setting, and can result in increased radiation risk to patients and staff. Radiation protection and fluoroscopy facilities separate from radiology departments The extent of the problem with radiation protection in endoscopy suites can vary greatly from one jurisdiction to another [1, 2]. In some countries, there is no database of fluoroscopic equipment located outside radiology departments. As a result, staff in endoscopy suites need enhanced radiation protection education and need to routinely utilize radiation protection tools (e. There is huge variation, between institutions and between countries, in the level of involvement of radiologists and medical physicists in radiation protection for endoscopic procedures. Potential risk areas In some hospitals and in some jurisdictions, there may be a lack of radiation protection culture, with a paucity of patient and staff dose monitoring [1, 2]. There may be poor quality control of fluoroscopic equipment with risk for incidental accidental high exposures or routine overexposures affecting patients and staff. Poor radiation shielding, including lead flaps and poor maintenance of radiation protection equipment, can also be associated with additional risks. Radiation dose to patients in endoscopic procedures Shielding systems to protect staff should be optimized to reduce dose, but must not interfere with performance of clinical tasks. Scheduled periodic testing of fluoroscopic equipment can provide confidence in equipment safety [1, 2]. Equipment factors — Under-couch tubes reduce scattered radiation and exposure to operators, staff and patients. Image hold and image capture options also represent very important features of modern fluoroscopy which can reduce dose and should be used where feasible. Procedure related factors There are many important steps which can be taken to reduce radiation exposure, including the careful use of collimation to reduce area of exposure, limiting the number of radiographic images, using magnification only when really necessary and avoiding steep angulations of the X ray tube [1, 2]. The X ray tube should be as far as possible and image receptor as close as possible to the patient. In addition, the radiation field should be limited carefully to the parts of the body being investigated. Staff doses at endoscopic retrograde cholangiopancreatography Average effective doses of 2–70 μSv per procedure have been reported for endoscopists wearing a lead apron [1, 2]. Lead aprons provide protection; however, there can be substantial doses to unshielded parts such as the fingers and eyes. Use of ceiling mounted shielding, and lead rubber flaps mounted on pedestals that are mobile, should be mandatory and staff should be educated in how to use them effectively. Procedures performed by highly experienced and trained staff usually result in much lower patient and staff exposures — every 10 years of experience has been reported to be associated with 20% reduced fluoroscopy time. There has been continued high utilization of plain radiographs, in spite of the fact that other studies have questioned the diagnostic value of these studies and their ability to influence patient management [3]. Small groups of patients (and especially subgroups of Crohn’s patients) can be exposed to substantial cumulative effective doses of ionizing radiation [3]. In addition, limiting the use of plain abdominal radiography in Crohn’s disease and other chronic gastrointestinal disorders should be considered, as performance of these studies usually has little impact on patient management.
Syndromes
- Blood culture
- Testing can be done at home and with little training. For example, persons with diabetes must check their blood sugar several times a day using capillary blood sampling.
- Abdominal pain, changes in bowel movements, or weight loss
- Joint x-rays
- Blood clot in the lung
- The amount swallowed
- Change in skin color (pallor)
- Thick, coarse facial features with low nasal bridge
- Hot and spicy foods or liquids
- The blisters break, forming small sores that begin to dry and form crusts. The crusts fall off in 2 to 3 weeks. Scarring is rare.
Buy generic altace 10 mg on line
Some deci- husband heart attack enzyme test generic 5 mg altace mastercard, but this desire now appears to be in confict with the sions arise automatically on the basis of experience blood pressure medication harmful buy 10 mg altace mastercard. This demands of her new position as medical director of a large usually works well arteria dorsalis nasi order altace canada, but from time to time life throws us a hospital-based program. Susan has become short-tempered curve ball, destabilizes us, and causes us to experience stress and feels increasingly dissatisfed with her professional and or even distress. In speaking with a friend, she realizes that she is helpful to “check in” with our values and beliefs. This means living life the way her parents did, and is deeply ashamed of her being able to identify and defne our core values, to explore career choices. After refecting on her core values, she resigns and challenge our own belief systems, and to be open to new her administrative position and fnds more time to spend with understanding. And so her value confict, although painful, proves going by knowing where we have been. Values Values are complex, often abstract cognitive structures that Beliefs shape our behaviour, give us motivation and drive, defne our Beliefs are the cognitive structures we use to guide us through world view and help us determine what is important in life and the world. Beliefs or “cognitions” have a powerful our beliefs, which are generally somewhat in fux until they infuence on our mood, our ability to initiate and maintain become solidifed as “knowledge. Sometime we if we view new information as credible, reasonable and of entertain distorted beliefs that hold us back from achieving value. This allows us to be open and fexible—traits that help our goals and even from living our lives in line with our value us cope with new stressors and situations. For example, physicians may be prone to “impostor our beliefs can be so profoundly affrmed and validated that syndrome,” a distorted belief that they are not as competent as they become infexible convictions. When rigid beliefs fail to the world perceives them to be, that they are at constant risk help us in times of stress, we are faced with a challenge similar of being “found out,” and that they must put great effort into to value-based confict. Some other, similarly damaging beliefs beliefs that are not based on fact or evidence (e. If the feedback isn’t in keeping with our beliefs, it and others from one role to another. For example, feeling can precipitate a crisis of identity, security and confdence. Yet it is more likely that we have a variable sense of self in our roles, particularly Identify three or four people who love you and whom roles that are new, novel or in fux. Then ask two or three questions, The fellow likely generalized their sense of success from such as their professional life to their personal life, and seems to • How is our relationship going? What do we do have believed that both situations were stable and suc- that is really great and what do we need to work cessful. How do you think my life—my career being just one part it— Talking about feelings, identifying goals and sharing honest is going right now? What are your top three ideas and opinions helps to sustain spousal relationships. In the absence of sharing, assumptions will be created that might not be accurate. At this stage, the fellow and spouse Then give the person time to refect and get back to you. Avoid saying mediate situation, determine if they want to maintain the “but” or “maybe. Say thank you and then relationship, and—if so—begin the process of repair and refect carefully on the comments. See if you can develop a routine of “checking in” with your friends and loved ones. The refective cycle proposed by Gibbs in 1988 comprises the following stages: Case 1. Feelings: What were you thinking and feeling during slowly injecting an intravenous medication that ought to be the event? Evaluation: What was positive or negative about the the nurse has more practice experience. We learn, by observation fnd it helpful to use as a framework while engaged in a physi- or instruction, how we prefer to behave in particular types of cal activity (e.
Order altace cheap online
Polystyrene boxes within cardboard boxes are useful for their insulating and shock absorbing properties heart attack iglesias best buy altace. If polystyrene boxes are not available pulmonary hypertension 50 mmhg 5 mg altace order fast delivery, sheets of this material can be cut to fit inside cardboard boxes with a similar effect (though the package is less leak-proof) hypertension 3rd class medical buy generic altace 2.5 mg. The strength of the cardboard box needs to be sufficient for the weight of the package. If hard plastic or metal insulated boxes are used for transport, cardboard boxes around them can be used for protection and to attach labels. It is possible to make ice packs by freezing water inside a plastic bottle that is sealed (not filled completely and taped closed to prevent the top coming off in transit) and then placed in a sealed plastic bag to further prevent leakage. If frozen carcases are being transported they can act as a cool pack for other samples sent in the same container. When using ice packs they should be interspersed between samples to achieve a uniform temperature throughout. When submitting dead fish for post mortem examination they should be wrapped in moist paper to prevent them drying out and then refrigerated but not frozen. Fish decay very quickly but a fish refrigerated soon after death may be held for up to twelve hours before examination and sample fixation. Keeping samples frozen Dry ice (solid carbon dioxide) or in some circumstances liquid nitrogen can be used to ship frozen specimens. The gaseous carbon dioxide given off by dry ice can also damage some disease agents and this must be considered before using it for tissue transport. As the volume of both dry ice and liquid nitrogen expand as they change to gas, specialist containers that allow for this expansion are needed for their transportation. Note: Shipment of formalin, dry ice, liquid nitrogen and alcohol is regulated in many countries and must be cleared with a carrier before shipping. Samples preserved in formalin, other chemical fixative or alcohol can be transported without chilling. Shipping It is important to pack any space within packages with a substance such as newspaper which will prevent movement of containers, act as a shock absorber and may also soak up any potential leakages. Packaging and labelling Packaging and labelling of specimens must conform to the regulations of the country from which the package is sent and also those of the country in which it will be received (if it is being sent to a laboratory in another country). It is important to mark the outside of the package with the required labelling regarding the type of specimen being transferred and where necessary the method of cooling (e. Advice from national authorities about permit requirements must be sought prior to collection and transportation of samples. Carriers Samples should be shipped where possible by carriers that can guarantee 24-hour delivery to the diagnostic laboratory. Where possible arrange for collection of sample packages from the point of origin to avoid delays. When shipping arrangements have been made, contact the diagnostic laboratory to provide them with further details including estimated time of arrival and any shipping reference numbers. Chapter 3, Field manual of wildlife diseases: general field procedures and diseases of birds. Detailed field observations during the course of an outbreak and information about events preceding it, may provide valuable data on which to base a diagnosis and corrective actions. It is important for the information gatherer to keep an open mind about the potential cause of the problem. Some information which may seem irrelevant in the field may become very important when piecing together the events leading up to an outbreak. A thorough chronology of events is key to diagnosis and disease control operations, and is almost impossible to obtain some time after the outbreak has occurred. A key concept is that of explaining to the diagnostician how the affected individuals relate to the whole population at risk. As an example, 100% of the dead animals may be adult males but the population present (i.
Generic altace 5 mg amex
The internal jugular vein is most easily seen with the pa- tient reclining (usually at 45˚) arrhythmia medication discount altace, with the head supported Cyanosis and the neck muscles relaxed and in good lighting con- Cyanosis is a blue discolouration of the skin and mu- ditions arrhythmia can occur when altace 10 mg overnight delivery. It is due to the presence of desaturated toid muscle in the upper third of the neck hypertension patient teaching purchase altace 2.5 mg free shipping, behind it haemoglobin and becomes visible when levels rise above in the middle third and between the two heads of ster- 5 g/dL. Cyanosis is not present in very anaemic patients nocleidomastoid in the lower third. Cyanosis is divided from the carotid pulse by its double waveform, it is non- into two categories: palpable, it is occluded by pressure and pressure on the r Peripheral cyanosis, which is seen in the fingertips and liver causes a rise in the level of the pulsation (hepato- peripheries. The jugular waveform and pressure give it is due to poor perfusion, as the sluggish circulation information about the pressures within the right atrium leads to increased desaturation of haemoglobin. This as there are no valves separating the atrium and the in- may be as a result of normal vasoconstriction in the ternal jugular vein (see Fig. It is a result of failure of 3cmrepresents an abnormal increase in filling pressure Chapter 2: Clinical 27 Normal The normal pulsation has a rapid rise in pressure followed by a slower phase or reduction in pressure. Slow rising The slow rising pulse is seen in aortic stenosis due to obstruction of outflow. Collapsing The collapsing pulse of aortic regurgitation is characterised by a large upstroke followed by a rapid fall in pressure. This is best appreciated with the arm held up above the head and the pulse felt with the flat of the fingers. Alternans Pulsus alternans describes a pulse with alternating strong and weak beats. Bisferiens This is the waveform that reults from mixed aortic stenosis and regurgitation. The percussive wave P T (P) is due to ventricular systole, the tidal wave (T) is due to vascular recoil causing a palpable double pulse i. Paradoxus This is an accentuation of the normal situation with an excessive and palpable fall of the pulse Inspiration pressure during inspiration. Once the atrium is filled with blood it contracts to give the ‘a’ wave a The ‘a’ wave is lost in atrial fibrillation. The ‘a’ wave is increased in pulmonary stenosis, pulmonary hypertension and tricuspid stenosis (as a consequence of right atrial or right ventricular hypertrophy). The atrium relaxes to give the ‘x’ descent; however, the start of a ventricular contraction causes ballooning of the tricuspid valve as c it closes, resulting in the ‘c’ wave. The further ‘x’ descent is due to descent of the closed valve towards the cardiac apex. This may occur in right-sided heart Timing to systole or diastole is achieved by palpation failure, congestive cardiac failure and pulmonary em- of the carotid pulse whilst auscultating. Murmurs are further described according to their Precordial heaves, thrills and pulsation relationship to the cardiac cycle. Thisoccursinmitralregurgitation, ventricular hypertrophy when the impulse is at the tricuspid regurgitation and with a ventricular septal same time as the apex beat and carotid pulsation. It is heard r A thrill is a palpable murmur and is due to turbulent with aortic stenosis, pulmonary stenosis and with an blood flow. For example, a diastolic thrill at r A late systolic murmur is heard in mitral valve pro- the apex is suggestive of severe mitral stenosis (aortic lapse. This is most tercostal space) and the relationship to the chest (mid- helpful when the flow of blood is considered according clavicular line, anterior axillary line, etc). The normal to the lesion, for example aortic stenosis radiates to the position is the fourth or fifth intercostal space in the neck, mitral regurgitation radiates to the axilla. Investigations and procedures Heart murmurs Coronary angioplasty Heart murmurs are the result of turbulent blood flow. Coronary angioplasty is a technique used to dilate stenosed coronary arteries in patients with ischaemic heart disease. These slowly disease or triple vessel disease to be treated by bypass release a drug (e.
Buy discount altace line
The student will be allocated an individual tutor/ supervisor based at the University of Edinburgh blood pressure medication images order altace with paypal, and we would aim to find people with appropriate specialist interest in the areas required blood pressure chart heart.org cheap altace 10 mg. Candidates will however be encouraged to work closely with senior staff in their home institutions hypertension images purchase altace us, with mutually beneficial fostering of suitable academic links between the University of Edinburgh and medical institutes worldwide. The submission of the thesis (as per University regulations) on an agreed topic must normally be within 36 months of initial registration. Requests for an extension to the period of study must go through the Programme Director as a formal request to the College Postgraduate Studies Committee. Forms for this purpose, and for ‘interruption of studies’ due to special circumstances, are available from the course organizer. The final thesis will be in two forms: a printed document that will be marked and lodged in the university library, and an electronic version which will be set in the course archive for reference by future students. Students must ensure that their submitted dissertation meets the following criteria: 15,000 words or less (excluding references) A4 portrait format with appropriate margins Easily-readable font and font size (e. Progression and distinction Candidates gain the given number of credits required for a degree award incrementally in each academic year. Credits required are as set out in the Scottish Qualifications Framework and incorporated into the University’s Curriculum Framework. Progression on the programme is dependent on satisfactory performance at each level of the award. Students may choose to graduate after one year with a postgraduate certificate (60 credit points), or after the second year (120 credit points) entitling them to a postgraduate diploma. Year 1: During the first year, the student is required to complete (to the satisfaction of the Board of Examiners) all compulsory modules (with the option of replacing the Science of Medicine course with two elective modules from year 2). On satisfactory completion of year 1, they can leave the programme with a Certificate in Internal Medicine, or progress to the second year. All students who obtain a mark of greater than or equal to 40% are entitled to progress into the diploma year. Individuals failing to attain this grade will be deemed to have failed the programme. Students who fail their second year will leave the programme at this point with the award of a postgraduate certificate having attained sufficient credits for this award during their first year. Year 3: Students who achieve 50% or more in the master’s dissertation will be entitled to graduate with a master’s degree. Individuals who fail to achieve 50% will leave the course with the award of a postgraduate diploma. Students who achieve a mark of at least 70% on all courses on the programme will be awarded a master’s with distinction. This programme will adopt progression criteria in accordance with the University’s regulation should they change (we understand that these are being reviewed currently and are awaiting formalisation). The 20-credit Science of Medicine course will have double the weighting to the other 10-credit modules. Taking this into account, the assignment marks in each year will aggregated by averaging. Sufficiently high marks must be achieved at the first sitting in the first year (certificate) to allow progression to the second year (diploma) (see above). The diploma will be marked by two Internal Examiners with quality assurance and check-marking by the External Examiner. The provisional marks and marker comments will be discussed by the Board of Examiners and a decision taken as to the mark awarded and feedback to be given to the candidate. Only one submission of a dissertation (or any of the other assignments) is permitted. Note that major correction and resubmission is not permitted under University regulations (see below). Students achieving at least 70% (Grade A) for the dissertation and an average close to 70% for the rest of the assignments will be awarded ‘master’s with distinction’. For those electing to leave the programme after two years with a diploma, an average assignment mark of 70% or more will earn the award of ‘diploma with distinction’.
Generic altace 10 mg on-line
These substances are also referred to as psychoactive drugs blood pressure medication recall buy altace 10 mg overnight delivery, meaning that they affect the central nervous system and alter mood arteria gastrica sinistra purchase cheap altace online, thinking hypertension xray cheap 10 mg altace with mastercard, perception and behaviour. Blanket definitions which attem pt to cover these areas as well as the substance/user/affect nexus often have weak logic underpinning their m eanings, m aking them vulnerable to challenge, particularly in term s of highlighting inconsistencies. For exam ple, if alcohol and tobacco are not defined as drugs, what does that say about adult society which approves and endorses their use, (m indful of the health and social costs they can both incur) but disapproves of the use of cannabis and ecstasy by young people? Once a broad, working definition of drugs has been established, one is better placed to discuss the health, personal and social costs arising from substance use. This does not m ean that the legal status of any drug is not im portant; rather, it acknowledges that the risks arising from drug use are not present exclusively in relation to the crim inal/justice system. Drug Use Drug use is a broad term to cover the taking of all psychoactive substances within which there are stages: drug-free (i. Drug Misuse Substance misuse is defined by the Royal College of Psychiatrists as “… any taking of a drug which harms or threatens to harm the physical or mental health or social well-being of an individual or other individuals or society at large, or which is illegal. The notion of addiction to a wide range of substances and behaviours is now firmly embedded in our cultural outlook. However, increased usage of the terms has not automatically ensured an increase in the level of understanding of the process of dependence. Abuse Substance abuse is described as a: ‘maladaptive’† pattern of substance use leading to clinically significant im pairm ent or distress, as m anifested by one (or m ore) of the following within a 12 m onth period: 1 Recurrent use leading to failure to fulfil major role obligations (work, home, school, etc. Responses to young people’s drug use which are couched in adult understandings of adult drug m isuse/dependence and see young people’s drug use from such a perspective are not only unlikely to m eet the needs of young people but are also unlikely to work. The following section looks at the factors involved in the different stages of drug use and specifically the different types of drug use som e young people m ay typically experience. If our responses to drug use are to be effective, they have to be em bedded in this understanding. The diagram presents a sim plified m odel of the different stages or levels of drug use, starting with a Drug Free stage. The reality is that we live and, as drug educators, work in an environment where drug use is an intimate part of our culture. Putting illicit drug use to one side, tea, coffee (both containing the stimulant substance caffeine), tobacco, over the counter and prescribed medications and alcohol are prevalent throughout our homes, work and social domains in a myriad of forms with equally diverse uses. This has an impact on young people from birth and throughout their childhood and adolescence – long before we start to directly and formally address drugs education issues with them. With this in mind, the drug free state can be primarily regarded as an idealised one. It is presented to dependent drug users as an indication of where they should aspire to be (and how different their world would be if they were not using drugs). It may also come about as the result of a conscious decision to abstain from drug use. However it rarely refers to all substances contained within the definition of ‘drugs’. Patterns of Adolescent Drug Use Several different patterns of young people’s drug use have been identified, mainly centred around experimental and recreational use:6 y Exploratory or Experimental Use y Social Use y Emotional or Instrumental Use, which has two different strands: Generative or Hedonistic Use Suppressive or Compensatory Use y Habitual Use y Dependent Use Exploratory Or Experimental Use The experimental stage of drug use is a short-term, learning phase, influenced by culture and availability and characterised by: y peer group activity y random choice of drugs Within an Irish context, young people’s experimentation with drugs will often feature alcohol and/or tobacco, given their prevalence and the ease of access to them. Availability (particularly alongside curiosity), anticipation of effects, youth culture and current fashions regarding substance use each play a role in young people’s experimentation with drugs. For the majority of people, experimentation is confined to those drugs which are socially acceptable. Experimentation with substances does not automatically lead onto recreational drug use or, indeed, dependent use and may cease once the initial motivating factors have been satisfied. The following characteristics of experimental use have been identified: y Curiosity and risk taking are deemed the primary motive y Mood altering effects are secondary to the ‘adventure’ of drug use itself y The young people may try more than one substance but usually not more than a few times. As with any drug use by young people, experimental use can be an enormous source of concern; but Morgan (2000) notes that: “… risk factors are not always negative in nature, especially in the case of experimental drug use. This is illustrated in a longitudinal study by Shedler and Block (1990) who collected information on personality and adjustment from five years upwards. Their results showed that, at least in the American context of the time, those adolescents who engaged in mild experimentation with cannabis were relatively better adjusted (less anxious particularly) than those who had never experimented while frequent users were the least well adjusted. This phase is characterised by: y regular use y group activity y use over a longer period of time 12 Stages of Drug Use The key here is that control is exerted over use, with specific choices being made in relation to what drugs are used, in what amount, where they are used (normally in specific situations) and when. As users become schooled in what drugs give the effect they desire in different situations, their substance use develops a degree of predictability and, generally, is not perceived to be problematic.
Rasul, 47 years: Reproducibility of the variations between humans in the response of serum cholesterol to cessation of egg consumption.
Basir, 52 years: The urine is obtained and administered prior to the principal meals against which it is providing protection.
Lukar, 45 years: Although many resources have been allocated to the setting up of referral guidelines/appropriateness criteria by various national radiological societies, institutions and commissions [4–6], more efforts to address this gap are required, through understanding the issues behind the failure of proper justification and increased awareness through education.
Sancho, 50 years: Targeting vectors in integrated disease control strategies can be effective and usually take the form of environmental management, biological controls and/or chemical controls, or actions to reduce the contact between susceptible hosts and vectors.
Carlos, 32 years: The tumour can present with obstruction, recurrent r no malignant pleural effusion.
Asam, 43 years: This is obvious when one group of subjects is chosen from members of a health club, has higher average education, or is from other groups that might intrinsically be more health-conscious than the average person.
Cole, 35 years: Modern medical science has supplemented this range of methods with imaging techniques, e.
Altus, 59 years: Take tartar and [break] it into little bits, and wrap it in a new piece [of cloth] and dip it in strong vinegar so that it be- comes thoroughly soaked, and then let it be placed on the fire until it turns to coals.
Milten, 31 years: The continued role of pharma- cogenomic screening is evident through its association with key drug-metabolizing pathways.
Denpok, 46 years: The first set of definitions defines validity by the process with which it is determined.
8 of 10 - Review by F. Jens
Votes: 45 votes
Total customer reviews: 45
References
- Katayama A, Mafune K, Tanaka Y, et al. Autopsy findings in patients after curative esophagectomy for esophageal carcinoma. J Am Coll Surg 2003;196(6):866-873.
- Bernard EO, et al. Ibutilide versus amiodarone in atrial fibrillation: a double-blinded, randomized study. Crit Care Med 2003;31:1031-1034.
- Whiteway J, Morson BC. Elastosis in diverticular disease of the sigmoid colon. Gut 1985;26:258.
- Ogata M, Mateer JR, Condon RE. Prospective evaluation of abdominal sonography for the diagnosis of bowel obstruction. Ann Surg. 1996;223:237-241.
- Tsang HS, Schoenfeld FG: Malignant hyperthermia. IMJ III Med J 149(5):471-473, 1976.
- Evans DB, Christians KK, Foley WD. Pancreaticoduodenectomy (Whipple operation) and total pancreatectomy for cancer. In: Fischer JE, Jones DB, Pomposelli FB, et al., eds. Fischer's Mastery of Surgery. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2012:1445-1465.
- Somnier FE, Keidling N, Paulson OB. Epidemiology of myasthenia gravis in Denmark: A longitudinal and comprehensive population survey. Arch Neurol. 1991;48:733-739.